By
Dr. Adel S. Al-Mayaly
Otolaryngology surgery
Scalp & Face Anatomy
Overview
The scalp is the soft tissue covering the skull.The scalp extends from the supraorbital margins anteriorly
to the highest nuchal lines at the back of the skull & down to the ears and zygomatic arches at the sides.
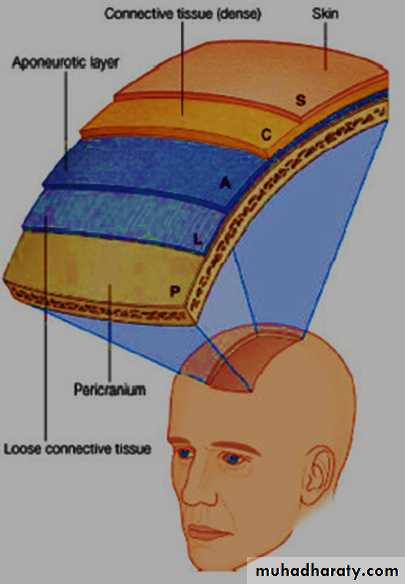
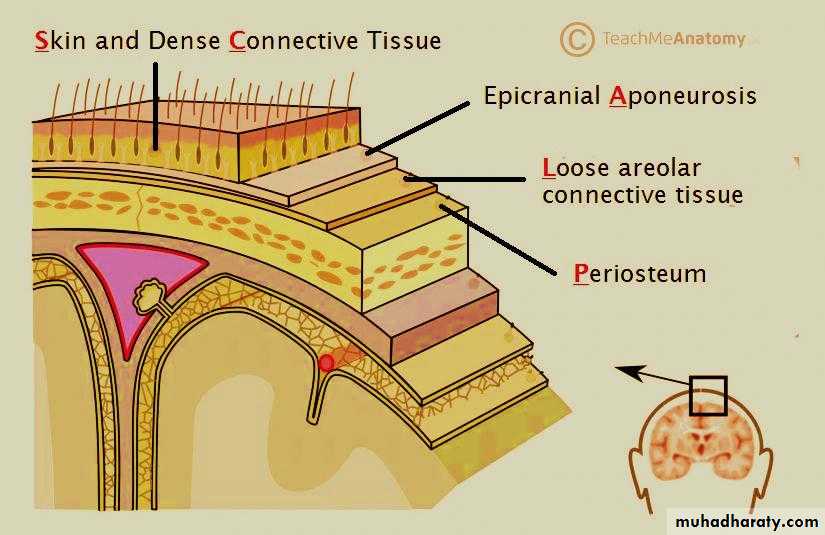
It consists of five layers.
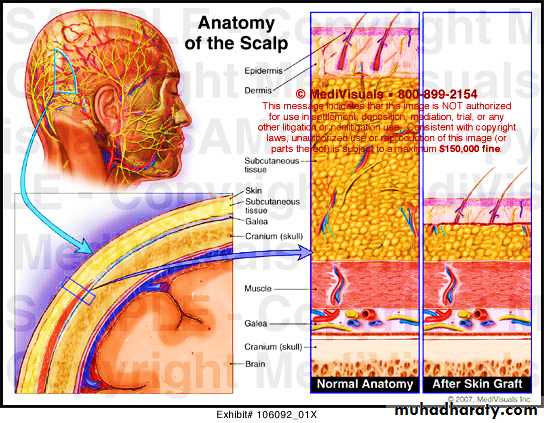
Layers of scalp
They are easily remembered using the acronym:S: skin
C: connective tissue
A: Epicranial aponeurosis (galea aponeurotica)
L: loose areolar tissue
P: periosteum (pericranium)

Skin of the Scalp
Is thickest skin in the body, & is thickest of all in the occipital area.It is being the hairiest part of the body. it also contains a
high concentration of sebaceous glands
the fibres of the scalp muscle are inserted into it.
Is connected to the galeal layer by tough fibrous septa.
Subcutaneous Connective Tissue
Contains many blood vessels and lymphatics.Contains tough dense septa that form inelastic layers around blood vessels.
These inelastic layers prevent complete contraction of vessels, causing profuse bleeding in scalp lacerations.
Infection of the superficial layer of the scalp remains localized because of the fibrous septa.
Galea AponeuroticaEpicranial Aponeurosis
Is the dense epicranial aponeurosis that merges with the fascia overlying the occipitalis
muscle posteriorly and the frontalis muscle, anteriorly.
