1
Lecture 06 Pathology D. Rasha
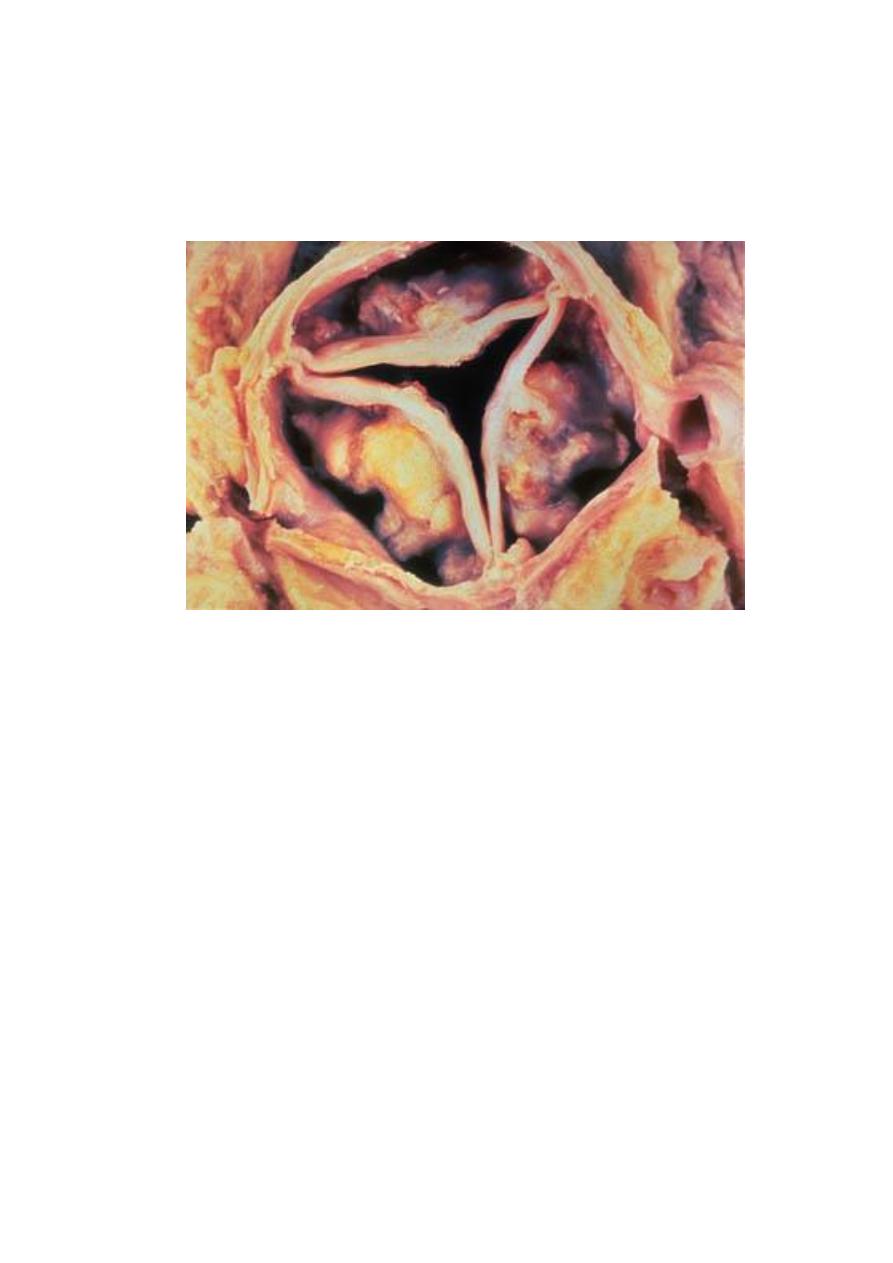
Calcific aortic stenosis:-
This occur due to aging process by degenerative changes with fibrosis of valve leaflets
and calcification, so it's called degenerative calcific aortic stenosis (DCAS).
