Clinical Training
50 SLIDES
for third year students
Prepared by
Dr. Ismael Dawoud
Chairman
Department of Medicine
2016 - 2017
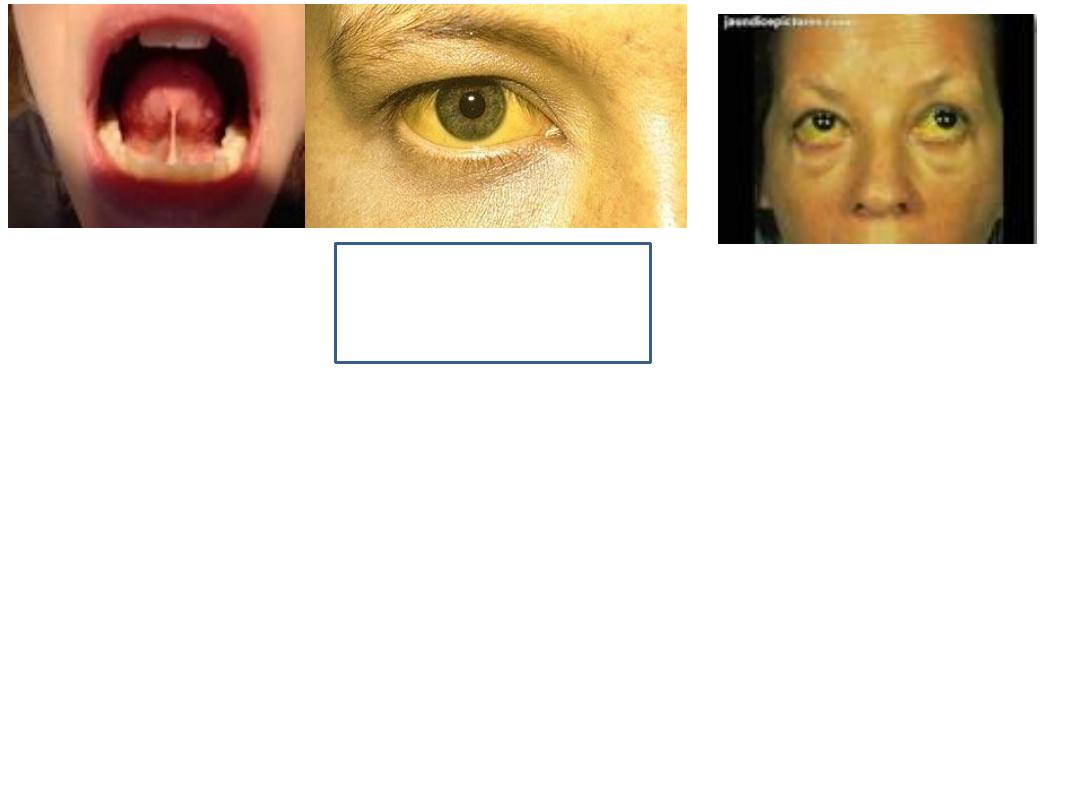
Look to sclera, skin and frenium of tongue.
Causes:
1.
Hemolytic: hereditary (spherocytosis, thalasemia, etc. Acquired: Drugs like
penecilln, methydopa, disease like SLE, Lymphoma).
2.
2. Hepatocellular (increase liver enzyme: ALT, AST) like viral hepatitis, alcohol,
drugs (INH, rifampicine, etc)
3.
Obstructive (increase ALP): stone in CBD, Ca head of pancreas, etc) pruritis
and deep jaundice.
4.
Congenital non-hemolytic: like Gilbert syndrome.
Jaundice

Some causes:
Nutritional (B12, folic acid (macrocytosis), iron (MC/HC), etc.
Blood loss; acute and chronic.
Hemolysis.
Bone marrow suppression.
Anaemia
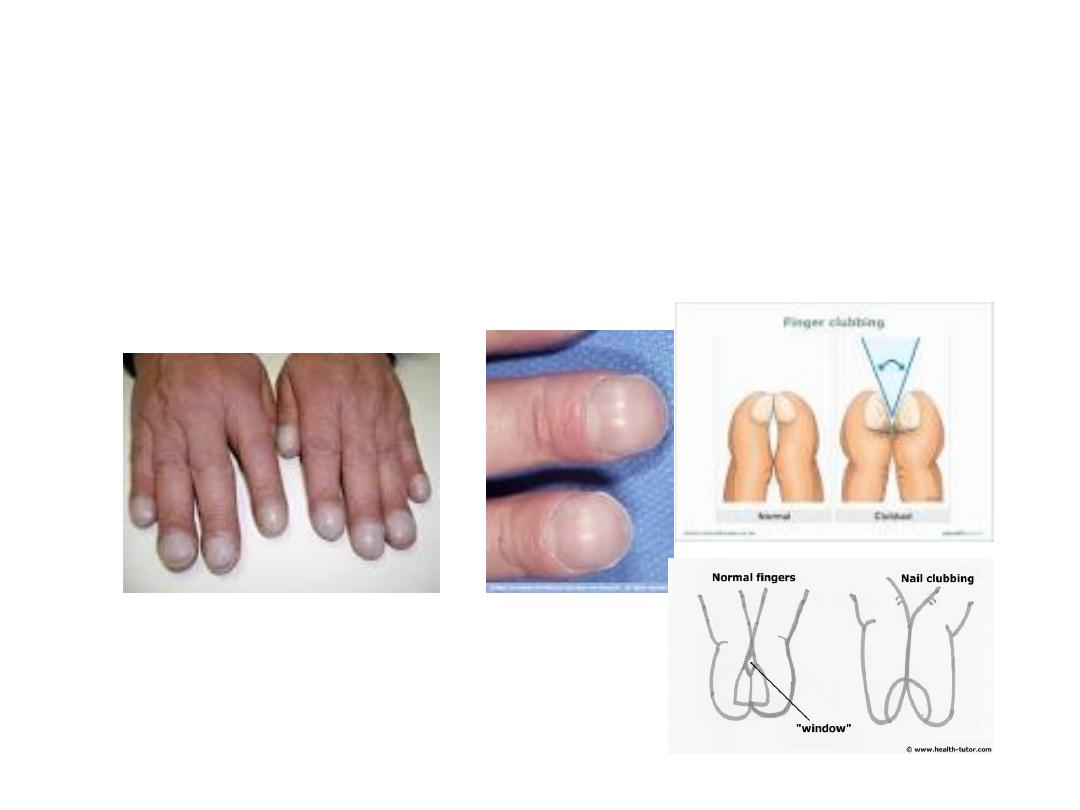
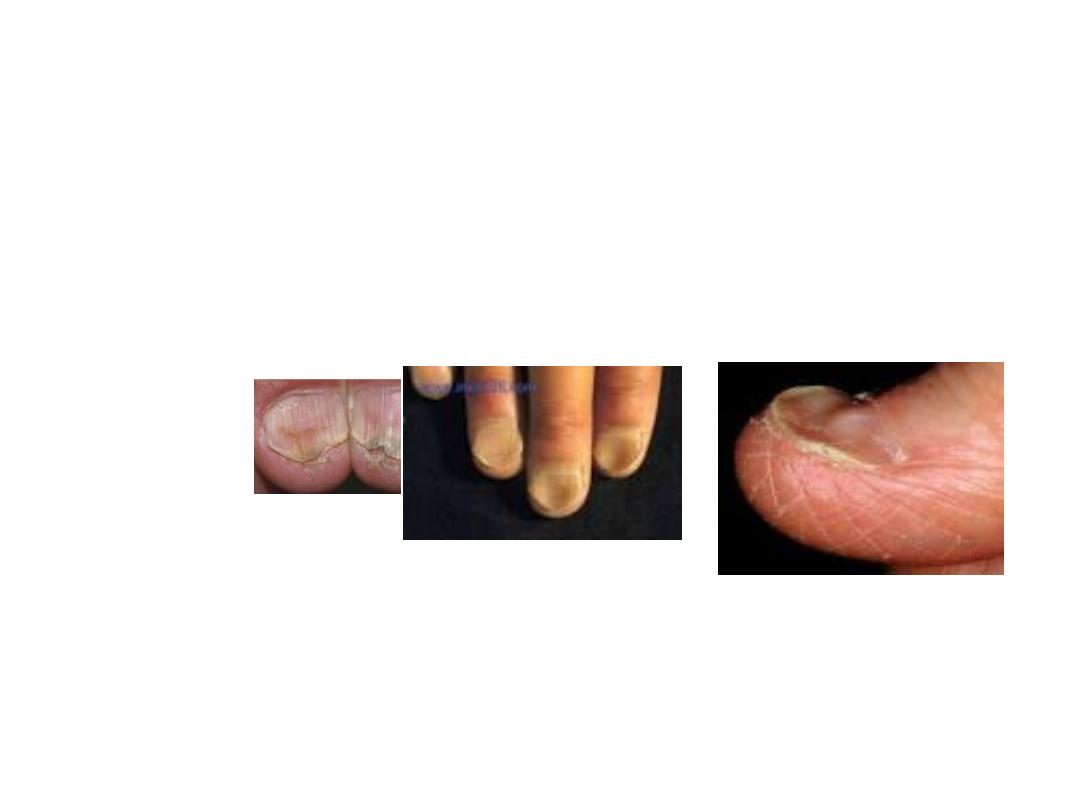
What theses pictures are demonstrating?
Clubbing of fingers and the first picture is also showing cyanosis.
Enumerate some causes:
1.
Respiratory: Bronchiectasis, lung cancer, etc.
2.
Heart: Cyanotic congenital heart disease.
3.
GIT; e. g ulcerative colitis, Crohn’s disease, liver cirrhosis.
Schamroth’s test - Attach two corresponding
fingers by their nails. There is free space at
healthy fingers between them called
Schamroth’s window. There is no free space at
clubbing fingers.

