• Shoulder Instability
• By• Ass. Proff.
• Dr. Wahid M. Hassan
DEFINITION:
Glenohumeral instability is the inability to maintain the humeral head in the glenoid fossa.
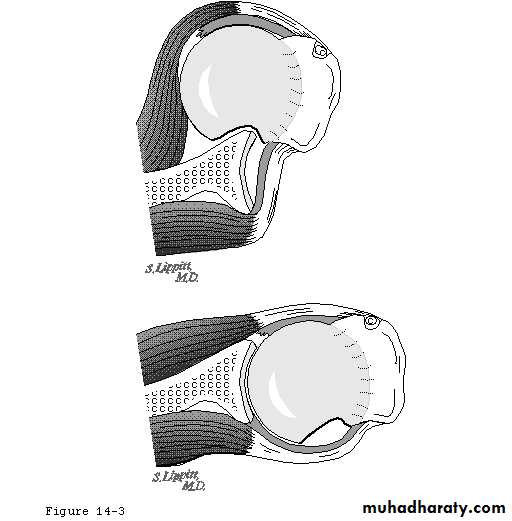
Glenoid Labrum
Static stabilizercontributes 20% to GH stability
fibrous tissue
deepens glenoid(50%), 9mm sup/inf, 5mm AP
3purposes:
increases surface contact area
butress
attachment site for GH ligaments

Biomechanics of GH stability
the normal shoulder precisely constrains the humeral head to the center of the glenoid cavity throughout most of the arc of movement.Static restraints
negative intra-articular pressureligaments and capsule
labrum (increases concavity)
articular surfaces/osseous anatomy
(very little because square area of humeral head is 3X glenoid)
joint fluid adhesiveness
suction cup
limited joint volume
Dynamic restraints
Rotator cuff musclesdeltoid and biceps
concavity compression
Types of instability
CongenitalAcute
Chronic
Recurrent
Traumatic
Atraumatic
Evaluation of recurrent traumatic dislocations
Injury to capsule, rot cuff, labrum, glenoid, humerus.
Young (14-34)
Male
History
HX of 1st dislocation or injurySubsequent dislocations/subluxations
X-RaysIdentify Bankart, Hill-SachsMRIUltrasoundArthroscopy
Diagnosis
TREATMENTRecurrent Traumatic Ant. Dislocation
Surgical stabilization
Open or arthroscopic
Poor response to non operative tx
• Atraumatic Instability
• 80% respond to physio• Surgical stabilization - capsulorraphy if non - operative fails.
TREATMENT
• Voluntary or Habitual
• Retrain muscles
• No surgery
TREATMENT
THE Elbow ,Wrist & Hand: Evaluation and Treatment of Common Disorders
14Tennis Elbow / Lateral Epicondylitis
15
Definition
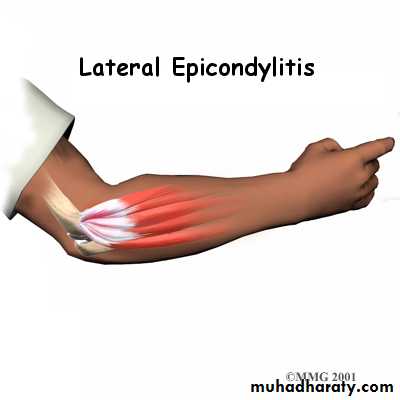
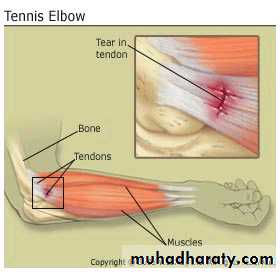
Tennis Elbow Defined:
Tennis elbow is an overuse injury of the elbow joint. It is commonly found in tennis and golf players, especially the “weekend warrior” type. The medical term for tennis elbow is lateral epicondylitis or radiohumeral bursitis
16
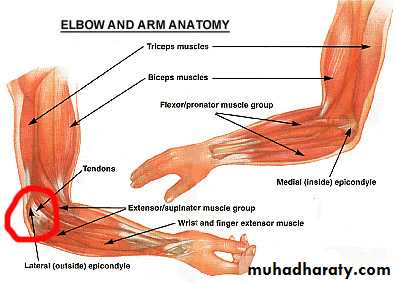
Anatomy
The elbow joint is made up of the following bones, muscles and ligaments.
Humerus, Radius and Ulna.
Bicep and Tricep.
Lateral and medial epicondyle.
Wrist flexor and extensor muscles.
Ulna collateral ligament.
17
A Detailed View of the Elbow
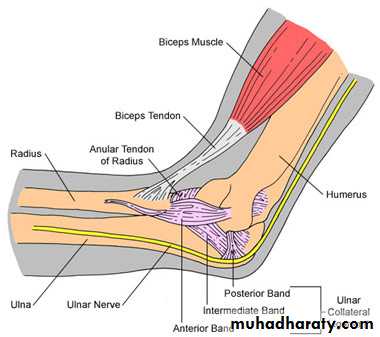
18
How Tennis Elbow Occurs
Tennis elbow is an overuse injury. The most common mechanism of injury is continuous forceful extension of the wrist with pronation of the forearm. This movement is most typically seen in the backhand stroke of tennis and in the downswing portion of a golf swing.

