DR. ALI ALIBRAHIMI
M.B.Ch.BChest examination
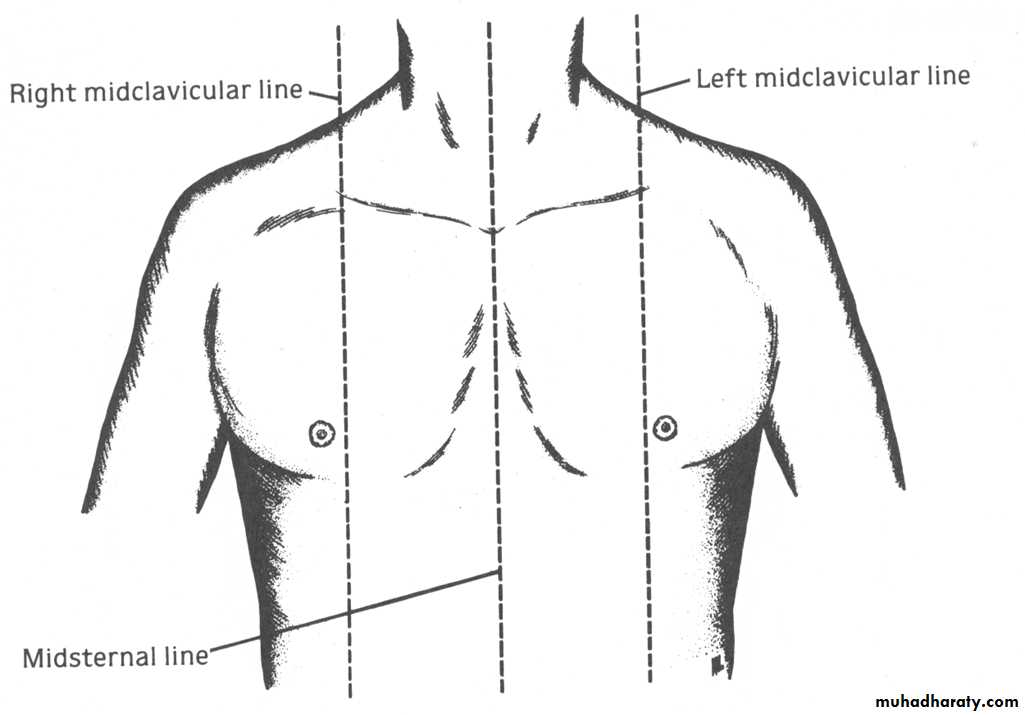
Chest topography\ anterior aspect
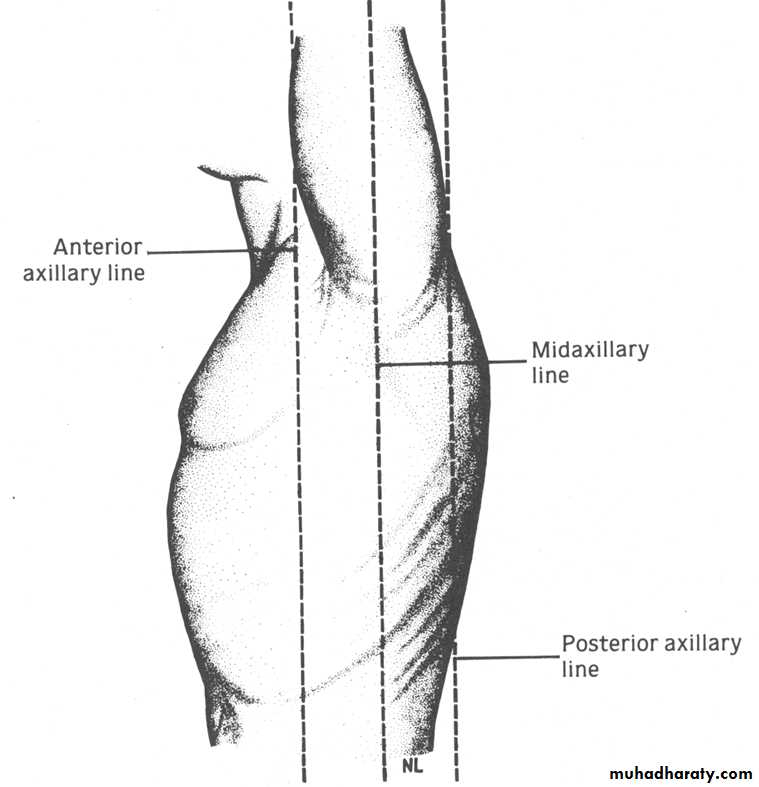
Chest topography\ lateral aspect
Skeleton of any clinical examination is based on :
1- INSPECTION2- PALPATION
3- PERCUSSION
4- AUSCULTATION
1- inspection:
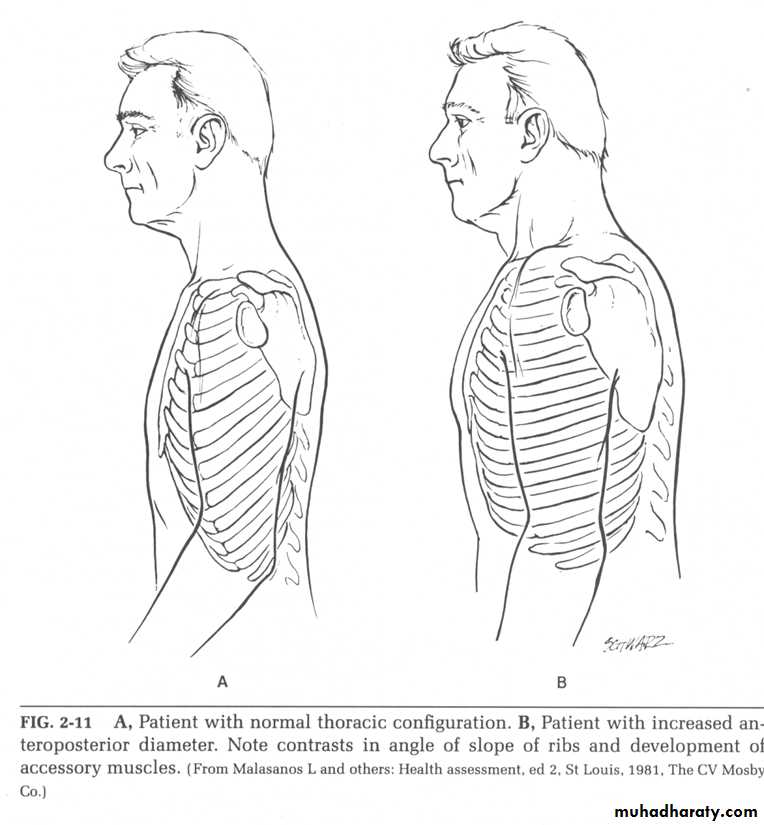
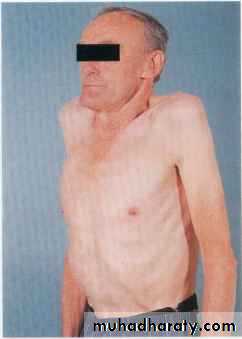
A- look to the chest , normally should be symmetrical and elliptical transverse to AP diameter should 7:5 cm , barrel-shaped chest seen in emphysema
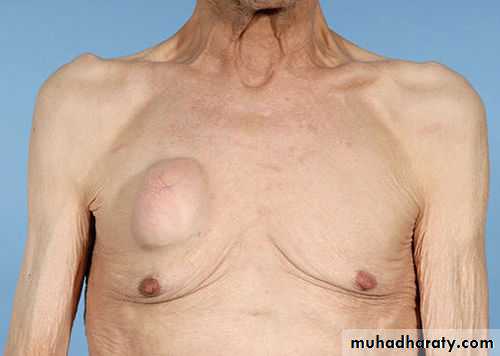
B- look for any scar from previous lung or heart surgery or any swelling marks or subcutaneous lesion eg; lipoma
C-look for any vascular anomalies eg dilated superficial veins(telengeictasia) occur in svc obstruction
D- calculate the respiratory rate (12-20 c\min)




2- palpation :
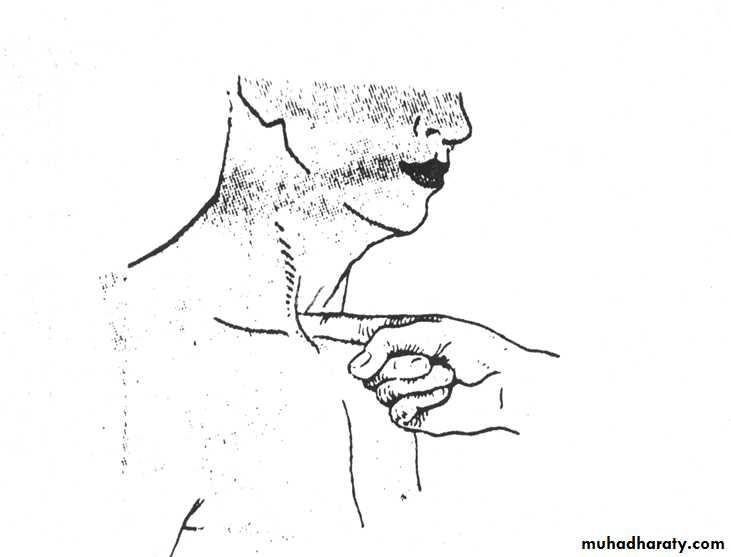
Palpate for any tenderness, position of mediastinum and detect the chest expansionDetermination of position of mediastinum by localizing the cardiac apex and position of trachea (by gently placing the tip of your right index finger in the suprasternal notch and palpate the trachea which is normally slightly deviated to the right ). Displacement of mediastinum occur in some cases eg ; pneumothorax
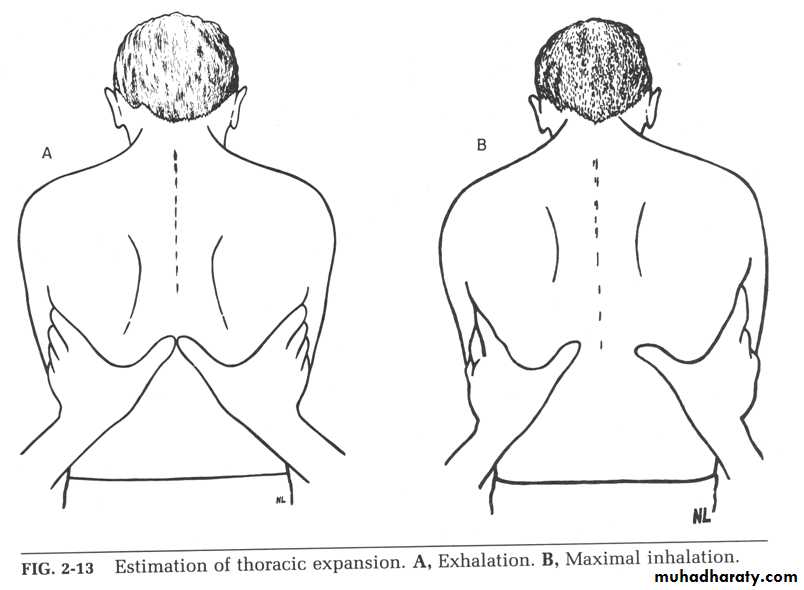