What this picture is showing?
Bruising. Due to trauma or bleeding tendency

What this picture is demonstrating?
Ascites.
Mention 3 physical sign for diagnosis of ascites.
1.
Abdominal distension with flat or everted umbilicus.
2.
In percussion: Shifting dullness is positive (the most important sign): percuss from
midline toward either flank. At point of dullness turn the patient toward the
opposite side so the dullness change to tympanic.
3.
Transmitted thrill of fluid wave become positive in tense ascites.

Diagnosis:
Abdominal striae
Causes:
Pregnancy, Obesity, Cushing’s
syndrome
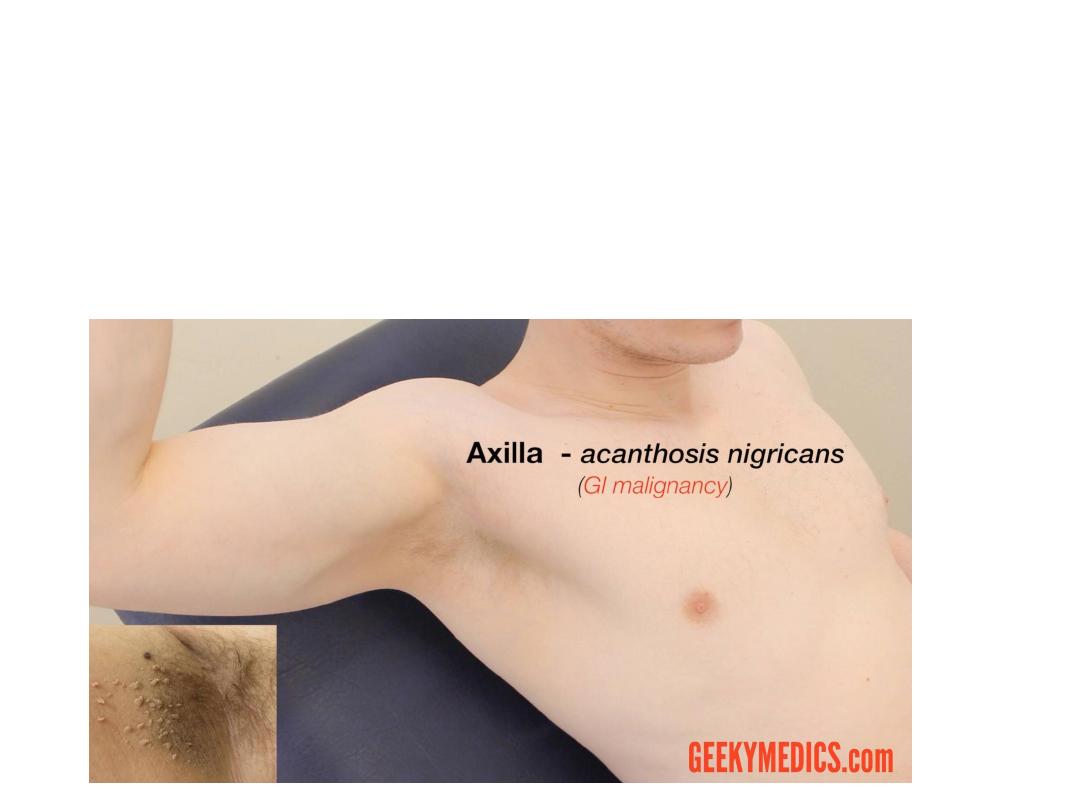
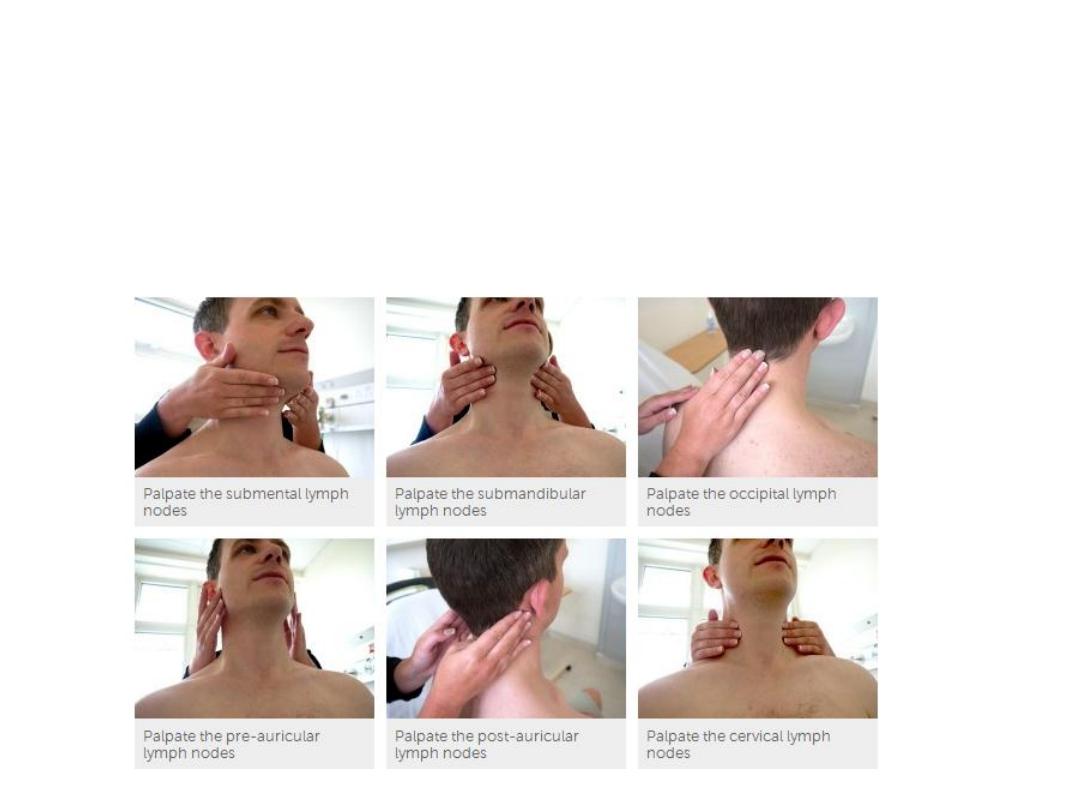
What is the value of axillary examination?
For detection of the following:
Lymphadenopathy – malignancy / infection
Hair loss – malnourishment / iron deficiency anaemia
Acanthosis nigricans (darkened pigmentation) – GI
adenocarcinomas / obesity
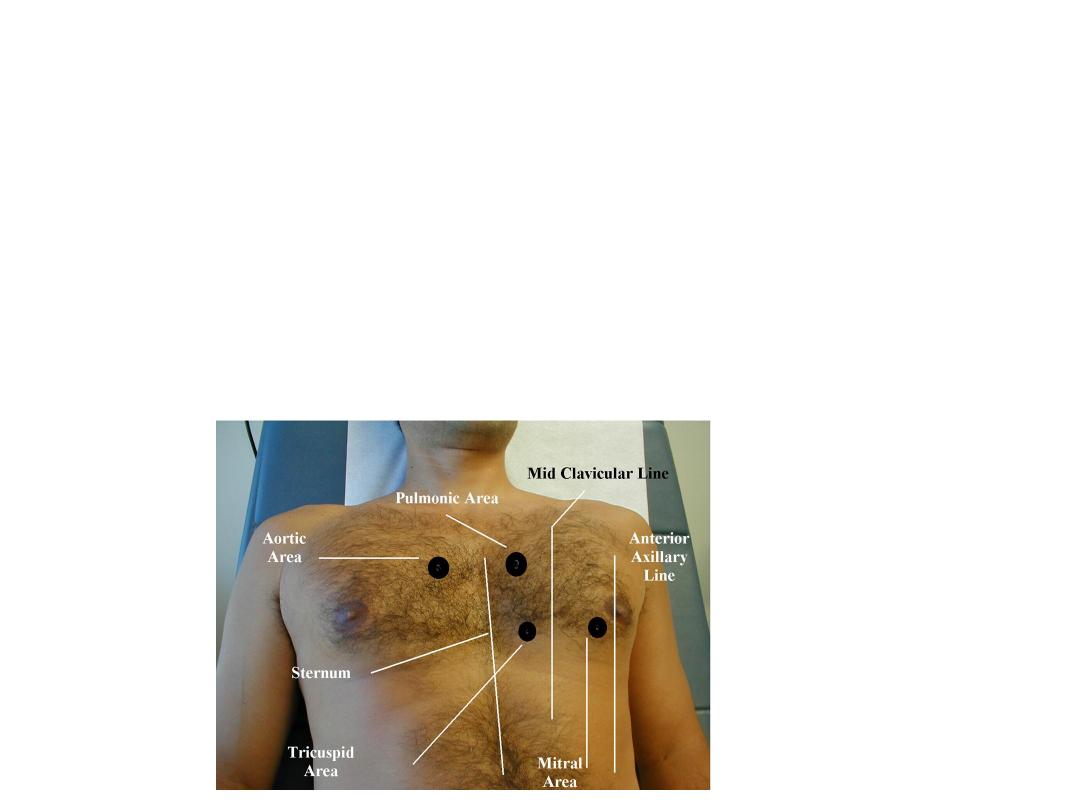
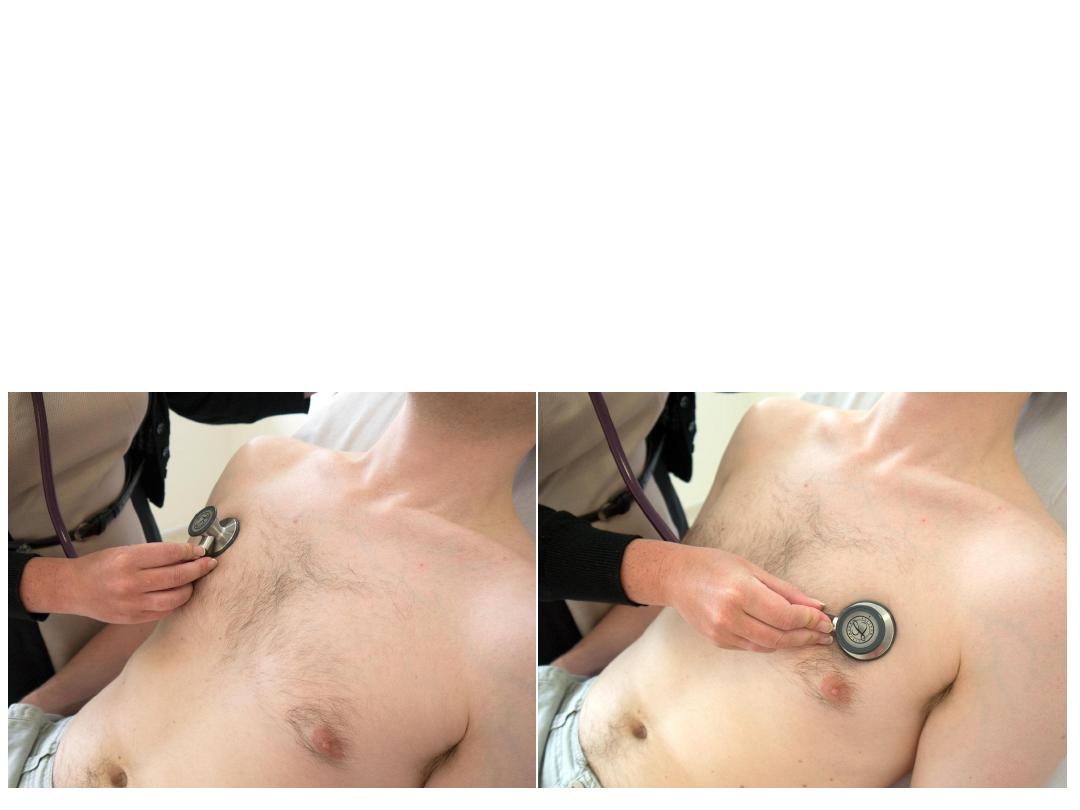
What is the definition of precordium?
Precordium: area on anterior chest that covers heart and great vessels.
What are the ausculatatory areas of the heart?
1.
Mitral area at apical area (5
th
intercostal /midclavicular).
2.
Tricuspid area: Just to the left of lower sternal area.
3.
Aortic area: base of the heart at 2
nd
intercostal space just to the
right of sternum.
4.
Pulmonary area: base of the heart at 2nd intercostal space just to
the left of sternum.
What is the picture diagnosis?
Koilonychia.
Cause: Iron deficiency anaemia.
What are the expected finding on inspection
during cardiac examination?