SURGICAL IMPLICATIONS
The galea aponeurotica is the most stable layer in the suturing of the scalp.After craniectomy;
the galeal layer should be approximated to prevent dehiscence of the scalp incision due to swelling of the intracranial contents.
Transverse lacerations of the scalp, including
the galea, tend to gape as a result of the opposing actions of the frontalis and occipitalis m.
Loose Areolar Tissue
Is a danger space of the scalp.• Is located between the epicranial muscles and the pericranium (periosteum).
• Forms a potential subgaleal space bounded posteriorly by attachments of the occipitalis muscles to the superior nuchal line and laterally by the zygomatic arch bilaterally.
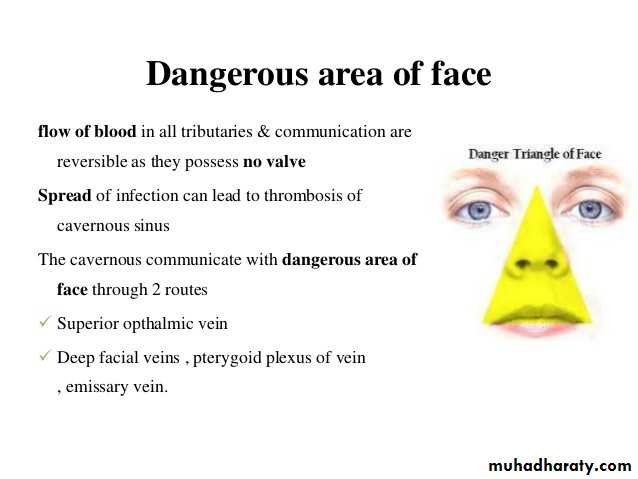
It is traversed by small arteries and emissary veins connecting the superficial scalp veins to the IC venous sinuses
SURGICAL IMPLICA TIONS
Danger space of the scalp: infection of this space may result in septic emboli from the emissary veins into the intracranialsinuses.
Because the frontalis muscle has no attachments between the
superciliary ridges anteriorly, hemorrhage and infection may extend to the upper & lower eyelids.
Pericranium (Periosteum)
The pericranium is the periosteum of the vault of the skull.
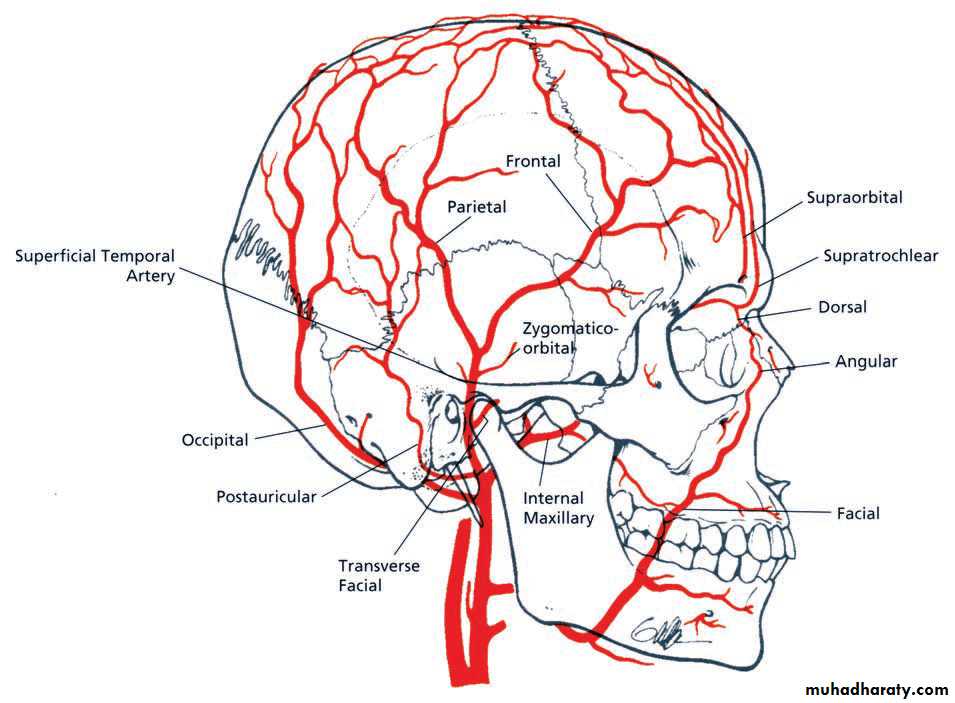
Blood supply
The arteries of the scalp are derived from the1- External carotid artery by the occipital, posterior auricular and superficial temporal branches.
