1
Patau's syndrome
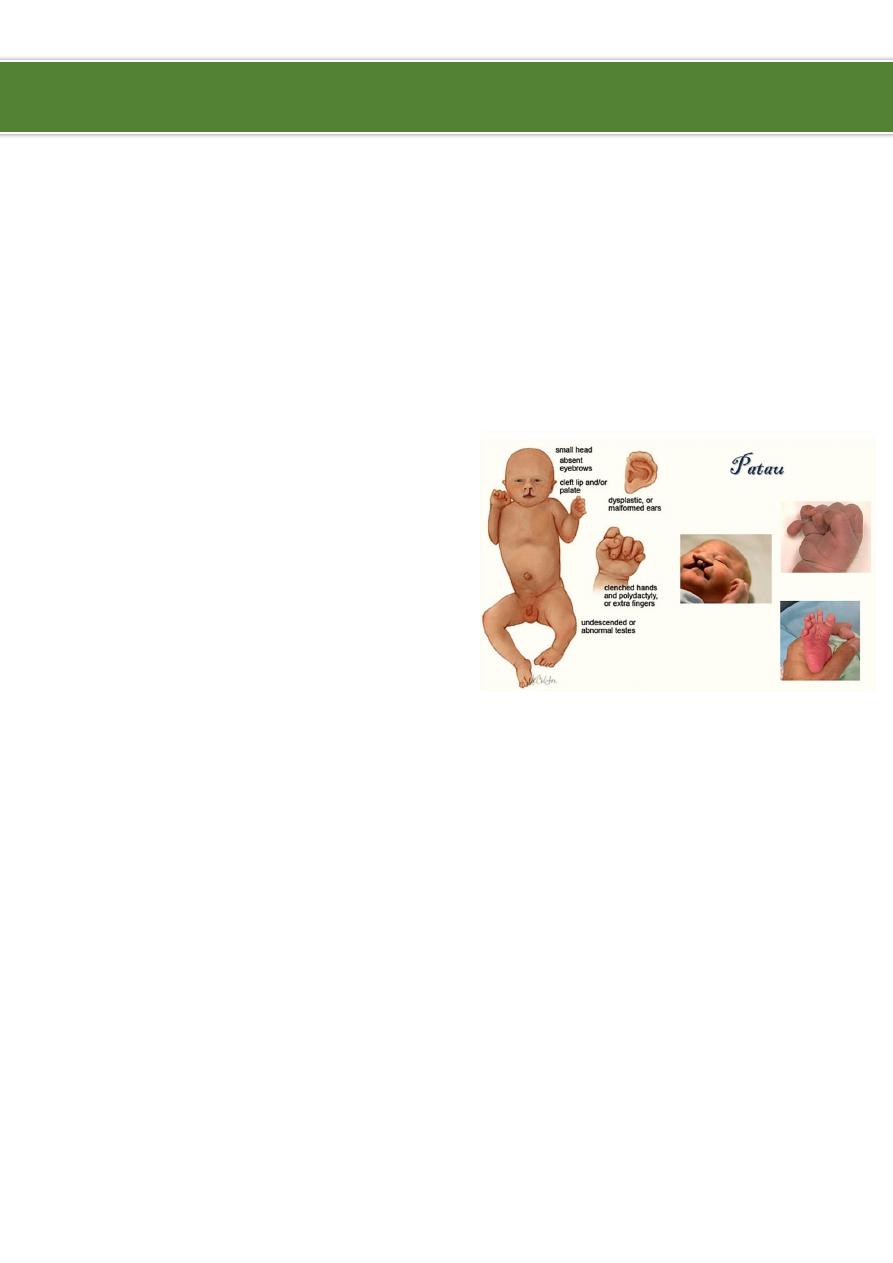
Patau's syndrome (trisomy 13):
Trisomy 13 third of the common trisomies, occurs in 1 in 12,000 live births.
It is usually fatal in the first year of life.
Clinical Features:
SGA.
Structural defect of brain.
Scalp defect.
Microcephaly.
Microphthalmia.
Midline facial defects as single orbit, single
nostril.
Cleft lip and palate.
Polydactyly.
Cardiac and renal malformations.
Management:
Medical Care:
o
All patients diagnosed prenatally with a fetus affected by Patau syndrome
should be
offered a consultation with a care provider skilled in delivering serious
information who is knowledgeable about recurrence risk, screening, and diagnostic
testing options for future pregnancies.
o
Once a diagnosis of Patau syndrome is made, pregnancy management varies
according to the gestational age at diagnosis.
o
Due to the physical stresses of pregnancy compounded by the emotional stress of
carrying a fetus with a lethal condition, or because of the identification of medical
conditions (eg, preeclampsia) that may complicate any pregnancy, labor induction
may be considered.
Ibnlatef
Notes
Pediatrics

2
o
Tocolysis (medical management to reduce uterine contractions) in an effort to
prevent preterm birth is not a reasonable option due to the lethal nature of this
condition.
o
Cesarean delivery for fetal indications is not recommended due to the lethal nature
of this condition.
o
Focused discussions directed at neonatal resuscitation efforts should be held in
advance of labor.
o
When delivery is planned in a hospital setting, labor and delivery nurses, obstetric
care providers, and pediatric and neonatal attendants should be informed of the
patient’s wishes for her child.
o
Pregnancy management of a child with a lethal condition can be complicated by a
lack of available resources.
Surgical care:
o
Surgical interventions are generally withheld for the first few months of life because
of the high mortality rates of babies with Patau syndrome.
o
Carefully weigh decisions about extraordinary life-prolonging measures against the
severity of the neurological and physical defects that are present and the likelihood
of postsurgical recovery or prolonged survival.
Consultations:
o
Referral to a geneticist or genetic counselor is important for appropriate counseling
regarding recurrence risks, etiology, prognosis, and the availability of local area
resources for support.
o
Recurrence risks differ based on the details of the chromosome abnormality and
the mother's age.
o
In general, for freestanding trisomy 13, the recurrence risk for trisomy 13 or
another clinically viable trisomy (ie, trisomy 21, trisomy 18) is approximately 0.5%
above the mother's age-related risk for autosomal trisomies.
o
Recurrence risks for Robertsonian and other structural rearrangements widely vary;
these risks can be as high as 100% in rare cases in which a parental translocation
occurs involving both copies of chromosome 13.
Diet:
o
In a group of 12 survivors with Patau syndrome, 4 were documented as requiring
gavage feeding as newborns, and 7 were bottle-fed.
o
Two children ate and drank with help prior to age 54 months, and feeding by spoon,
finger, and cup was reported.
----------------------------------------------------------------------------------------------
www.facebook.com/ibnlatef
https://goo.gl/RpvNsl