Comment on heart sounds:
The two major sounds heard in the normal heart sound like
“lub dub”. The “ lub” is the first heart sound, commonly
termed S1, and is caused by turbulence caused by the
closure of mitral and tricuspid valves at the start of systole.
The second sound,” dub” or S2, is caused by the closure of
aortic and pulmonic valves, marking the end of systole. Thus
the time period elapsing between the first heart sound and
second sound defines systole (ventricular ejection) and the
time between the second sound and the following first
sound defines diastole (ventricular filling).
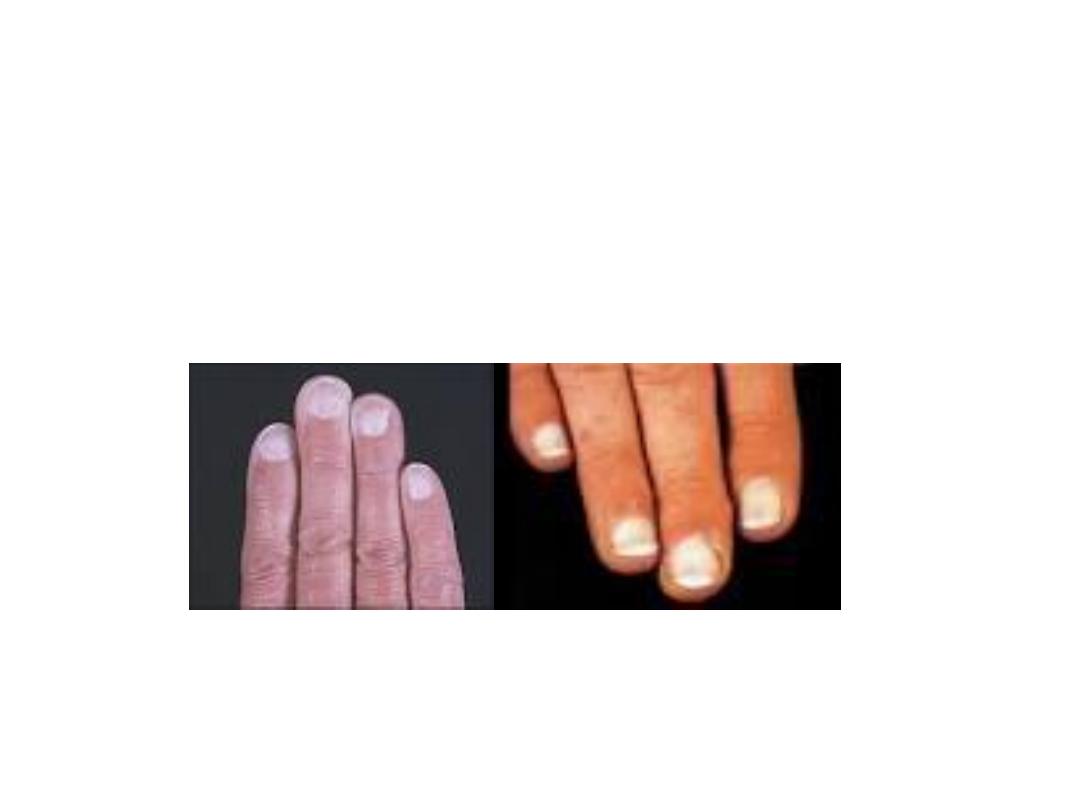
What is the diagnosis?
White nail
.
Cause:
hypoalbuminaemia
.