Chest expansion measured by placing the hands firmly on the back chest wall and extend your fingers around the sides of the chest , your thumbs should meet in the midline , during deep breath the thumbs should move at least 5 cm apart. Reduced chest expansion occur in some cases eg pleural effusion
3- percussion :
Percuss the lung apices . Percuss 3 symmetrical areas anteriorly (avoid percussion the midline), percuss 3 symmetrical areas laterally and percuss 4 symmetrical areas posteriorly ( avoid the scapula ).Note that you have to percuss in the intercostal spaces with your finger at a right angle
Possible findings are :
Resonance normal
Dullness increased density eg sold organ,mass
Stony dullness fluid filled eg pleural effusion
Hyper resonance decreased density eg pneumothorax

4- Auscultation
Auscultate while the subject taking deep breath through an open mouth. Compare both sides alternately. Listen : anteriorly from above the clavicle down to the 6th rib , laterally from the axilla to the 8th rib and posteriorly down to the level of 11th rib. Asses the quality and amplitude of the breath sound, identify the gap between inspiration and expiration and listen for added sound eg; crepitation , wheeze , pleural friction rubBreath sound:
A-normal vesicular breathing; caused by turbulent flow in large airway, the sounds is more intense in inspiration followed by expiration which is less intense and shorter
B- Bronchial breathing; is higher pitch sound with a hollow or blowing quality(similar to that heard over the trachea and larynx during normal breathing). The sound is similar in length and intensity in both inspiration an expiration with the presence of gap between the 2 phases. It is heard in some conditions eg; pneumonia
Examination of the precordium
Precordium is the area of the chest overlying the heart . To examine the precordium we have to follow these steps1- Inspection: mean examination by looking. Inspection of precordium after exposure of the subject lie at 45 degree , we detect:
A- any chest deformity eg; kyphosis, scoliosis
B- any surgical scar eg; valve replacement
C-pulsation eg; apex beat especially in thin subjects (PMP)
2-palpation: mean examination by hands. Palpation of the precordium by the following steps ;
1- lay the whole hands flat on the chest to get general impression about the cardiac activity
2- localize the apex beat, to detect any displacement eg; pneumothorax. And to detect character of apex beat, normally it is gentle , well localized and briefly lift the palpating finger
***HOW TO LOCALIZE APEX BEAT a-identify the sternal angle by count the intercostal spaces c-apex beat lies at 5th intercostal space within the midclavicular line.