Mitral valve prolapse:-
It's an isolated mitral regurgitation occur without predisposing heart disease, this
usually discovered between 20 and 40 years, it's characterized by an accumulation
of loose ground substance within the leaflets and chordae of the mitral valve, so
the valve become floppy and incompetent during systole.
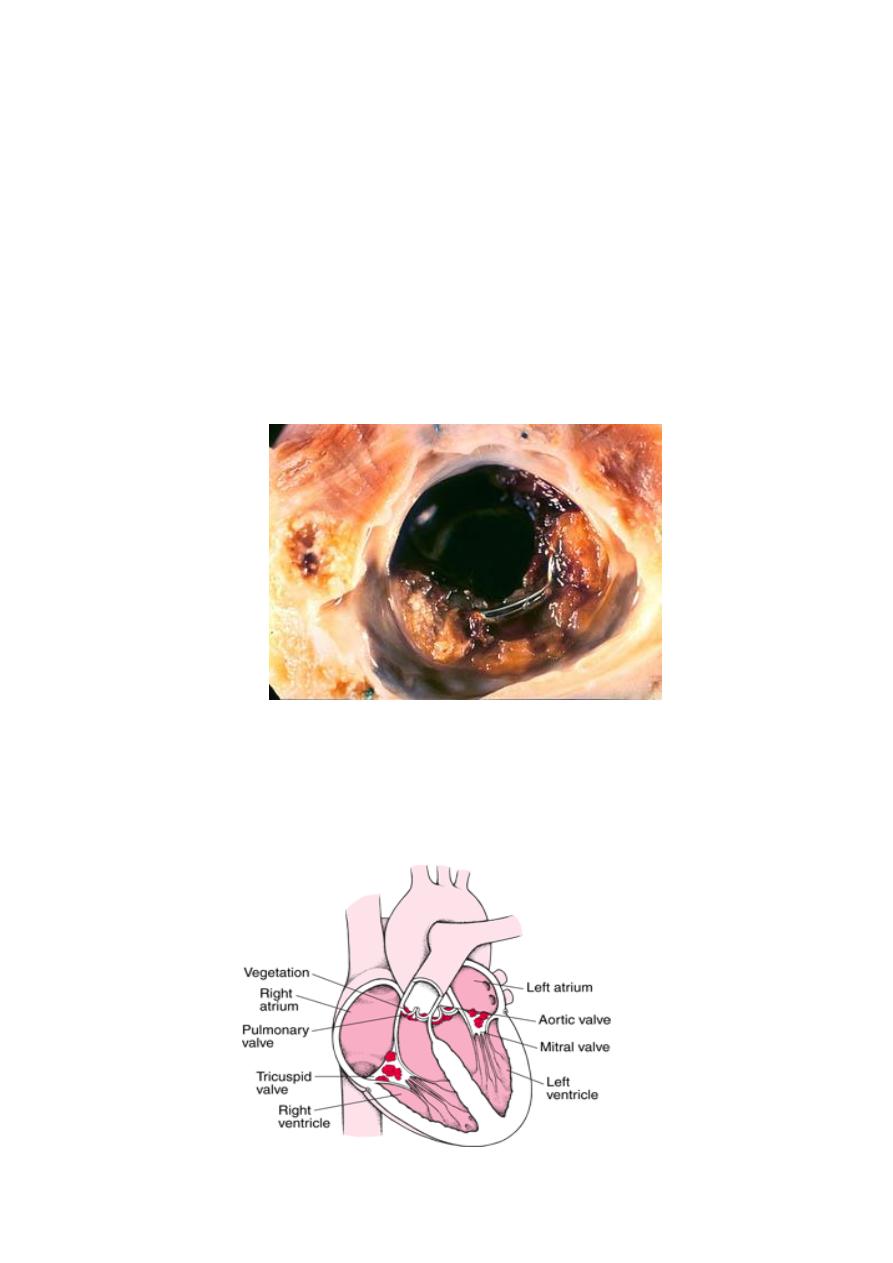
Infective endocarditis:-
It's infection of the cardiac valves or mural surface of the endocardium resulting in
the formation of an adherent mass of thrombotic debris and organism (vegetation).