Q: Define auscultation, mention two main stethoscope parts and
enumerate its purpose:
Auscultation:
is the term for listening to the internal sounds of the
body.
Auscultation
is performed for the purposes of examining;
1. the circulatory system and respiratory system (heart sounds and
breath sounds).
2. gastrointestinal system (bowel sounds).
The stethoscope comprises a bell and a diaphragm. The bell is most
effective at transmitting lower frequency sounds, while the diaphragm
is most effective at transmitting higher frequency sounds
Techniques

To optimize the effectiveness of auscultation the surroundings
should be:
1.Quiet - the ambient noise might interfere the heart and lung
sounds.
2.Warm - so that the patient feels comfortable while the upper
part of the body is being exposed. Also, it is to avoid shivering
that may add the noise.
3.Appropriate lighting - to allow good coordination between
visual and auscultatory findings.
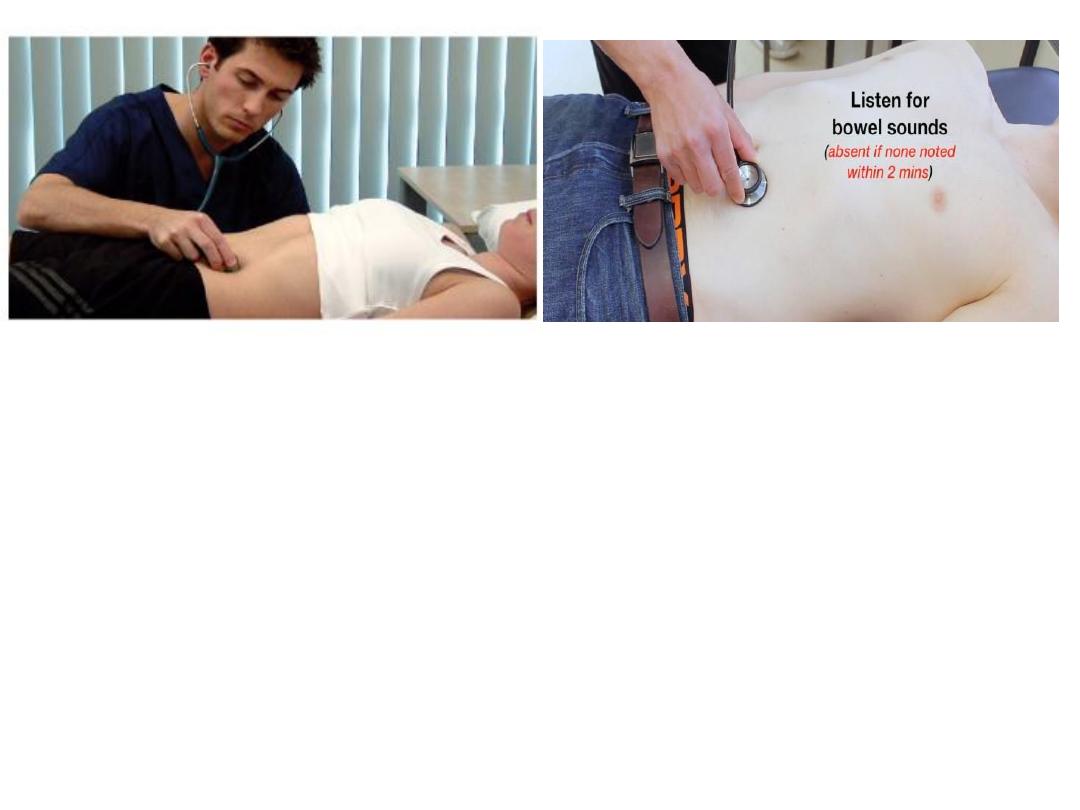
What this clinical examination is demonstrating ?
This is auscultation for bowel sounds.
What other things which can be detected by abdominal auscultation?
Friction rub over spleen and liver (inflammation)
Arterial bruit (Aortic bruits – auscultate just above the umbilicus – AAA
Renal bruits – auscultate just above the umbilicus, slightly lateral to the
midline).
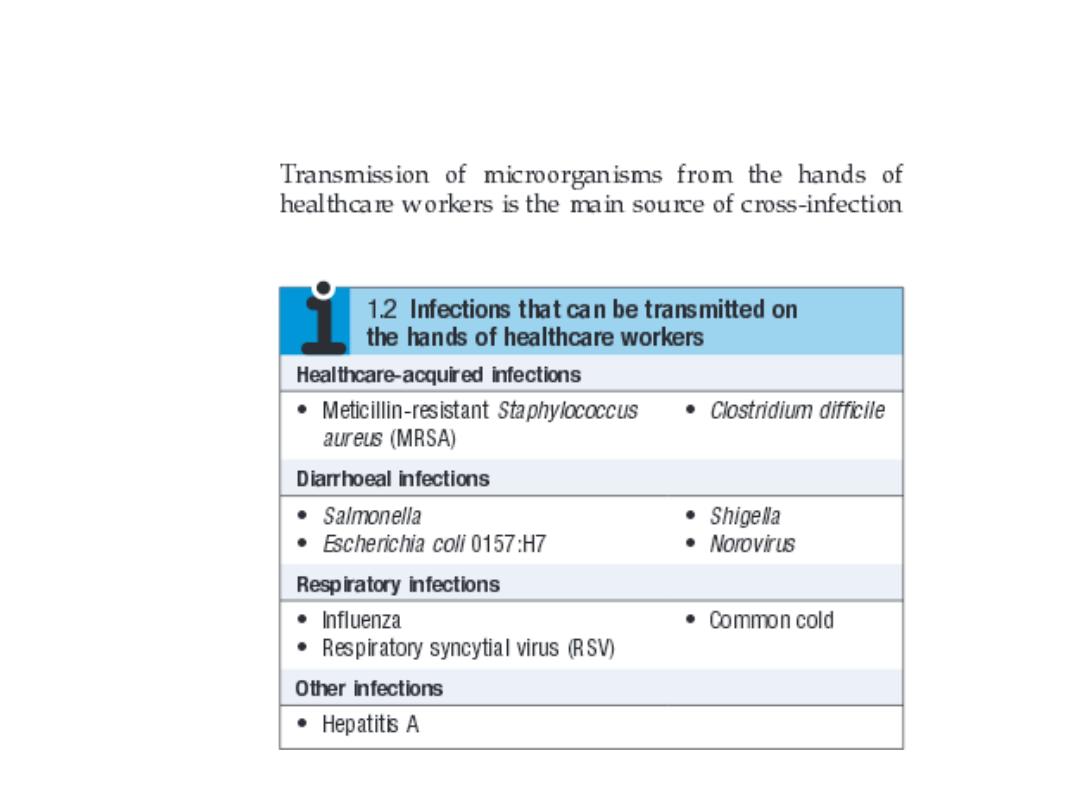
What is the importance of hand washing
and cleanliness before examining the
patient? Give two examples
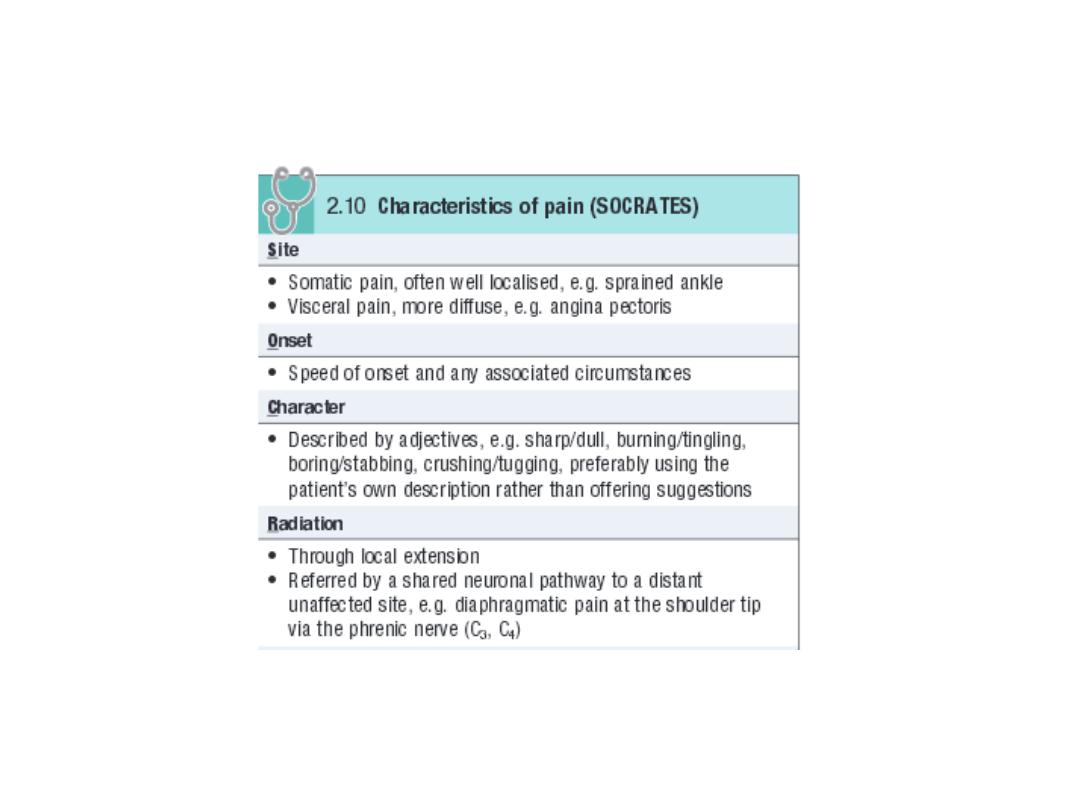
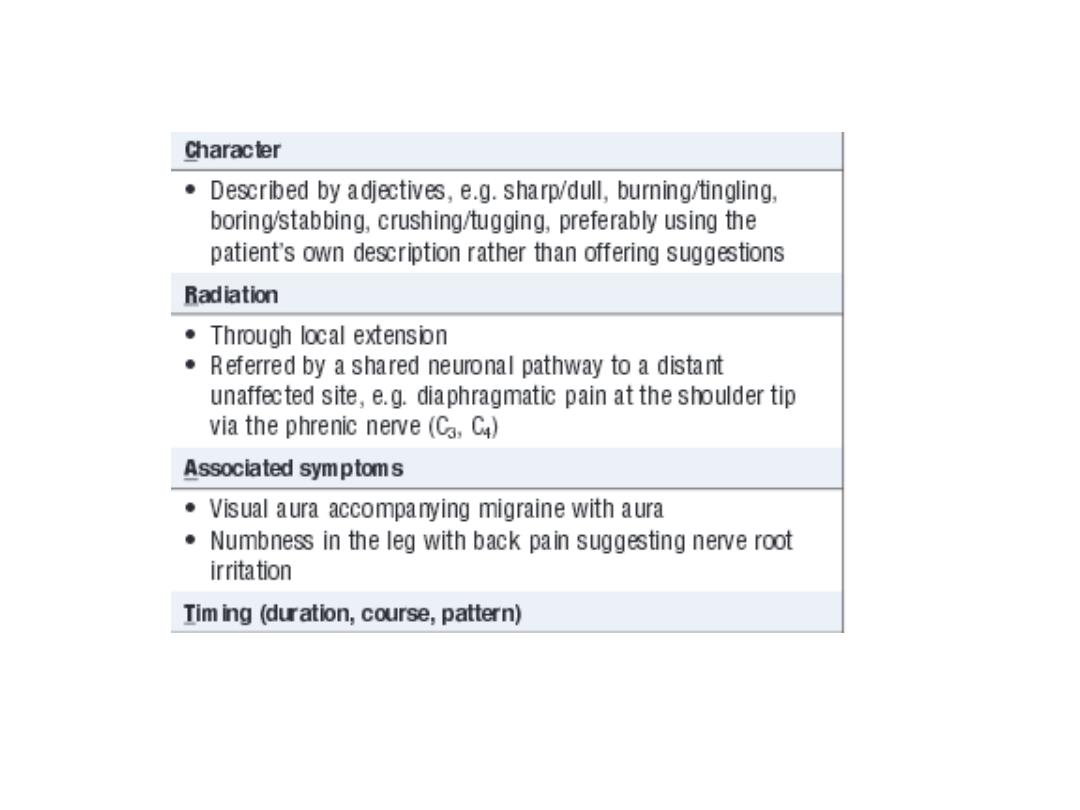
How you can analyze pain as a common symptom in
every day practice? Enumerate and comment on one.
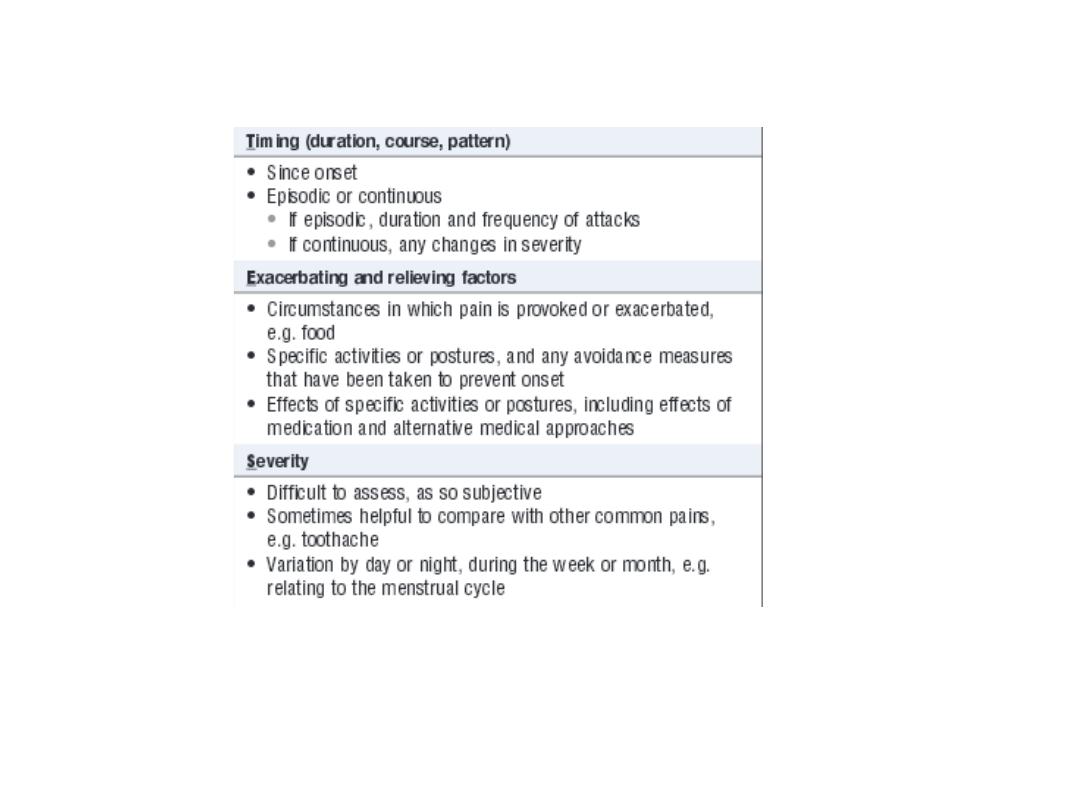

