RESPIRATORY TRACT
UPPER AIRWAYS
NOSE
INFLAMMATIONS
Infectious Rhinitis.
“common cold,” is in most instances caused by one or more viruses.
Secondary bacterial infection enhances the inflammatory reaction and
produces an essentially mucopurulent or sometimes frankly suppurative
exudate.
Allergic Rhinitis.
Allergic rhinitis (hay fever) is initiated by hypersensitivity reactions to
one of a large group of allergens, most commonly the plant pollens.
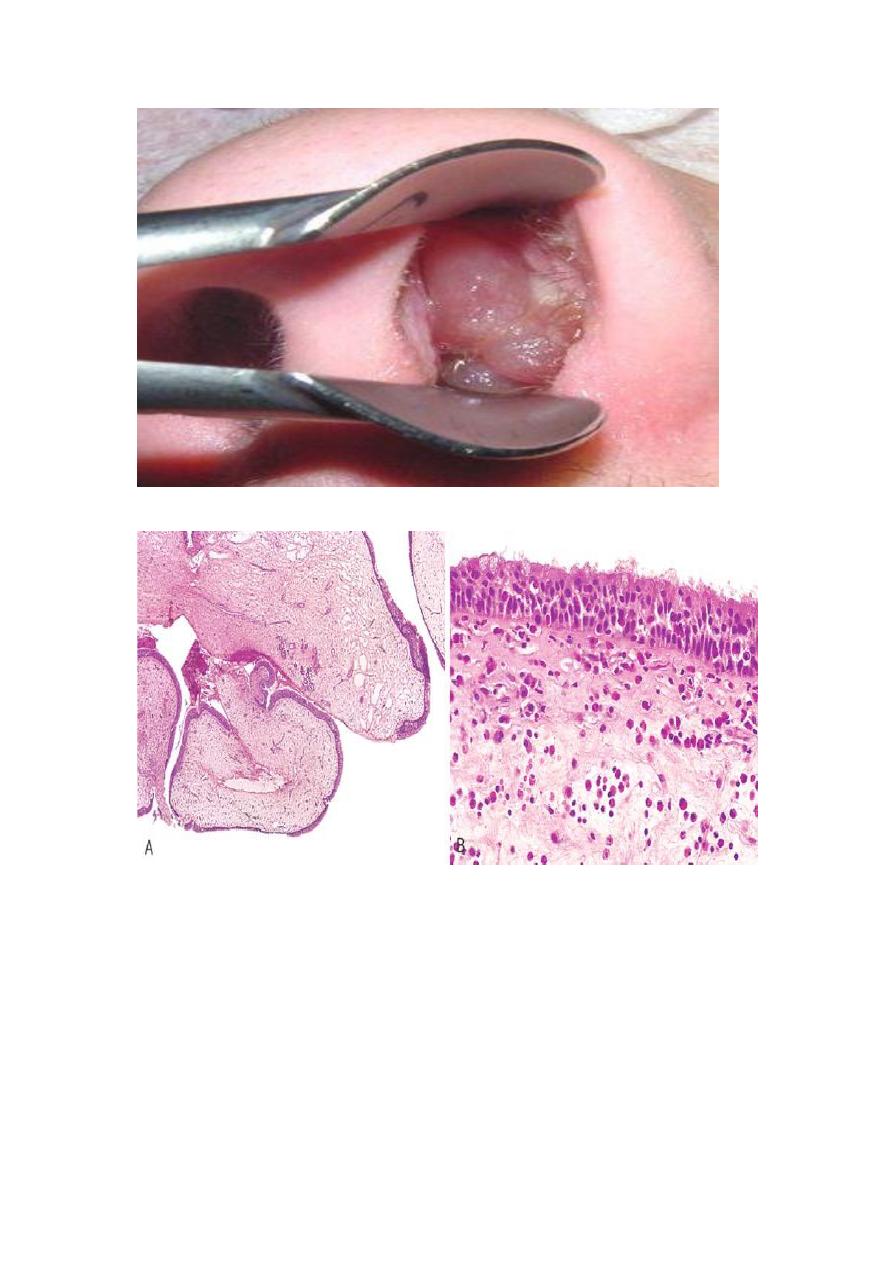
Nasal polyps:
Recurrent attacks of rhinitis may eventually lead to focal protrusions of
the mucosa, producing so-called nasal polyps, which may reach 3 to 4 cm
in length. On histologic examination these polyps consist of edematous
mucosa having a loose stroma, often harboring hyperplastic or cystic
mucous glands, infiltrated with a variety of inflammatory cells, including
neutrophils, eosinophils, and plasma cells with occasional clusters of
lymphocytes .
Sinusitis.
Acute sinusitis is most commonly preceded by acute or chronic rhinitis,
but maxillary sinusitis occasionally arises by extension of a periapical
infection through the bony floor of the sinus. Impairment of drainage of
the sinus by inflammatory edema of the mucosa producing empyema of

the sinus. Accumulation of secretions in the absence of direct bacterial
invasion, producing a so-called mucocele. Acute sinusitis may, in time,
give rise to chronic sinusitis
Nasopharynx
INFLAMMATIONS
Pharyngitis and tonsillitis
are frequent in the usual viral upper respiratory
infections. Most commonly implicated are rhinoviruses, echoviruses, and
adenoviruses. Bacterial infections may be superimposed on these viral
involvements, or may be primary invaders. The most common offenders
are the β-hemolytic streptococci, the major importance of streptococcal
“sore throats” lies in the possible development of late sequelae, such as,
rheumatic fever and glomerulonephritis .