2- Internal carotid A. via supraorbital & supratrochlear A
All these arteries anastomose very freely with
each other.
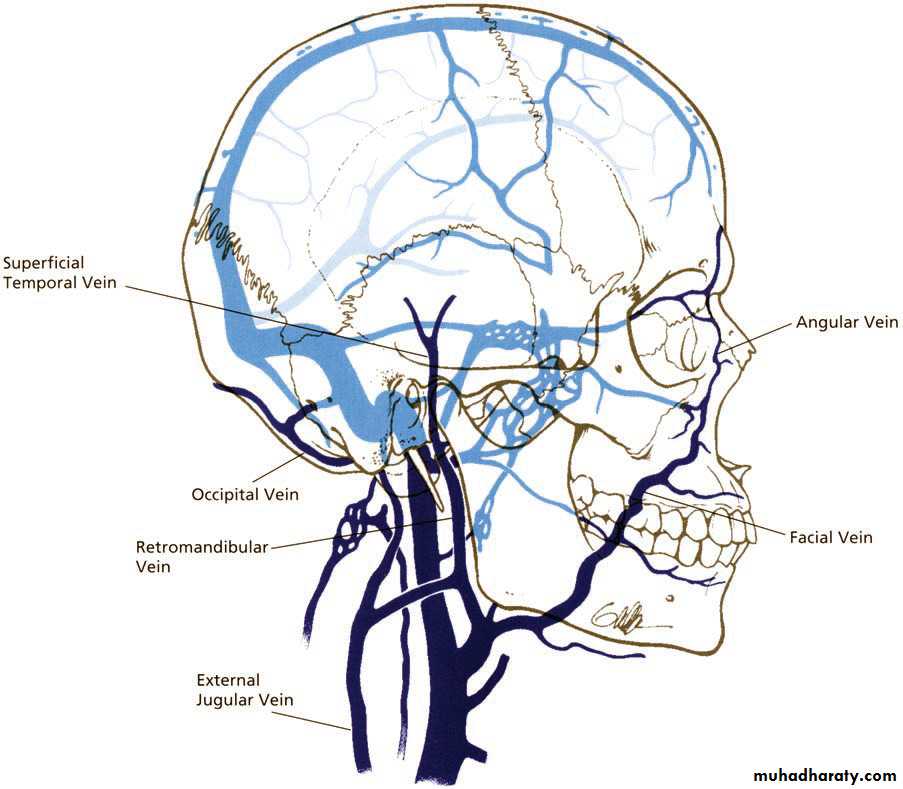
The veins of the scalp run back with the arteries.


Lymph drainage
There are no lymph nodes within the scalp.the posterior half of the scalp drain to occipital and mastoid nodes,
from the anterior half to preauricular (parotid) nodes
.
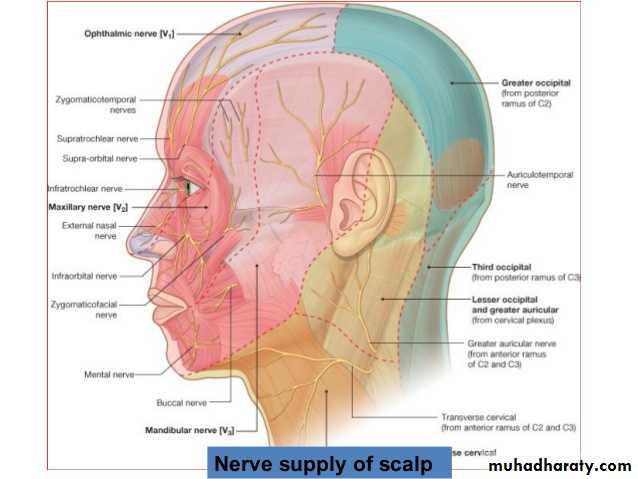
Nerve supply
The main sensory nerves run with the arteries.