Infective endocarditis divided into:-
1- Acute endocarditis:-
associated with infection of the valves by high virulent
microorganism as staphylococcus aureus on normal valve and cause rapidly
progressive infection with few local host reaction.
2- Subacute endocarditis:-
associated with infection of previously abnormal valves
by low virulent organisms, such as ά-hemolytic streptococci, the infection tend to
progress slowely and accompanied by the development of a local inflammatory
reaction and granulation tissue in the affected valve.
2
Pathogenesis:-
Infection occur from any microorganism as bacteria, fungi and parasite but bacteria
is the most causative agents, this bacteria found in blood (bacteremia) then
implanted on the endocardial surface, the source of bacteremia usually by
intravenous drug abusers, previous dental, surgical or other procedure.
The most common abnormalities of valve predispose to infective endocarditis are
prosthetic valve, chronic rheumatic heart disease, DACS and mitral valve prolapse.
Infective endocarditis is a particularly difficult infction to eradicate because of the
avascular nature of the heart valves, the inflammatory response to the infection is
relatively scant, so that even a virulent organism can proliferate in uncontrolled
fashion.
Morphology:-
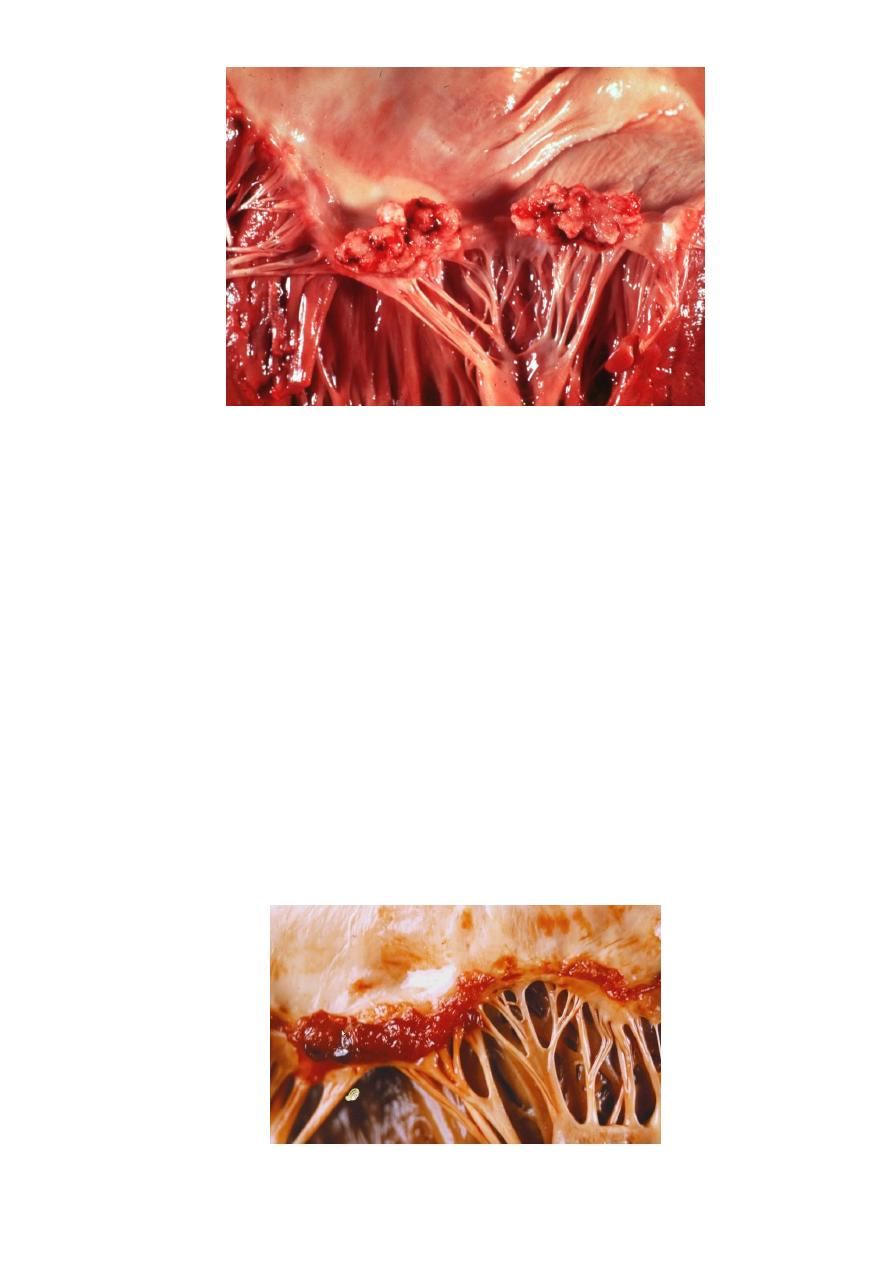
The hall mark of infective endocarditis is the presence of valvular vegetations
containing bacteria or other organisms, the aortic and mitral valves are the most
common sites of infection, the vegetations may be single or multiple and may be
involve more than one valve, seen grossly as small excrescence and vegetation
enlarge to form bulky, friable lesion obstruct valve orifice
3
Microscopically