Tumors of the Nose, Sinuses, and Nasopharynx
NASOPHARYNGEAL ANGIOFIBROMA: this is highly vascular tumor ,
occur almost exclusively in adolescent males. It is benign, cause profuse
bleeding during surgery.
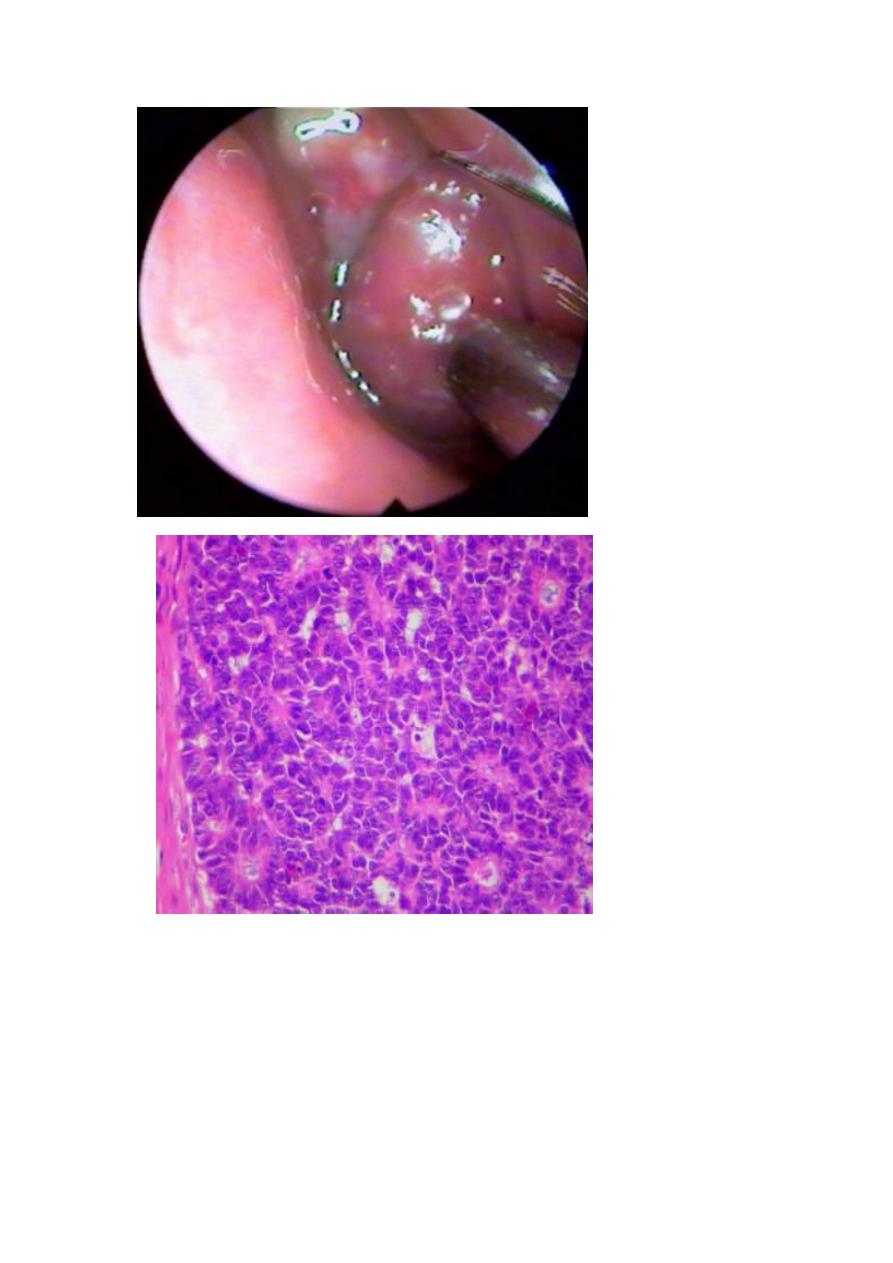
OLFACTORY NEUROBLASTOMA:
Uncommon highly malignant tumor, originate from olfactory membrane
of sinonasal tract composed of round small cells. The cells are of
neuroendocrine origin, age incidence from 2-90 years, it metastasize
widely. Treated by combination radiation and chemotherapy.
