Lec.4
Fetal Development:Determinants of birth weight are multifactorial and reflect the influence of the natural growth potential of the fetus which is affected by fetal genome and the intrauterine environment.
fetal growth is dependent on adequate transfer of the nutrients and oxygen across the placenta, this is also dependent on appropriate maternal nutrition and placental perfusion.
hormonal effects also play an important role of fetal growth like insulin and thyroxin.
Cardiovascular system and fetal circulation:
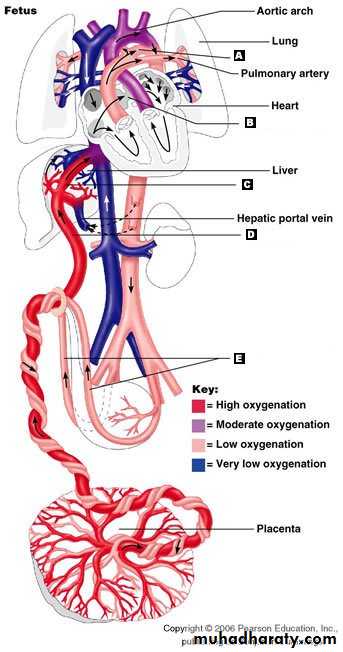
The fetal circulation is quite different from that of the adult. The fetal circulation is characterized by four shunts which ensure that the best , oxygenated blood from the placenta is delivered to the fetal brain and heart.1- Umbilical circulation.
2-Ductus venosus.
3-Foramen ovale.
4-Ductus arteriosus.
The umbilical vein, carrying oxygenated (80% saturated) blood from the placenta to the fetal body enters the portal system
a portion of this umbilical-portal blood passes through the hepatic microcirculation where oxygen is extracted and hence to inferior vena cava
most of the blood bypass the liver through ductus venosus which directly enters the inferior vena cava which also receives the unsaturated venous return from the lower body
blood reaching the heart through the inferior vena cava has an O2 saturation of about 70% which represent the most highly oxygenated blood in the heart
about one-third of blood returning to the heart from inferior vena cava streams across the right atrium mixing with blood from superior vena cava through the foramen ovale into the left atrium
blood flows from the left atrium into the left ventricle and then to the ascending aorta which gives off branches to supply the brain and upper body.
most of the blood returning through inferior vena cava enters right atrium mixes with the unsaturated blood from the superior vena cava enters the right ventricle
right ventricular outflow enters the pulmonary artery and because of the high pulmonary vascular resistance of the pulmonary circulation the blood will bypass the lungs and flow through the ductus arteriosus to the descending aorta
the descending aorta supplies the lower body and the major portion of blood flow goes to the umbilical arteries which carry deoxygenated blood to the placenta.
Changes in the fetal circulation after birth
1-Shortly after birth the umbilical vessels ,ductus venosus, foramen ovali and ductus arteriosus are obliterated.
2- Absence of placental circulation .
3- lung expansion.
4- Reduce pulmonary vascular resistance.
5- the right and the left ventricle work in series.
So the blood that passed to the placenta will be shunted to pass to the pulmonary circulation for gas exchange.
The Fetal Circulation
Factors increasing the oxygen supply to the fetus1- Increase diffusion of oxygen across the placenta.
2- High hemoglobin(Hb) concentration.3- Presence of Hb F which has high affinity to oxygen.
Respiratory system
The lung first appears as an outgrowth from the primitive foregut at about 3-4 weeks.
By 20 weeks the conductive airway tree and parallel vascular tree is well developed.Surfactant production starts from about 30 weeks
It prevents the collapse of small alveoli during expiration by lowering surface tension, it is composed of phospholipid and protein , is phosphatidylcholine ( lecithin ) . inadequate amounts of surfactant result in poor lung expansion and poor gas exchange , results in a condition known as respiratory distress syndrome(RDS).
Numerous , but intermittent , fetal breathing movements occur in utero.
Adequate amniotic fluid volume is necessary for lung maturation
Gastrointestinal system
The primitive gut is present by the end of the 4 th weekand consists of three parts , the foregut , midgut and hindgut.
Peristalsis in the intestine occurs from the second trimester.
at term the large bowel is filled with meconium consisting of intestinal secretion ,dead cells debries.
In utero meconium may pass into the amniotic fluid, This usually occur in post-term pregnancies and fetal hypoxia , aspiration of meconium-stained liquor at birth can result in meconium aspiration syndrome and respiratory distress
Liver, pancress and gall bladder
The pancreas , liver and epithelia lining of the biliary tree derive from the endoderm of the foregut by the third week or early in the fourthBy the sixth week, the liver performs haematopoiesis.
In utero , the normal metabolic functions of the liver are performed by the placenta.
Due to reduced ability to conjugate bilirubin because of relative deficiencies in the necessary enzymes glucuronyl transferase , physiological jaundice are common after delivery .
Glycogen is stored within the liver , maximal in the third trimester. So growth-restricted and premature infants prone to neonatal hypoglycemia.(has low glycogen )
Kidney and urinary tract
The kidney , recognized in its permanent final form ( metanephric kidney) by 4 th weeks
The mesoderm in the thoracolumbar area become epithelial tubules called mesonephric tubules(Wolffian duct) extends towards the most caudal end of the embryo , forming the urinary system in the female and the genitourinary system in the male .
The excretory and the collecting system are completed by the 32-36 weeks of gestation but these structures are not yet mature and the maturation and concentration ability is gradual and continues after birth.
As fetal urine forms much of the amniotic fluid renal agenesis will result in severe reduction or absence of amniotic fluid.
Blood and immune system
Very early red blood cells and immune cells are derived from haematopoietic cells in the yolk sac.By 8 weeks the yolk sac is replaced by the liver as the source of these cells
By 20 weeks almost all of these cells are produced by the bone marrow.
Immunoglobin G (IgG) originates mostly from the maternal circulation and crosses the placenta to provide passive immunity to the fetus and neonate.
Maternal IgM and IgA are not cross the placenta
. Detection of lgM/lgA in the newborn , without lgG , is indicative of fetal infection.
Most haemoglobin in the fetus haemoglobin (HbF ). Which has two gamma-chains ( alpha-2 , gamma- 2 ) . This differs from the adult haemoglobins HbA which have two (alpha-2, beta-2) .
Ninety per cent of fetal haemoglobin is HbF between 10 and 28 weeks gestation.
At term the ratio of HbF to HbA is 80:20;
By six months of age ,only 1 per cent of haemoglobin is HbF.
HbF has a higher affinity for oxygen than HbA.
At birth, the mean capillary haemoglobin is 18 g/dl.
Endocrine system
Major components of the hypothalamic-pituitary axis are in place by 12 weeks gestation.The thyroid gland produces thyroxine from (10 to 12)weeks.
Behavioral status
first activity is the beating of the fetal heart 5-6. weeks followed by fetal movements at 7-8 weeks.
By 12 weeks breathing movement , yawning, sucking and swallowing.