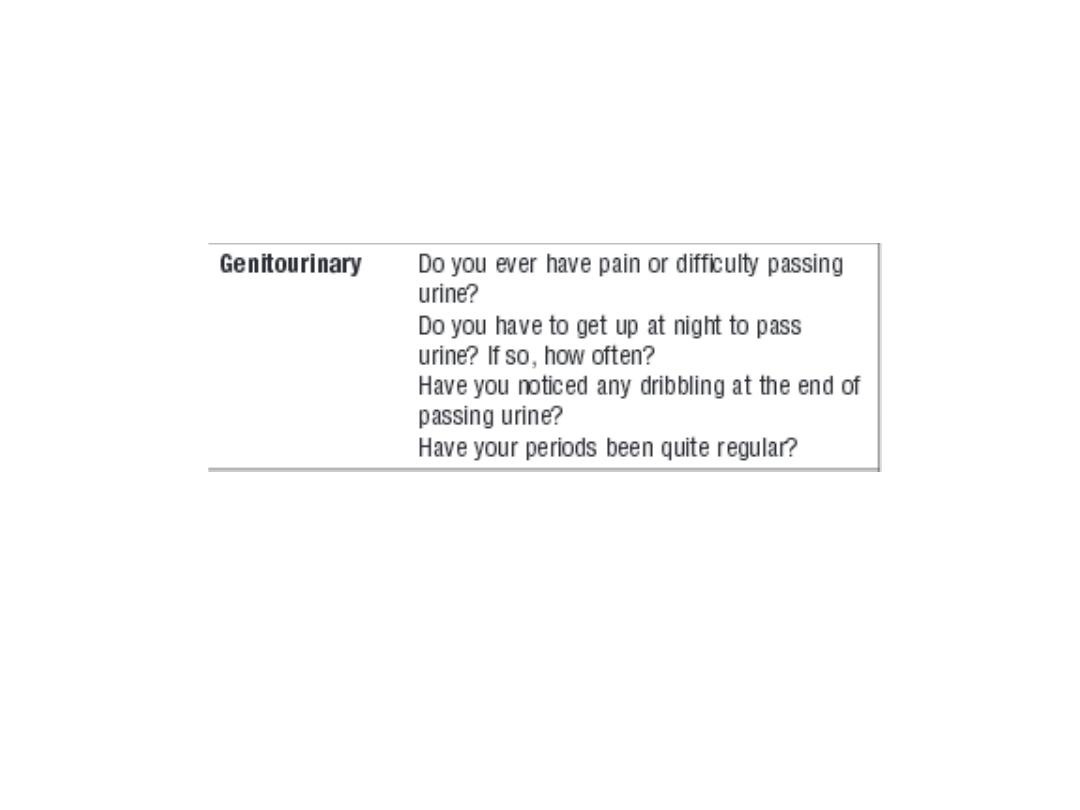
Mention the important questions about common
symptoms in cardiovascular, respiratory GIT and
genitourinary systems
The answer in next slides

Cardiovascular:
Ask about chest pain and its characters (ischemia,
pericarditis).
Ask about palpitation (SVT, atrial fibrillation, etc.)
Ask about waking up at night due to shortness of
breath (paroxysmal nocturnal dyspnea and pulmonary
oedema).
Respiratory:
Ask about cough and whether dry or productive of
sputum.
Ask about wheeze (bronchial asthma, bronchitis, etc.)
Ask about coughing of blood (TB, lung cancer, etc.).
Ask about shortness of breath.