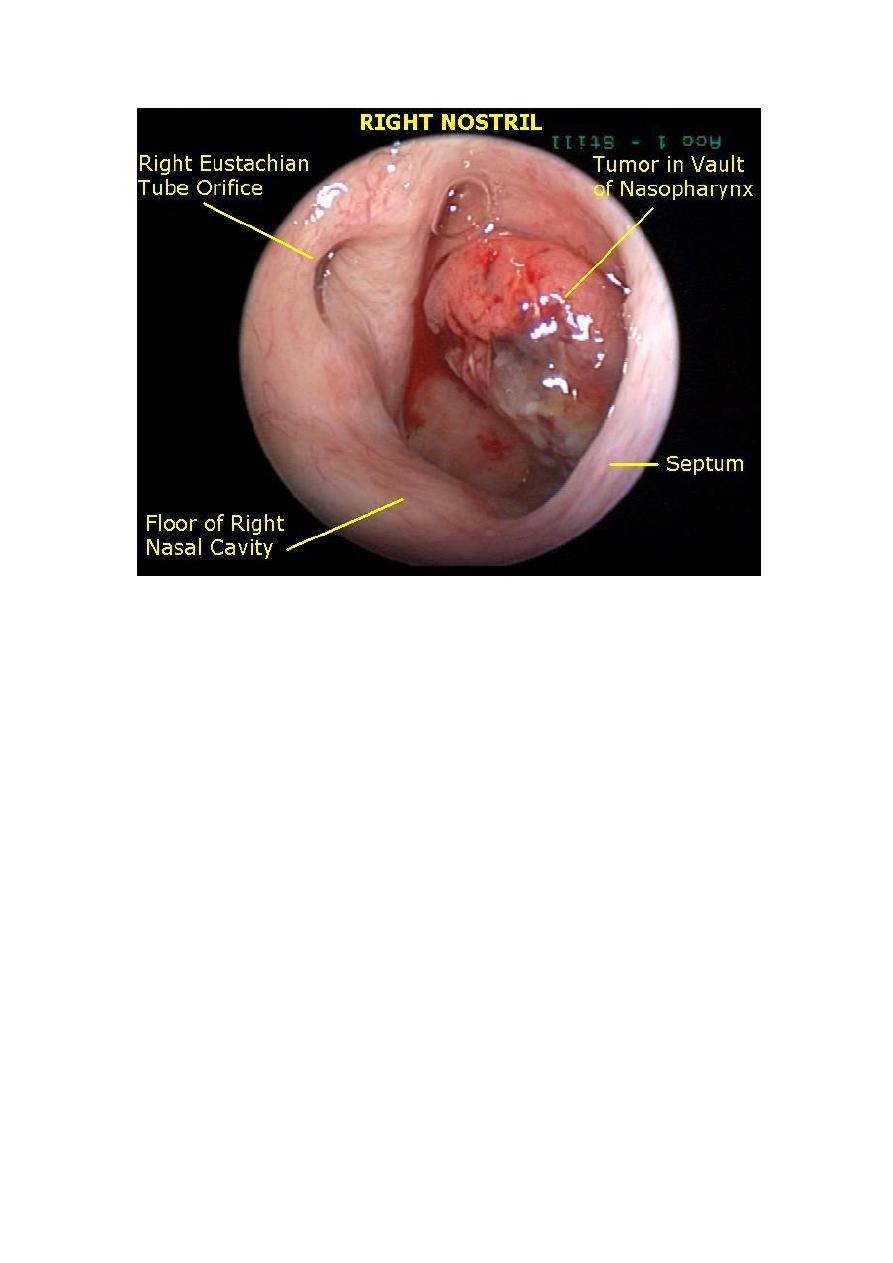
NASOPHARYNGEAL CARCINOMA:
This tumor characterized by: distinctive geographical distribution (in
African), a close anatomic relationship to lymphoid tissue, and an
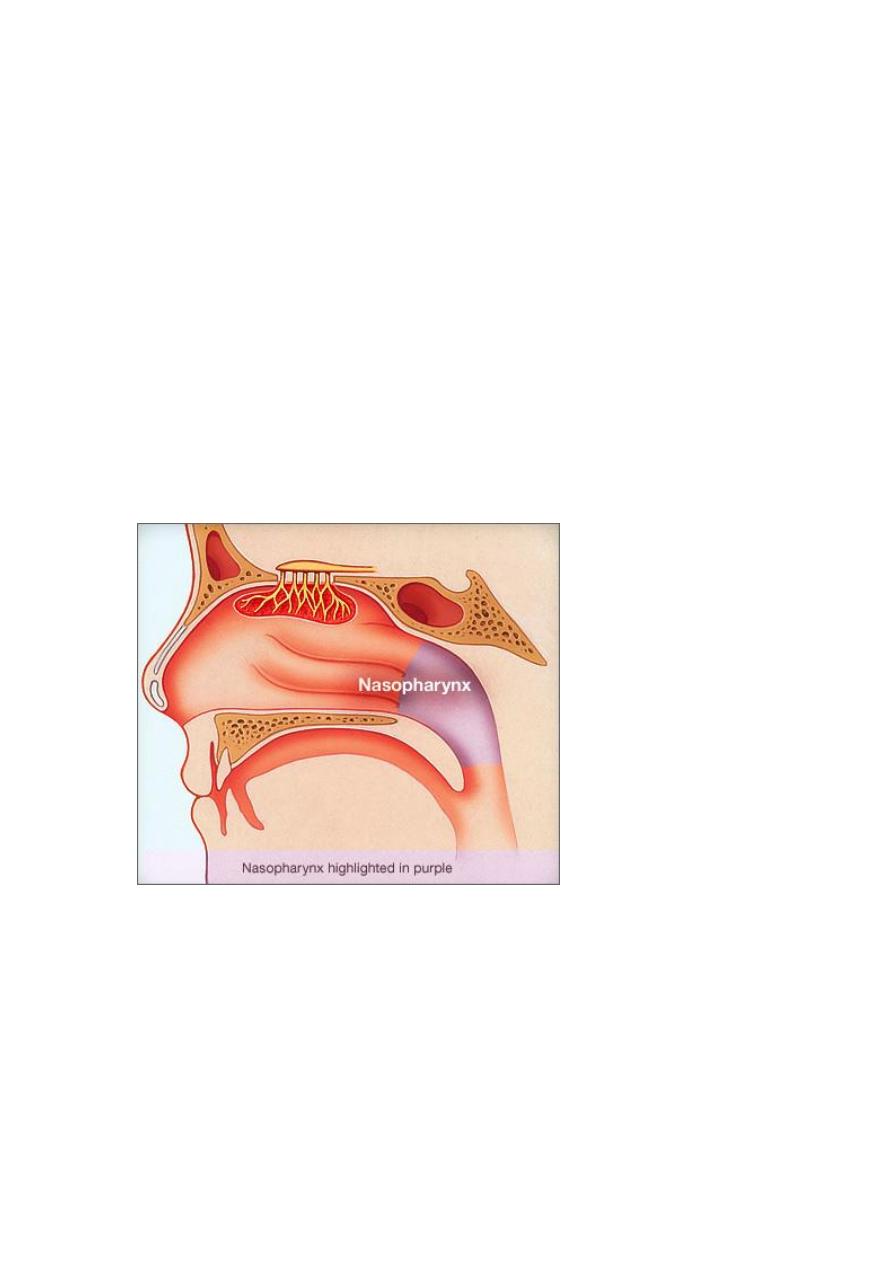
association with EBV. It takes three patterns; keratinizing scc,
nonkeratinizing scc, and undifferentiated carcinomas.