Tendinosis
Mucoid degenerationLoss of collagen tight bundled structure
FibrosisNeo-vascularisation
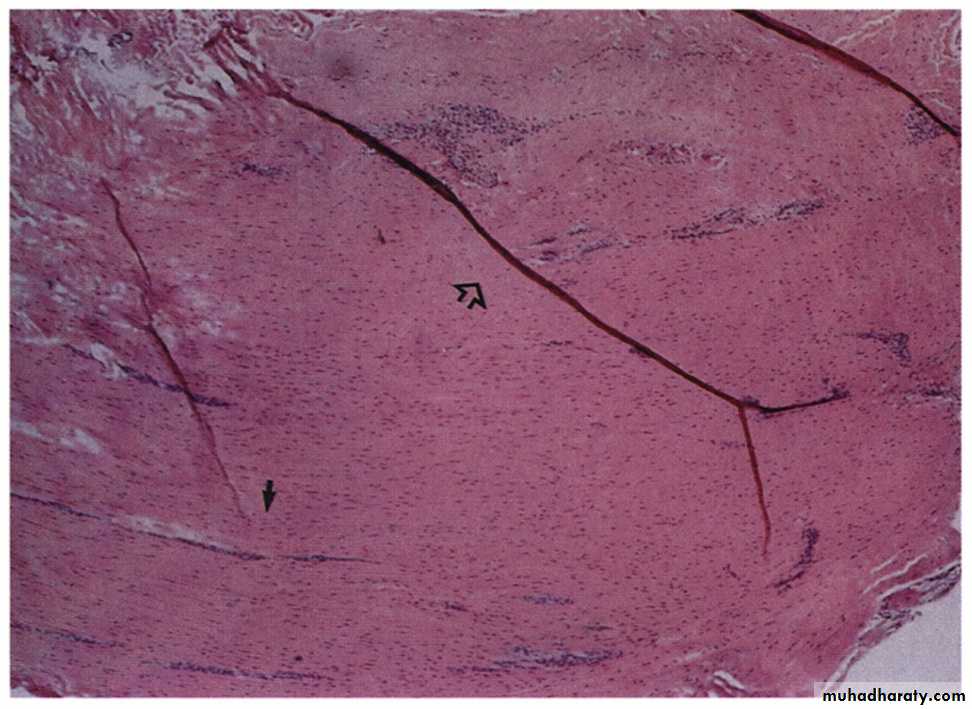
(Khan et al. 1999)
12/24/201620
Prevalence
Tennis elbow is found to have an impact on 1-3% of the general population.
Most commonly affecting men and women from the ages of 40-50 years of age.
However, tennis elbow can still present itself in people of all ages who are not properly condition to perform the activities which will tend to cause this injury. Examples are the weekend golf and tennis players who are not commonly active.
21
Symptoms and Signs
Pain along the lateral epicondyle while performing wrist extension against resistance.
Point tenderness to joint and musculature.
Loss of normal range of motion and function.
Difficulty opening door handles
Difficulty shaking hands

Treatment
Non-operativeRest
NSAIDs
Physiotherapy
Avoid exacerbating activities
USS
Injection therapy
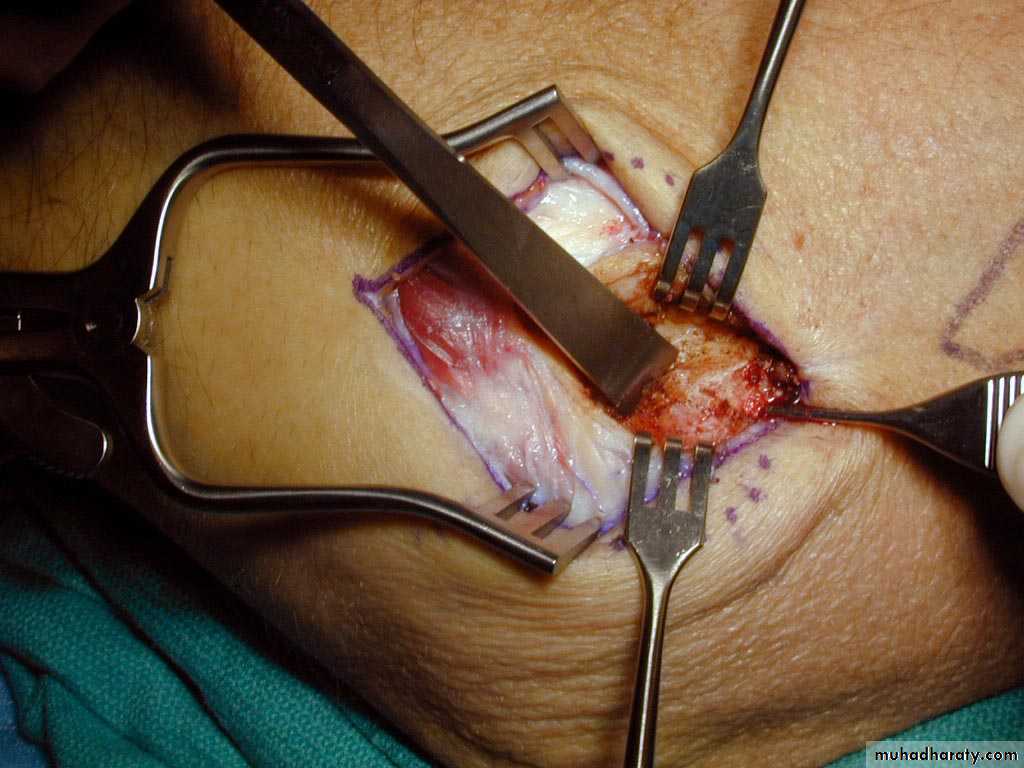
Operative
Tennis elbow release



Injection of blood products
Autologous bloodPlatelet Rich Plasma (PRP)
Bone Marrow Aspirate

Cortisone Injections

Botulinum Toxin A Injection
Extracorporeal shockwave therapyHeal with Steel?
Reserved for refractory casesDebridement of abnormal tendon of ERCB

Conclusion
What should we do?Corticosteroids should be used cautiously
PhysiotherapyAvoid exacerbating factors