GIT:
Ask about
dyspepsia
(indigestion): It is an upper abdominal discomfort. Many
causes : functional is the commonest cause , peptic ulcer, gastritis, cancer, etc.
Ask about
heart burn:
Burning sensation behind the sternum (retrosternal) due
to regurgitating (reflux) of stomach content to oesophagus in a disease called
gastroesophageal reflux disease (GERD ).
Ask about
abdominal pain
(Location: epigastric, lower abdomen, mid central,
etc.) , association and nature (constant or colicky).
Ask about a
recent change in bowel habit
(diarrhea, or constipation).
Ask about stool:
If it
containing
blood, mucus, food particles , etc.
Ask about
amount of stool (stool size):
small amount (in large bowel disease,
large sized stool usually in diseases of small bowel.
Bulky, offensive, greasy with difficulty in washing and floating stool in WC
indicates malabsorption syndrome.

What is hemoptysis? Enumerate some causes.
It is coughing of blood (mixed with sputum or pure blood)
Causes:
1. Pulmonary TB.
2. Bronchiectasis.
3. Carcinoma of lung.
4. Pulmonary infarction.
5. Mitral stenosis.
6. Blood disease.

What are the questions you like to ask a
patient who is presenting with SOB?
1. Onset (sudden or gradual.
2. Duration (hours, days, months, etc.)
3. Exertional (specify which kind of activity
provoke it ). or at rest.
4. Associated symptoms (cough, chest pain,
etc.).
What is orthodnea?
It is feeling dyspnic on laying down. It is
typically occur in left side heart failure
(pulmonary odema).

Enumerate the physical signs and symptoms of left side
heart failure:
The patient is feeling short of breath (dyspnea) and you
may see cyanosis, tachycardia and orthopnea in general
examination.
Apex of the heart may be displaced, Auscultation of chest
will reveal fine basal (at base of lungs posteriorly)
crepitation.
What are the features of right side heart failure:
Fatigue, cardiomegaly, raised JVP, bilateral pitting leg
oedema and may be features of ascites and pleural
effusion.
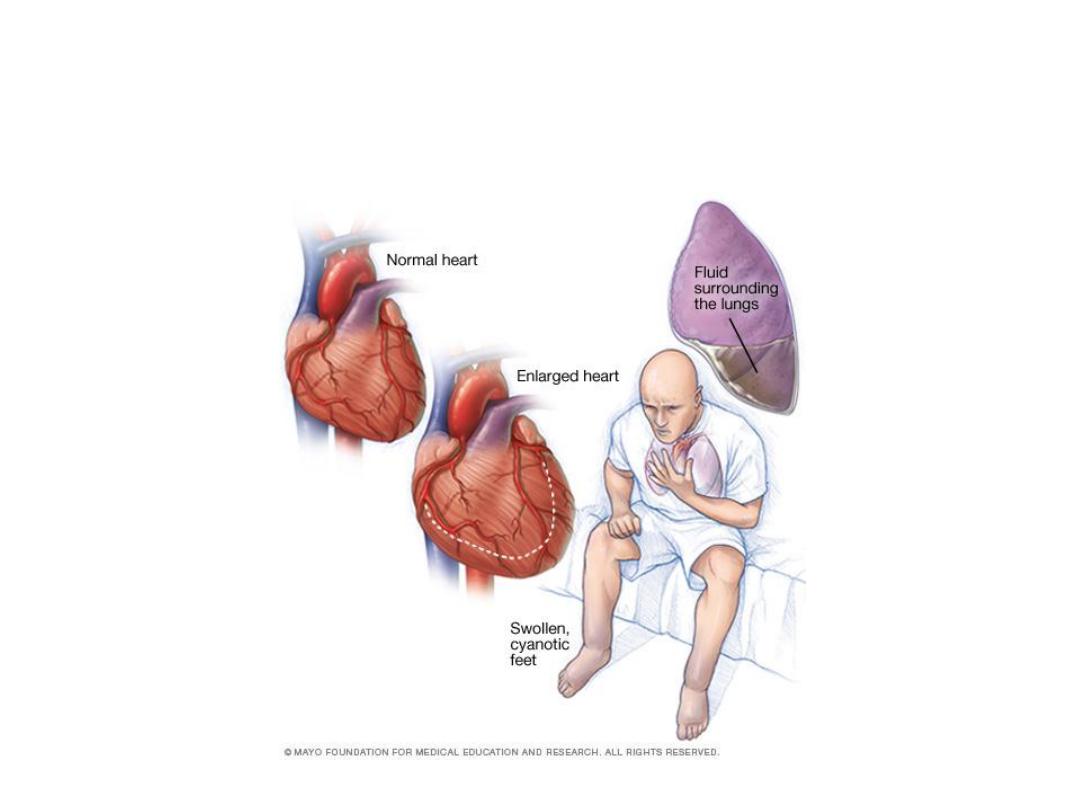
This picture demonstrating a patient
with heart failure

مهم جدا
Comment on site and character of cardiac apex:
Site:
(the most lateral and most inferior; normally in the 5th left
intercostal space in the mid clavicular line)
Displaced or not
Character :
The following are the common characters of apex:
thrusting displaced apex beat
is caused by
volume overload
: an active
large stroke volume ventricle eg
aortic or mitral regurgitation
or left to
right shunts.
sustained apex beat
is caused by
pressure overload
eg
aortic stenosis
,
gross hypertension
.
tapping apex beat
-
mitral stenosis
.
diffuse pulsation asynchronous with apex beat
- left ventricular
aneurysm.
double or triple impulse
may occur in
hypertrophic obstructive
myopathy.
an impalpable apex beat
- obesity, overinflated chest, pericardial
effusion. Also consider dextrocardia

مهم جدا
Comment on types of murmurs in
:
Aortic stenosis (AS):
The murmur of aortic stenosis is typically a
mid-systolic ejection murmur
, heard best
over the “aortic area” or right second intercostal space, with radiation into the right
neck.
Aortic incompetence (regurgitation):
Early
Diastolic murmur.
Mitral regurgitation (MR):
Pan systolic murmur: usually best heard at the apex, with radiation into the axilla.
Mitral stenosis (MS):
Mid diastolic murmur.
Ventricular septal defect (VSD)
: It is usually best heard over the “tricuspid area”, or
the lower left sternal border.