Primary nasopharyngeal carcinomas are often clinically occult for long
periods, and present as metastases in the cervical lymph nodes
radiotherapy is the standard modality of treatment .
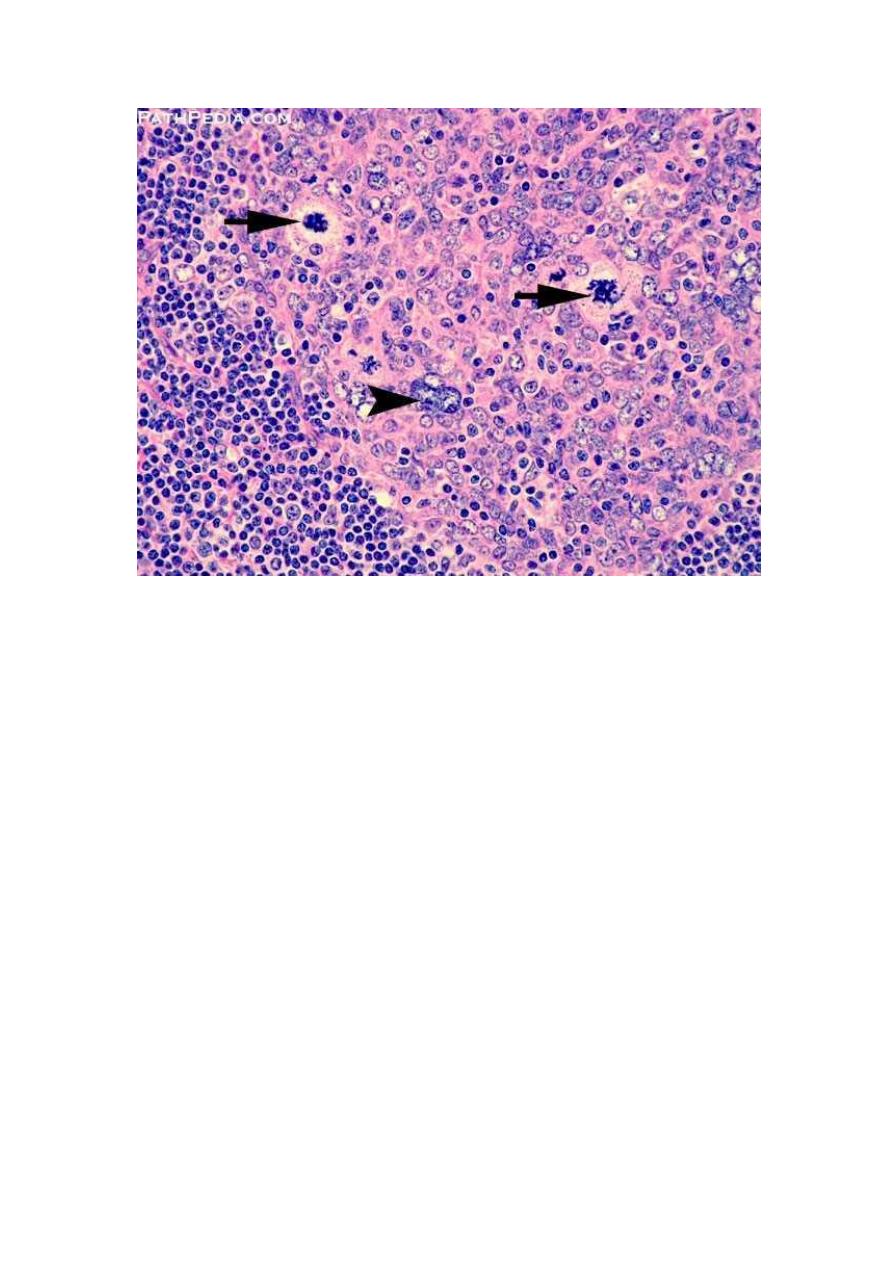
Morphology.
On histologic examination, the keratinizing and
nonkeratinizing squamous cell lesions resemble usual well-differentiated
and poorly differentiated squamous cell carcinomas arising in other
locations. The undifferentiated variant is composed of large epithelial
cells with oval or round vesicular nuclei, prominent nucleoli, and
indistinct cell borders disposed in a syncytium-like array admixed with
the epithelial cells are abundant, mature, normal-appearing lymphocytes,
which are predominantly T cells so give wrong old term of lympho
epithelioma.