Face
The face is the part of the front of the head between the ears and from the chin to the hairline
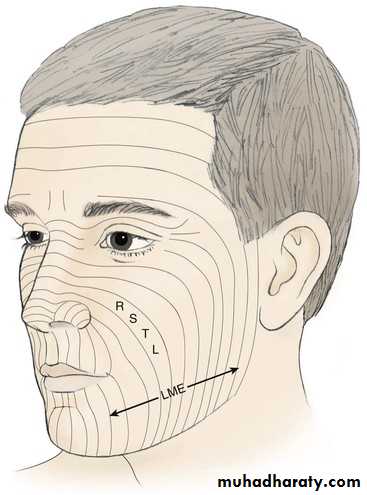
Skin of the face
The skin of the face has numerous sweat and sebaceous glands.It varies in thickness and is very thin on the eyelids.
There is no deep fascia on the face.
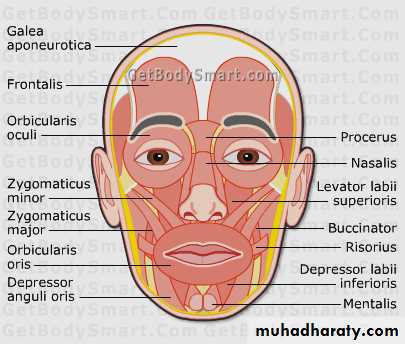
Muscles of the face
The muscles of ‘facial expression’ are developed from the mesoderm of the second pharyngeal arch.They all have 2 peculiarities:-
1- they are attached to the skin of the face.
2- they are all supplied by facial nerve.
FUNCTIONALLY
the muscles are differentiated to form groups around the orifices
The orifices of orbit, nose and mouth
there is a sphincter and an opposing dilator arrangement peculiar to each.
The varying expressions so produced on the face are side effects.
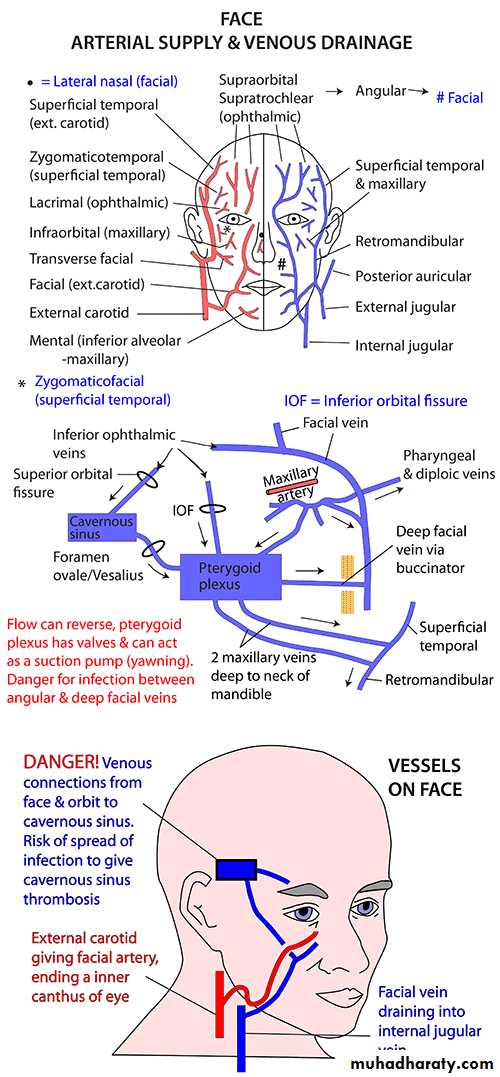
Blood supply of face
1- Arterial:- Facial arteryBranch of ECA
Course:-The facial artery hooks upwards over the inferior border of the mandible at the anterior border of the masseter
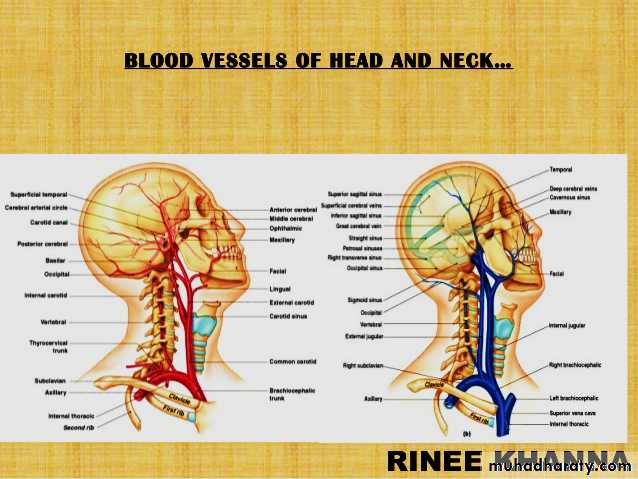
Venous Drainage