What are the causes of MR?
A: Mitral valve regurgitation is usually either a
congenital
condition or a consequence of
rheumatic heart disease
,
marked left ventricular dilatation, acute infective
endocarditis, or papillary muscle dysfunction secondary to
acute or prior myocardial infarction.
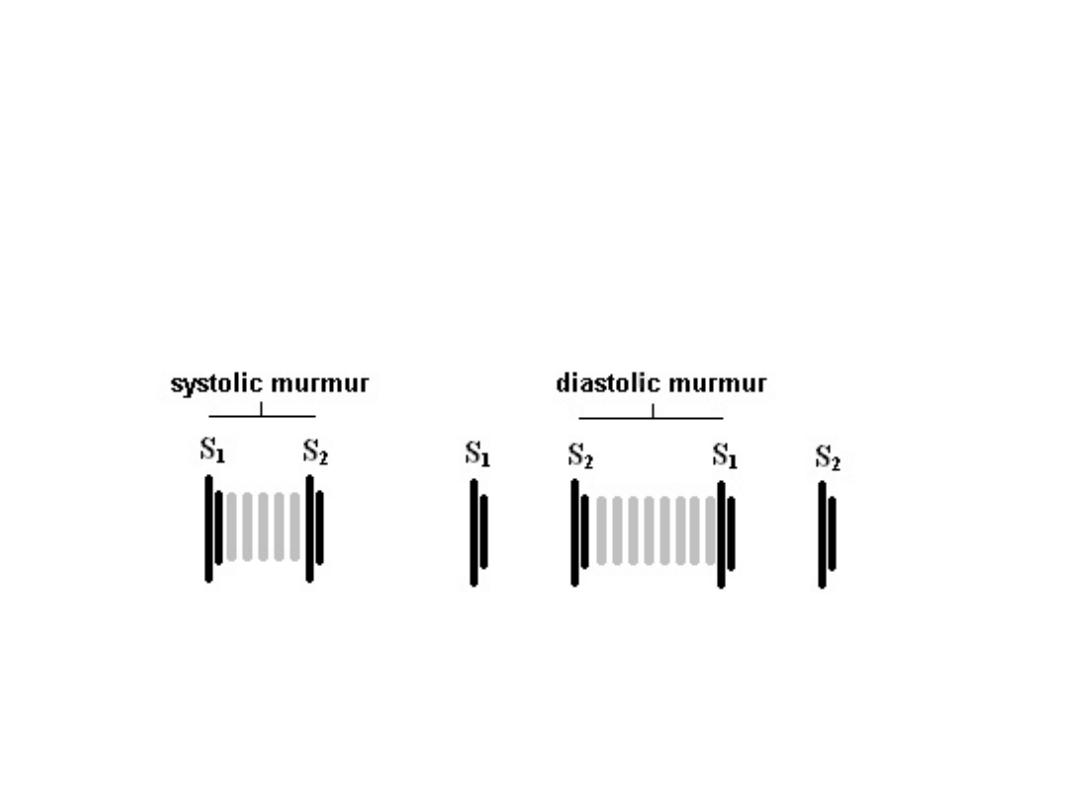
Diagrammatically demonstrate the heart sounds and cardiac murmurs
and give one example for each systolic and diastolic murmurs.
A. See the diagram below. مهم
B.
Example of systolic murmurs: MR and AS.
C.
Examples of diastolic murmurs: MS and AI.

What are steps of chest examination:
1.
INSPECTION.
2.
PALPATION.
3.
PERCUSSION.
4.
AUSCULTATION.

What this picture is demonstrating?
A. Chest expansion in step of
palpation
.

What this picture is showing? Enumerate 3 causes.
A. Flapping tremor.
1.
Type 2 respiratory failure.
2.
Hepatic (liver) failure.
3.
Renal (kidney) failure.

What are the things to be mentioned in pulse
examination?
Answer: Rate, rhythm, volume, character and
condition of vessel wall.

Give 2 examples of abnormal pulse rate:
مهم
1.
Tachycardia: pulse rate (more than) > 100 beat /m, bradycardia:
pulse rate (less than)< 60beat/m
Give 2 examples of completely irregular (irregular irregularity)Pulse.
1.
Atrial fibrillation (AF).
2.
Multiple ectopic.
Give 3 causes of AF:
thyrotoxicosis, ischemic heart disease (IHD),
hypertension, etc.
Give 2 examples of small volume pulse: Heart failure (HF), Volume loss
(diarrhea, vomiting, anaphylaxis, burn, hemorrhage, etc.).
Give 2 causes of large volume
(bounding) pulse: Hyperdynemic
circulation: chronic anemia, thyrotoxicosis, pregnancy, fever, etc.
Give one example for pulse character
: Collapsing pulse due to e. g.
thyrotoxicosis.
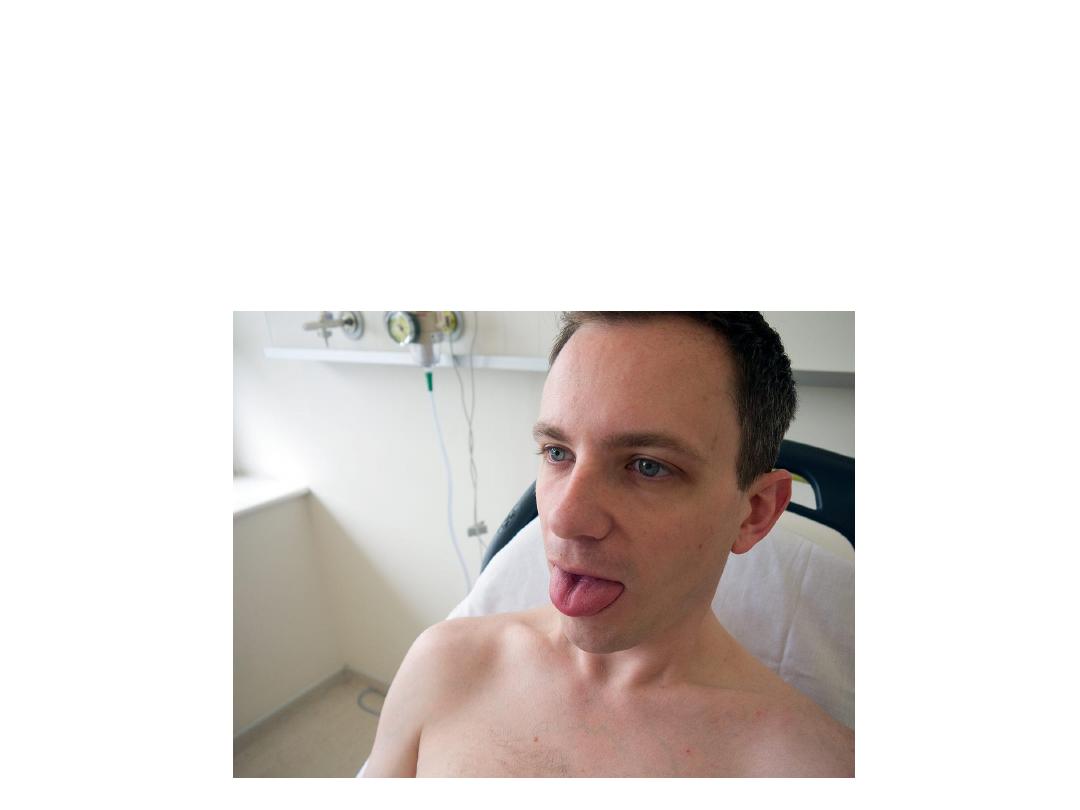
What is the value of this examination?
Tongue examination
for sign of dehydrations,
anemia, cyanosis, etc.

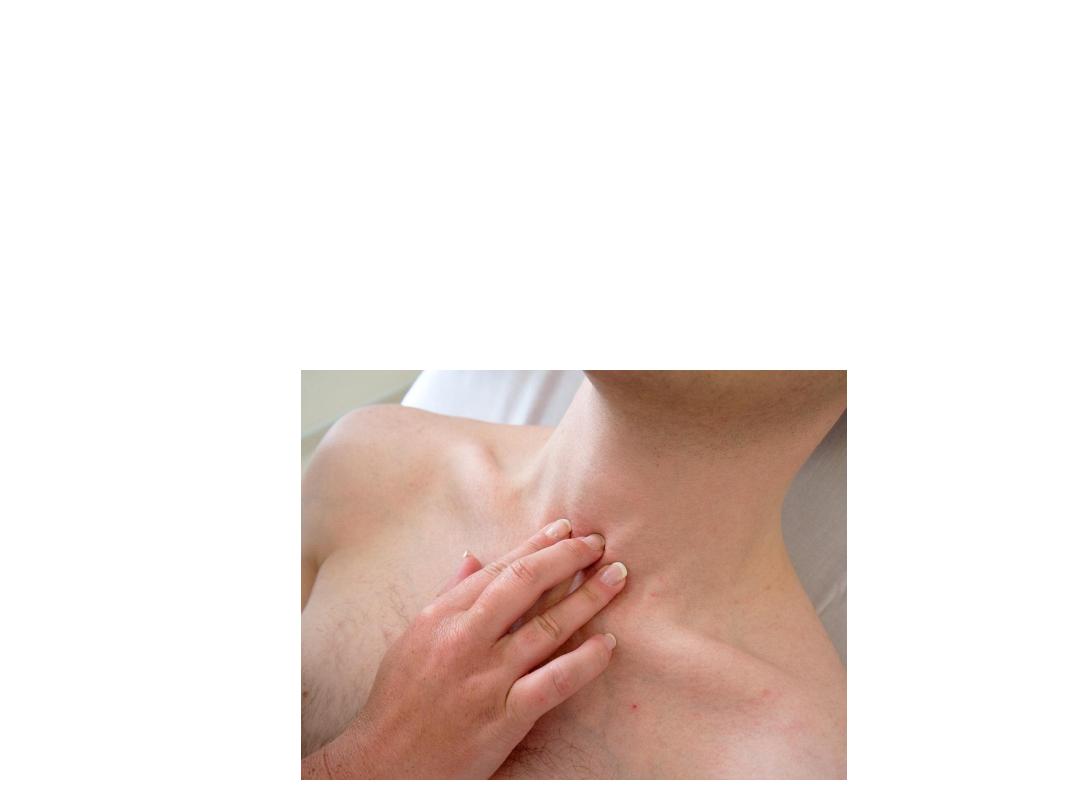
What is this examination?
Answer: Examination of left supraclavicular node (Virchow’s
Node ). This drains the thoracic duct so an enlarged node
(Troisier’s Sign) may suggest metastatic cancer e.g. lung or
abdominal.
What this picture is demonstration?
Tracheal palpation:
feel between the heads of the
two clavicles for the trachea. If it is deviated, it
may suggest a tumour or pneumothorax

What is this?
This is anterior chest percussion (step 3 in chest examination):
10.Perform percussion on both sides, comparing similar areas on both
sides. You should start by tapping on the clavicle which gives an
indication of the resonance in the apex. Then percuss normally for the
entire lung fields. Hyper-resonance may suggest emphysema where as
dullness suggests consolidation such as in pneumonia, effusion or a
tumour. Be sure to perform this on the back as well.