LARYNX
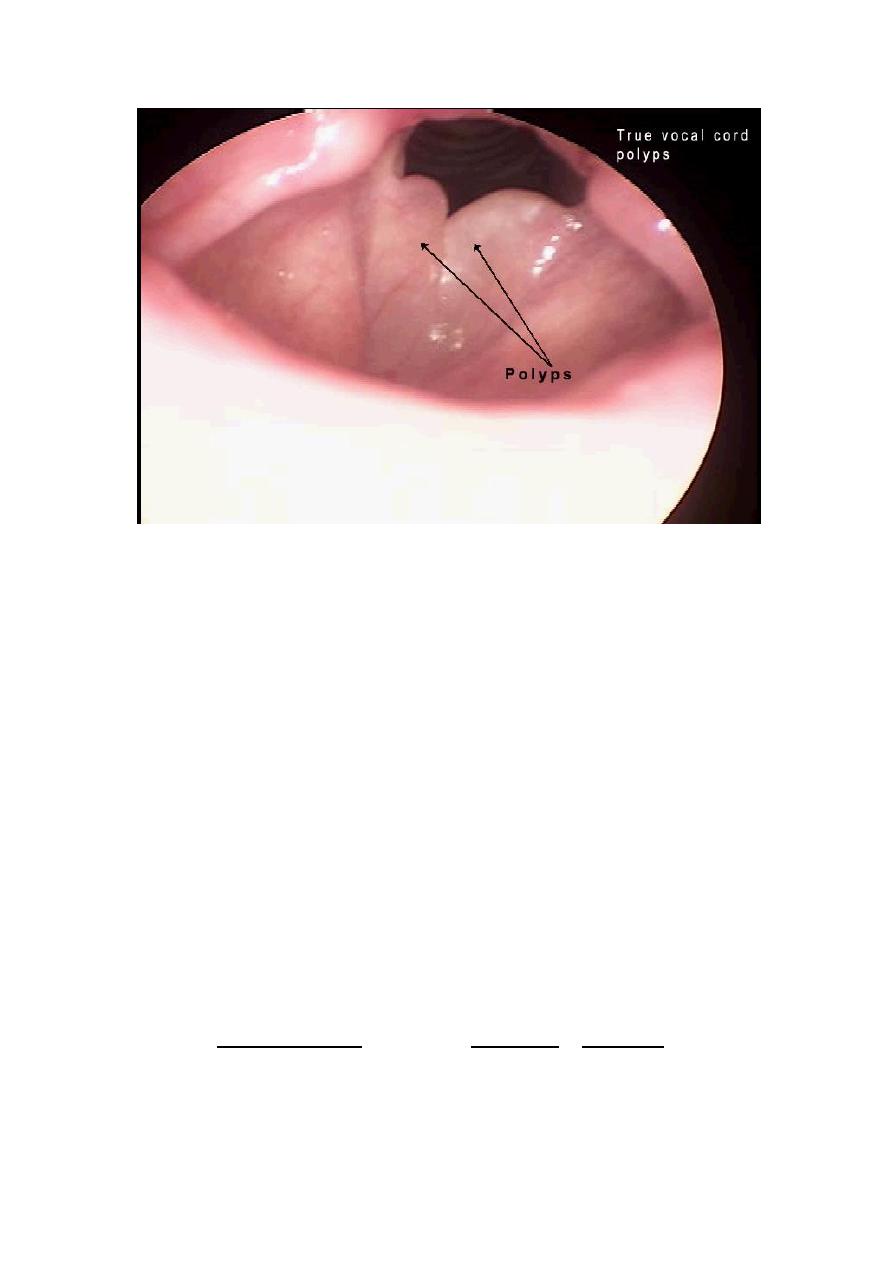
REACTIVE NODULES (VOCAL CORD NODULES AND POLYPS)
Reactive nodules, also called polyps, sometimes develop on the vocal
cords, most often in heavy smokers or in individuals who impose great
strain on their vocal cords (singers' nodules) . By convention, singers'
nodules are bilateral lesions and polyps are unilateral. Adults,
predominantly men, are most often affected. These nodules are smooth,
rounded, sessile or pedunculated excrescences, generally only a few
millimeters in the greatest dimension, located usually on the true vocal
cords. They are typically covered by squamous epithelium. The core of
the nodule is a loose myxoid connective tissue .