: show large numbers of organisms admixed with fibrin and blood cells.
Systemic emboli may occur due to friable nature of the vegetations sites, and
abscesses usually develop at the sites of such infarcts because of embolic fragments
contain large number of virulent organism.
Non bacterial thrombotic
endocarditis:
Is characterized by deposition of small masses of fibrin, platelets and other blood
components, on the leaflets of cardiac valves, these valvular lesions are sterile and do
not contain microorganism.
Pathogenesis:-
Endothelial abnortmalities and hypercoagulable states predispose to its development,
this hypercoagulability occur in deep venous thrombosis, malignancies and even occur
in healthy individuals.
Morphology:-
It's appear as group of small nodules on the lined of valve closure and may become
large and friable.
4
Primary myocardial diseases:
1- Myocarditis:-
It's an inflammatory processes of the myocardium that result in injury to the
cardiac myocytes. It's either
secondary
to other heart diseases as ischemic injury,
or
primary
myocarditis which's caused by several types of microorganisms as
viruses, parasites and bacterial infections or may be caused by immune mediated
reactions that cross react with myocardial cells as occur in rheumatic heart disease
Morphology:-
The heart may be of normal size or dilated, the myocardium is flabby and pale with
small areas of hemorrhage.
Microscopically:-
The microscopical changes depend on causative agents but in
general it consists of inflammatory cells infiltrate as lymphocytes, mononuclear
cells and even neutrophils, with degeneration and/or necrosis of myocytes.
Cardiomyopathies:-
Or heart muscle disease, it is heart disease result from a primary abnormality in the
myocardium.