What is this?
This is test for tactile vocal fremitus. Place the
medial edge of your hand on the chest and ask
the patient to say “99” in English or 44 in
Arabic Do this with your hand in the upper,
middle and lower areas of both lungs. This
again gives a suggestion of the constitution of
the tissue deep to your hand.
What is this?
Auscultation of lungs (step 4 ):
Do this in all areas of both
lungs and on front and back comparing the sides to each
other.
Listen for any reduced breathe sounds,
or
added sounds:
crackles
(crepitation), wheeze (rhonchi),
pleural rub.

Give 2 causes for crepitation (crackles):
Bronchiectasis, pneumonia.
Give 2 causes of wheeze (rhonchi):
Bronchial asthma, bronchitis.
Give 1 cause of pleural rub:
pleurisy (inflammation of two surfaces of
parietal and visceral pleura).
Give1cause of stony dullness on chest percussion: pleural
effusion(accumulation of free fluid inside pleural space).
What these pictures are demonstrating?

Dilated veins on abdominal wall due
to inferior vena caval obstruction.
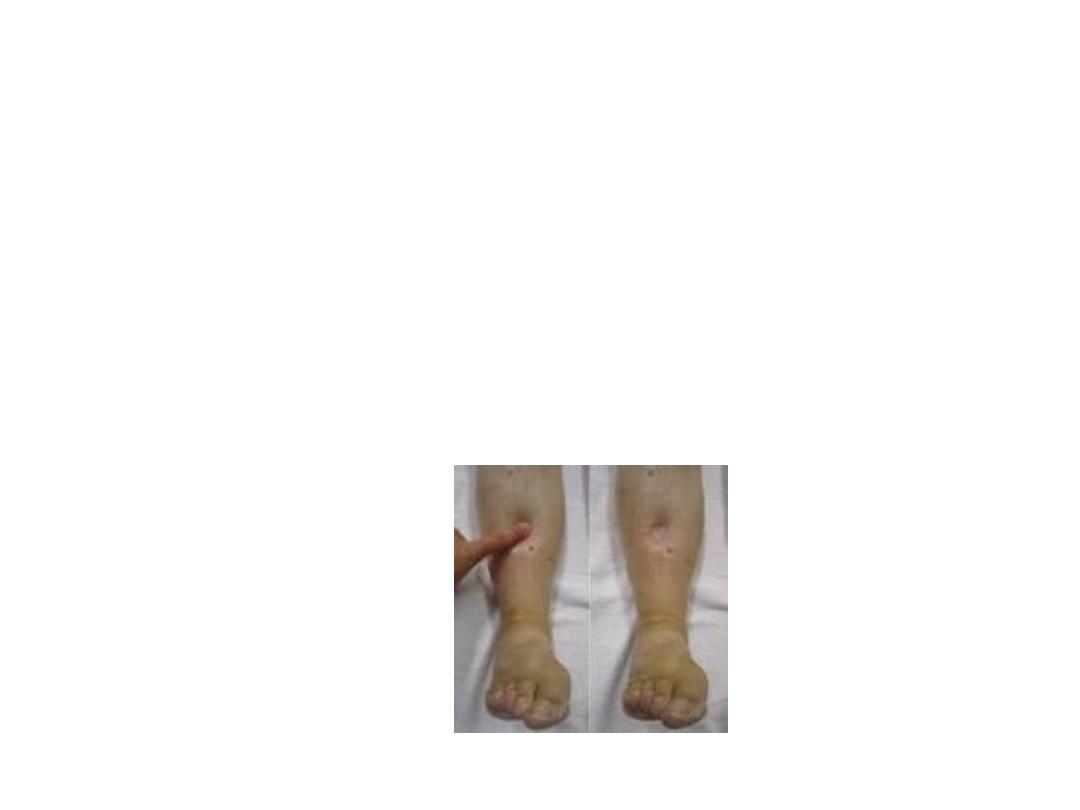
Bilateral pitting leg oedema
Causes:
Heart failure
Nephrotic syndrome (renal)
Chronic liver disease and cirrhosis and
other causes of hypoalbuminaemia.
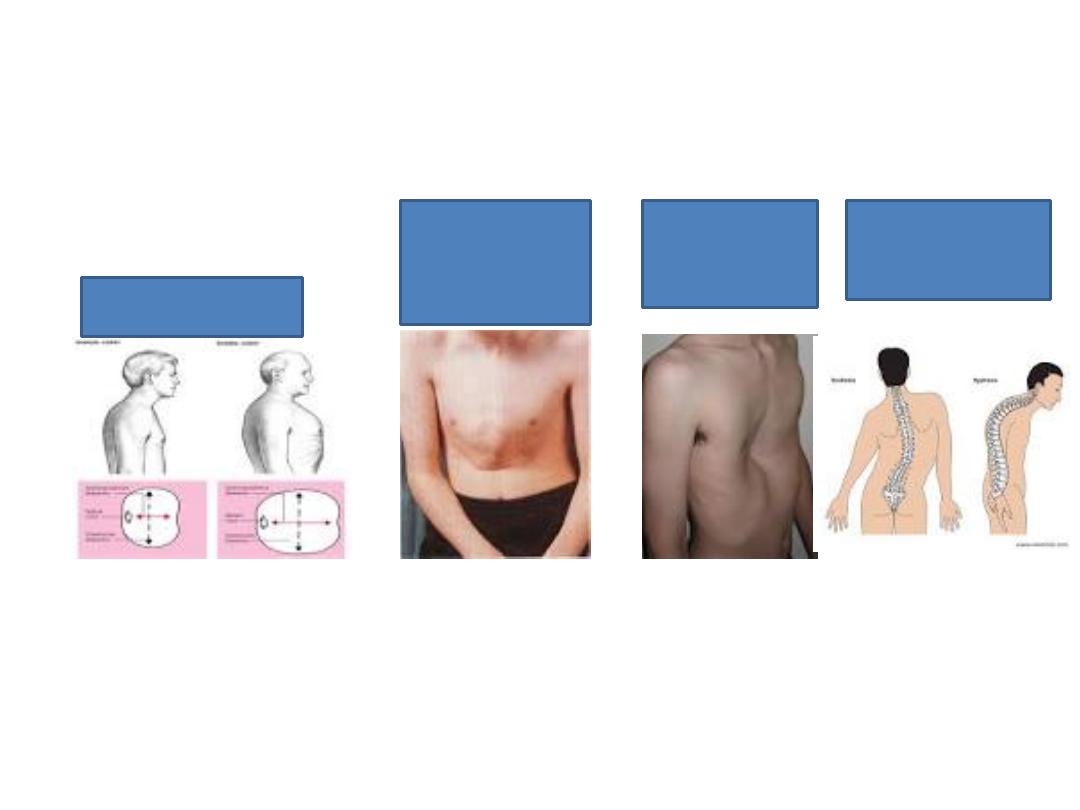
Some forms of chest
Barrel chest
emphysema
Pigeon chest
Asthma since
early
childhood
Pectus
excavatum
congenital
Scoliosis and
kyphosis

Unilateral leg swelling:
Causes: DVT, cellulitis, lymphatic
obstruction, ruptured baker cyst,
trauma.

How you can differentiate between enlarged spleen and enlarged
left kidney?
1.
You can not get above spleen.
2.
Spleen has a notch at medial side.
3.
Percussion is dull over the spleen
4.
Spleen is enlarged obliquely toward RIF.
5.
Kidney is bimanually palpable while spleen can be palpable by
one hand.