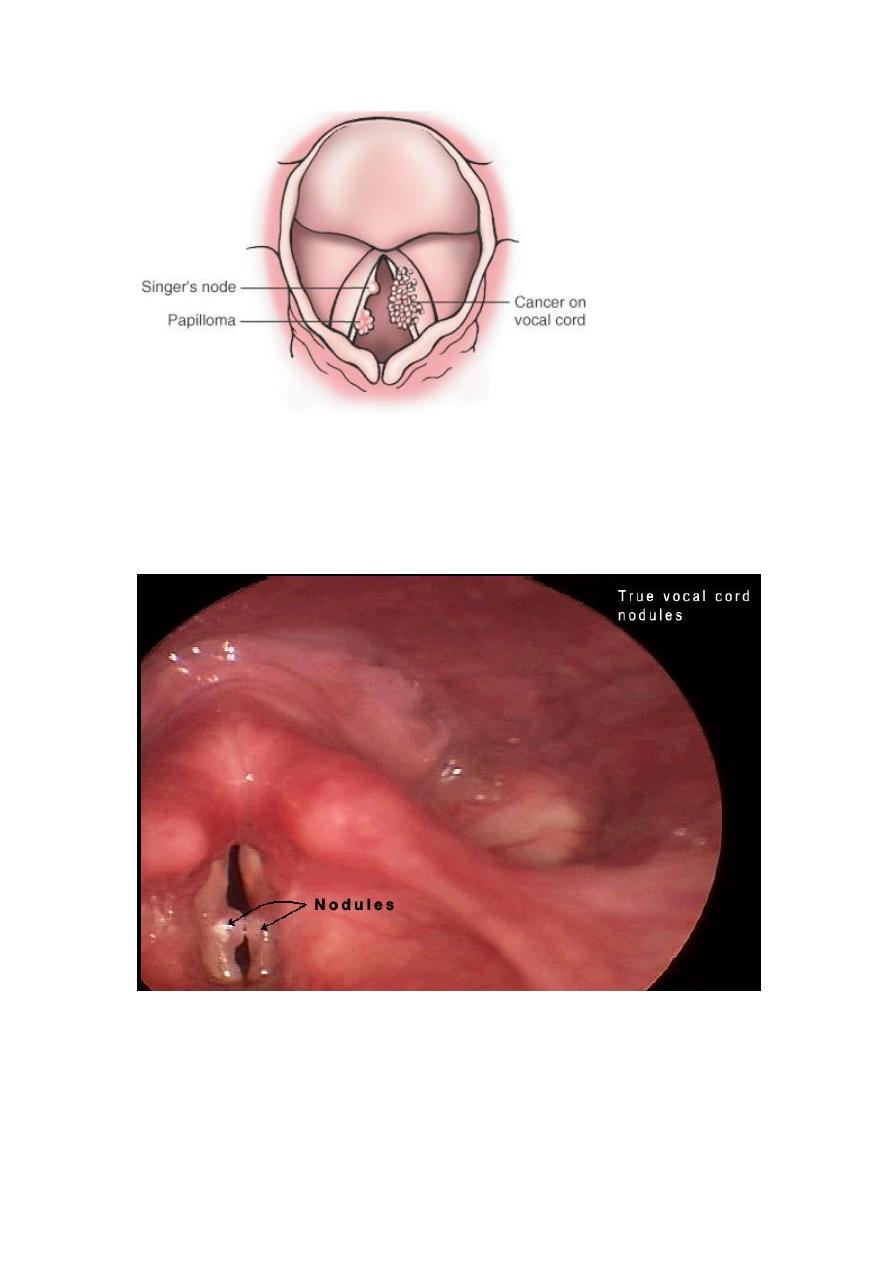
Diagrammatic comparison of a benign papilloma and an exophytic
carcinoma of the larynx to highlight their quite different appearances.
SQUAMOUS CELL PAPILLOMA AND PAPILLOMATOSIS
It is benign neoplasm usually on the true vocal cords. Usually single in
adults and multiple in children, the lesions are caused by HPV type 6 and
11, they have a risk of recurrence, cancerous transformation is rare.
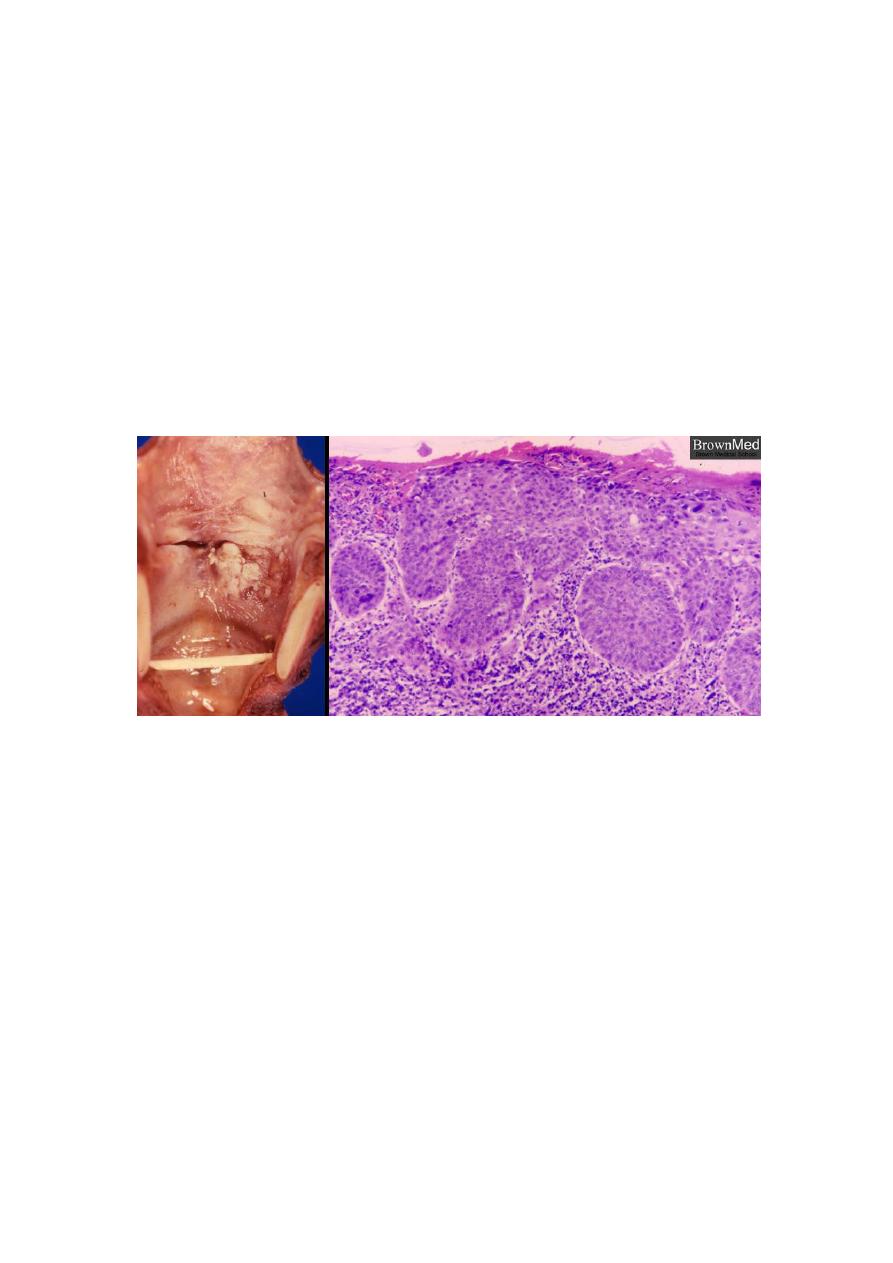
CARCINOMA OF THE LARYNX
Sequence of Hyperplasia-Dysplasia-Carcinoma.