It's divided into 3 major groups:
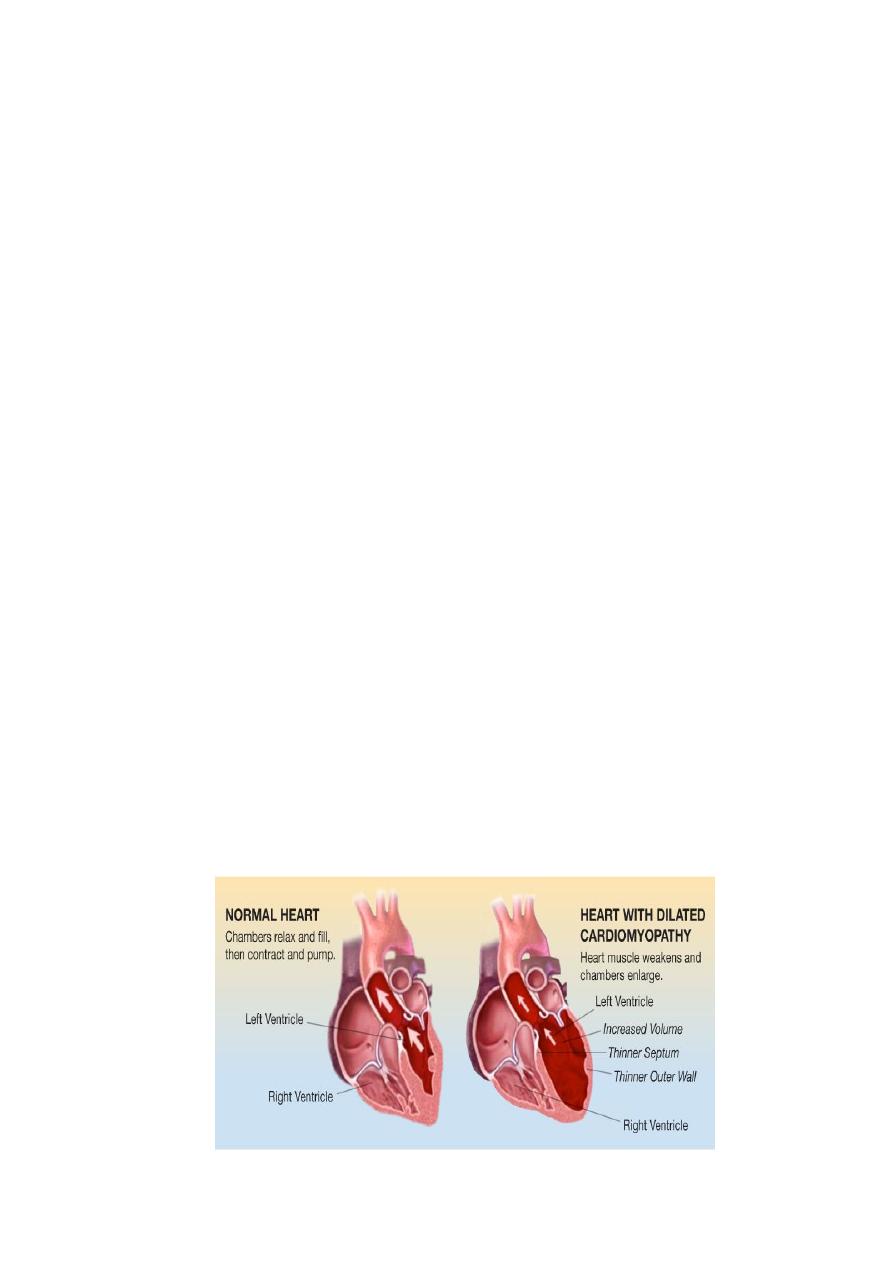
1. Dilated cardiomyopathy:-
It's usually idiopathic but it may be secondary to other causes, it's characterized by
progressive cardiac hypertrophy, dilation and contractile (systole) dysfunction.
Dilated cardiomyopathy occur at any age but it usually common between ages of 20-60
years.
Morphology:-
The heart is enlarged by dilation and hypertrophy of all chambers. The dilation and
poor contractile function cause stasis of blood in cardiac chambers and predispose to
development of fragile mural thrombi and emboli.