A spectrum of epithelial alterations is seen in the larynx. They range from
hyperplasia, atypical hyperplasia, dysplasia, carcinoma in situ, to
invasive carcinoma.
Macroscopically :
the epithelial changes vary from smooth, white or
reddened focal thickenings, to irregular verrucous or ulcerated lesions
that are similar in appearance to carcinoma.
Risk factors:
1- tobacco smoke.
2- Alcohol is also clearly a risk factor. Together smoking and alochol
increase the risk substantially.
3- Other factors that may contribute to increased risk include
nutritional factors, exposure to asbestos, irradiation, and infection
with HPV.
Morphology. About 95% of laryngeal carcinomas are typical squamous
cell tumors. The tumor usually develops directly on the vocal cords, but
it may arise above or below the cords.
LUNGS
The lungs are ingeniously constructed to carry out their cardinal
function: the exchange of gases between inspired air and blood.
progressive branching of the bronchi forms bronchioles, which are
distinguished from bronchi by the lack of cartilage and submucosal
glands within their walls. Further branching of bronchioles leads to the
terminal bronchioles, which are less than 2 mm in diameter. The part of
the lung distal to the terminal bronchiole is called the acinus; it is roughly
spherical, with a diameter of about 7 mm. An acinus is composed of
respiratory bronchioles (which give off several alveoli from their sides),
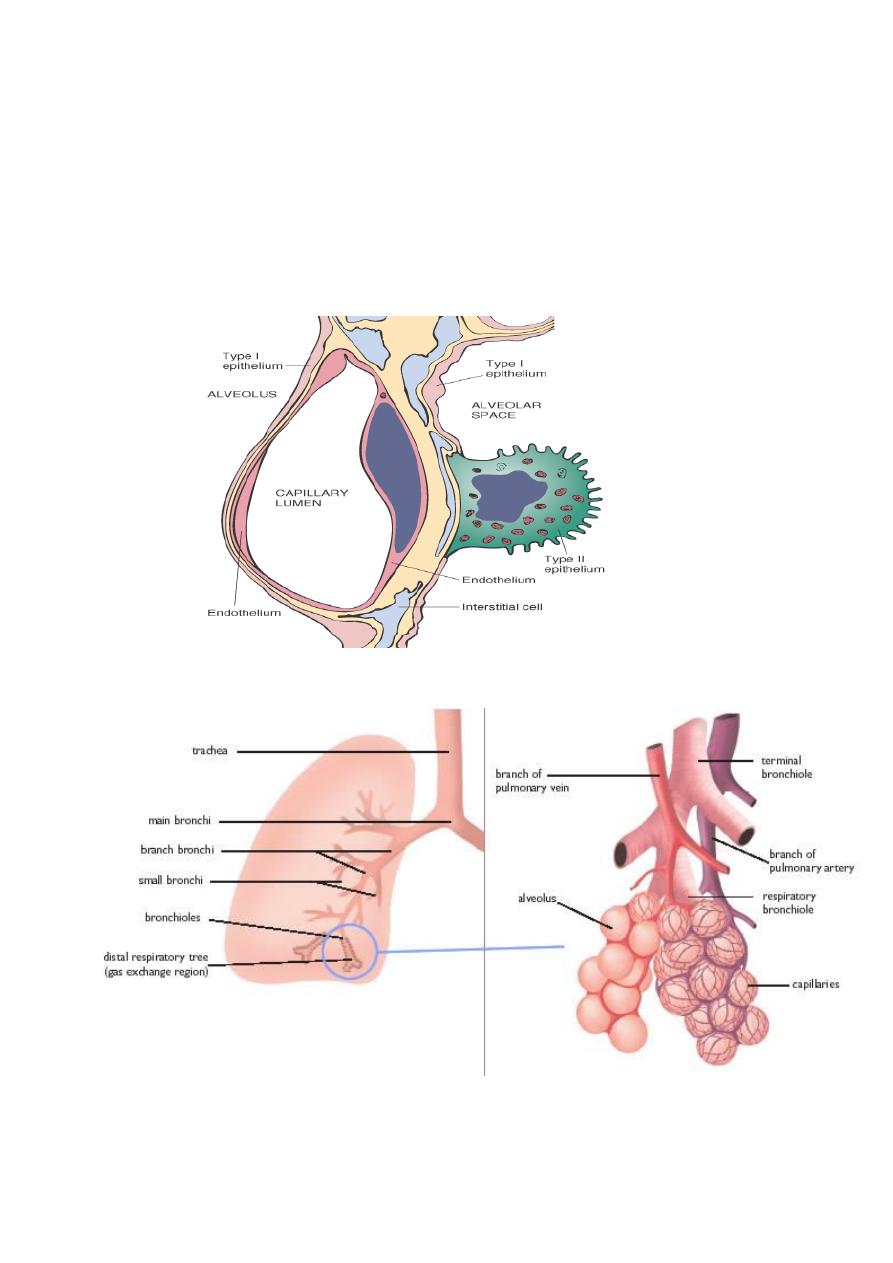
alveolar ducts, and alveolar sacs, the blind ends of the respiratory
passages, whose walls are formed entirely of alveoli, which are the site of
gas exchange. A cluster of three to five terminal bronchioles, each with
its appended acinus, is referred to as the pulmonary lobule. This lobular
architecture assumes importance in distinguishing the major forms of
emphysema.

Atelactasis (collapse):
It refers either to incomplete expansion of the lungs (neonatal atelactasis)
or to the collapse of previously inflated lung, producing areas of relatively
airless pulmonary parenchyma.
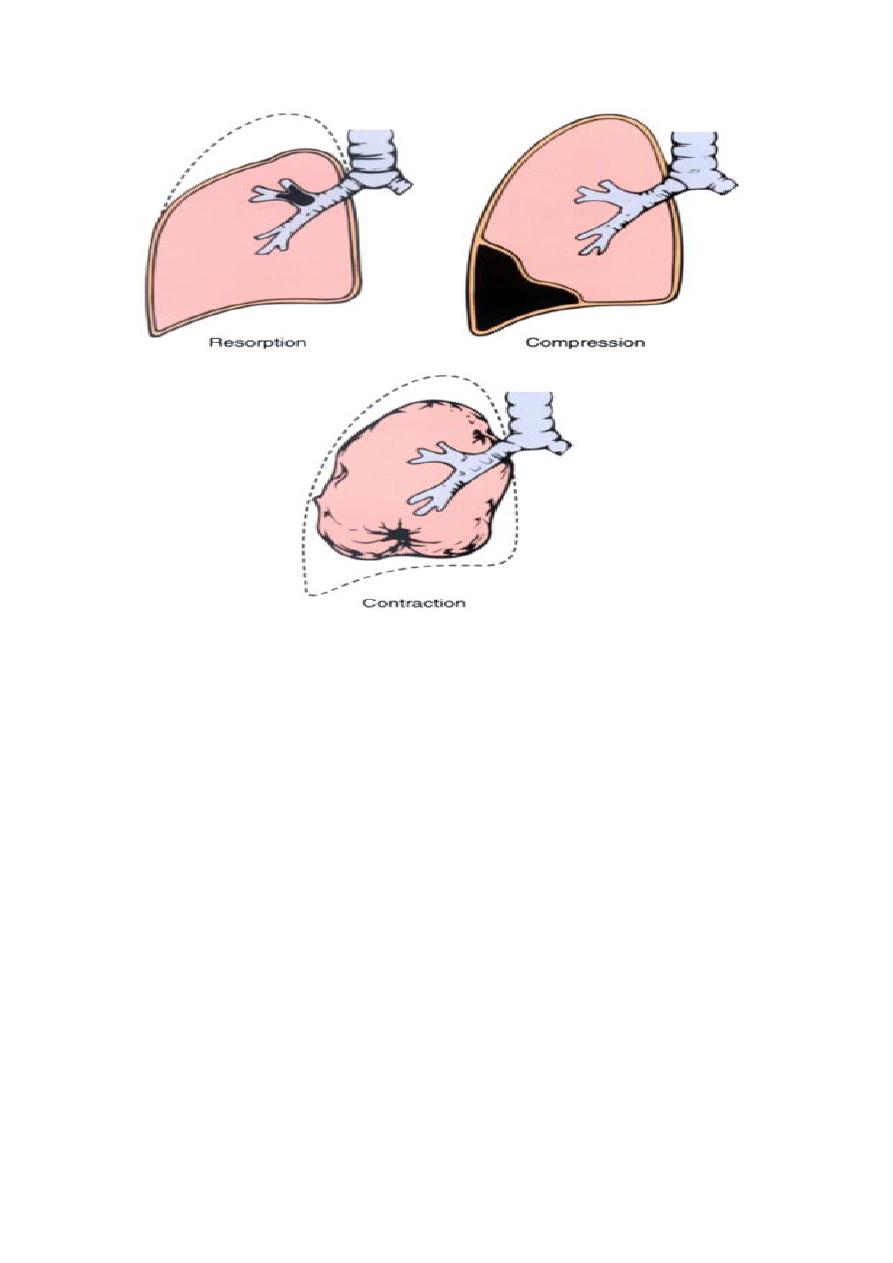
Acquired atelactasis.:
Encountered mainly in adults, divided into resorption (or obstruction),
compression, and contraction atelactasis.
RESORPTION ATE.:-
Is the consequences of complete obstruction of an airway, which leads to
resorption of the oxygen trapped in the dependent alveoli, since lung
volume is diminished, the mediastinum shifts toward the atelactatic lung.
COMPRESSION ATE.:-
Results whenever the pleural cavity is partially or completely filled by fluid
exudates, tumor, blood, or air, when air pressure impinges on and
threatens the function of the lung and mediastinum.
CONTRACTION ATELACTASIS:-
Occurs when local or generalized fibrotic changes in the lung or pleura
prevent full expansion.
significant atelactasis reduces oxygenation and predispose to infection.
it is a reversible disorder (except that caused by contraction).