5
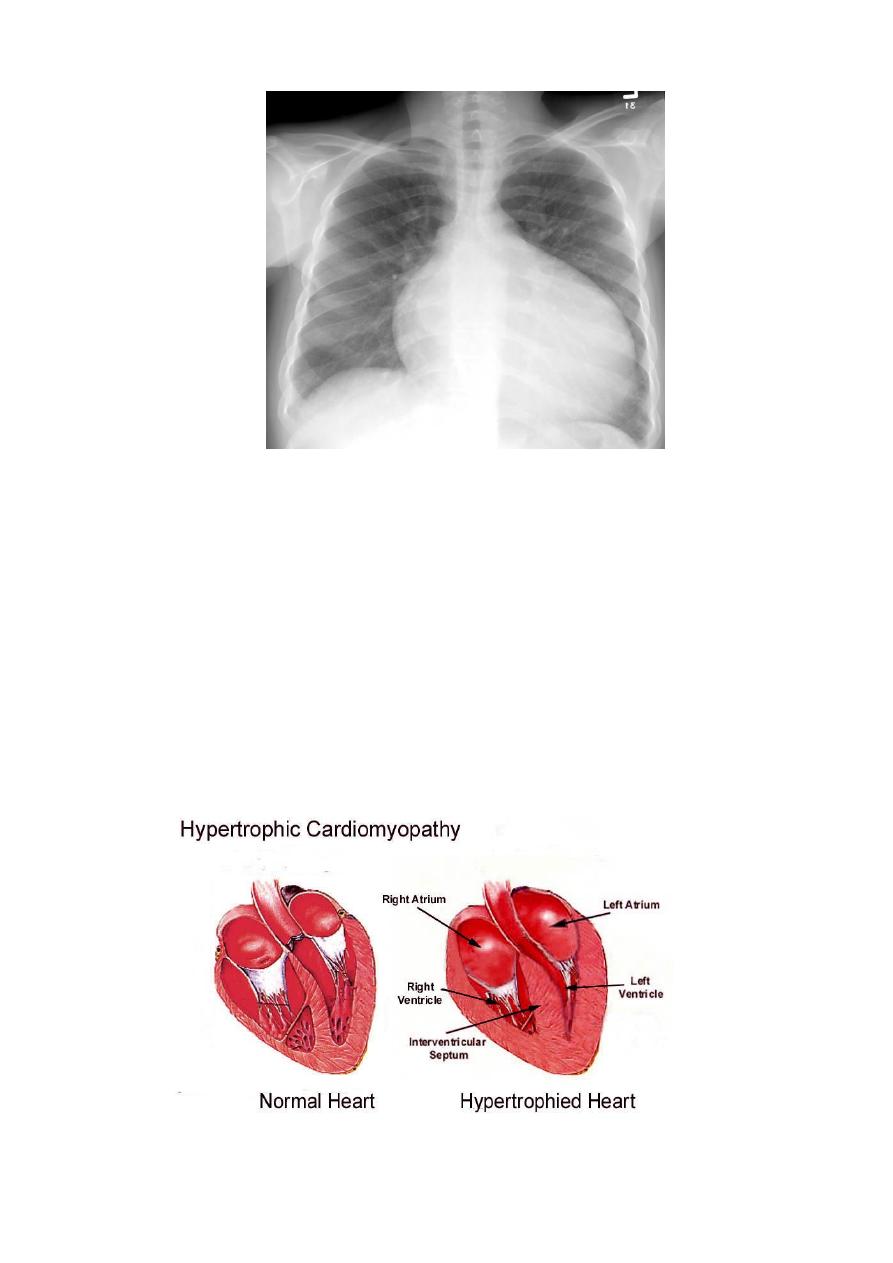
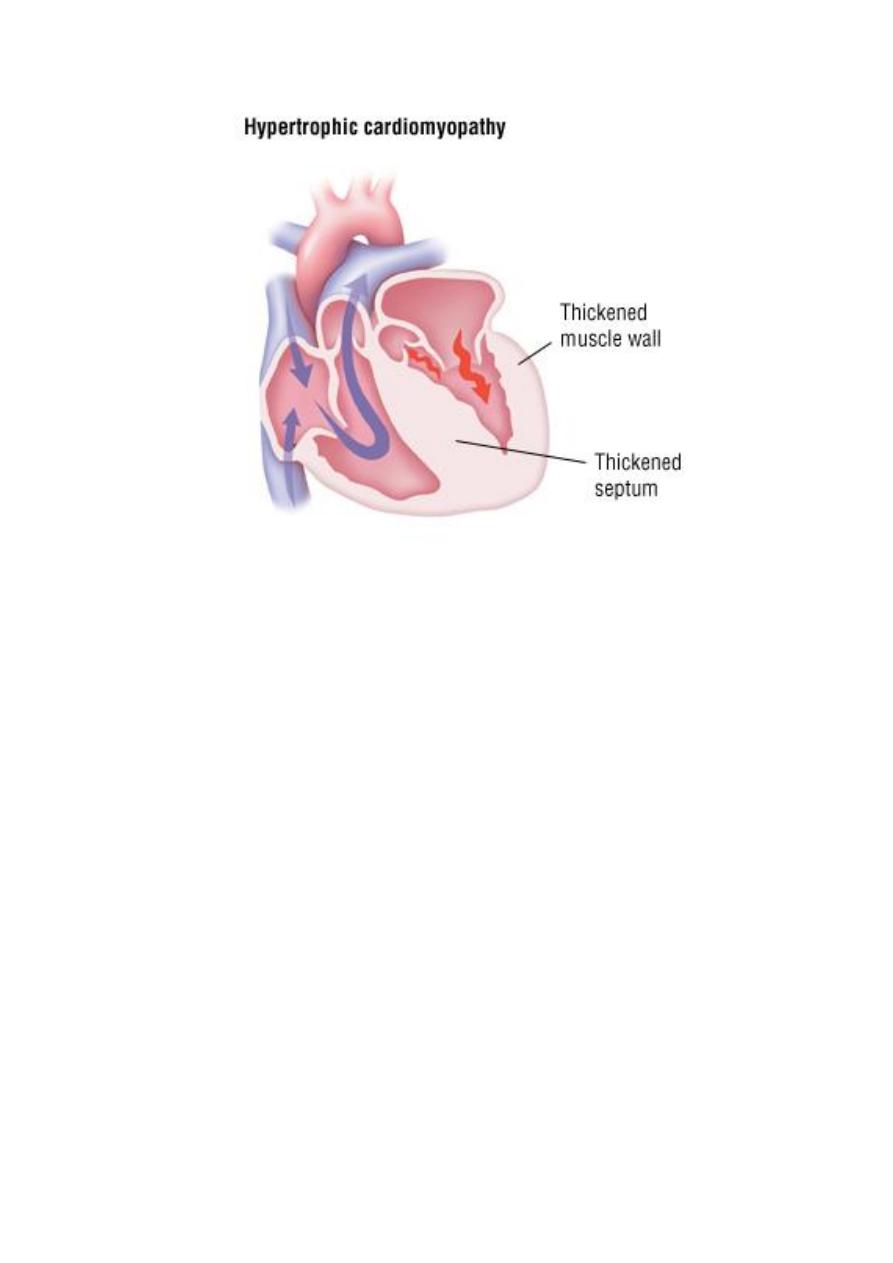
2. Hypertrophic cardiomyopathy:-
It consists of a symmertric septal hypertrophy and idiopathic hypertrophic subaortic
stenosis, it' s characterized by myocardial hypertrophy, abnormal diastolic filling and
intermittent ventricular outflow obstruction.
Morphology:-
The essential feature of hypertrophic cardiomyopathy is myocardial hypertrophy
which's most pronounced in the left ventricle and interventricular septum.
The hypertrophy is usually conspicuous in subaortic region of the septum, so this
asymmetric hypertrophy is often associated with ventricular outflow obstruction
during systole, so it's called "idiopathic hypertrophic subaortic stenosis" .
Ventricular dilation is uncommon but left atrium may be dilated because of impaired
diastolic filling of thickened rigid left ventricle.
6
Restrictive cardiomyopathy:-
It's a disorder characterized by a primary decrease in ventricular compliance,
resulting in impaired ventricular filling during diastole, most common cause of this
decrease of compliance due to endomyocardial fibrosis.