3- percussion: rarely used in examination of precordium.
4- Auscultation examination using medical stethoscope with 2 surfaces: bell to detect high pitch sound eg first and second heart sound, and diaphragm to examine low pitch sound eg; third heart sound.
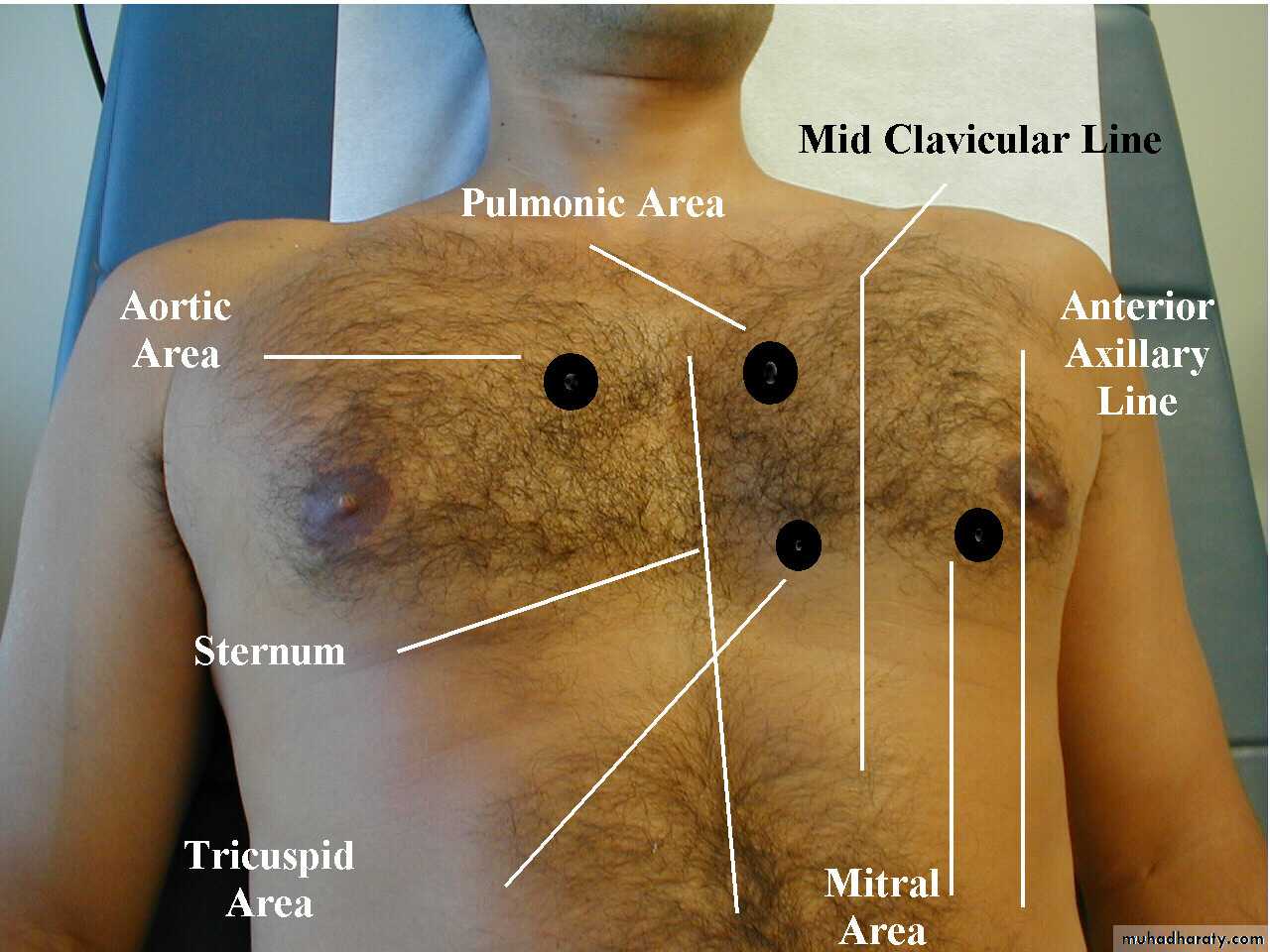
***AUSCULTATORY AREA
1- aortic area; lies in right 2nd ICS close to the sternal edge
2- pulmonary area ; lies in left in 2nd ICS close to sternal edge
3- tricuspid area: just to the left lower end of the sternum
4- mitral area ( apex beat); at left 5th ICS in MCL
Auscultation to detect heart sounds(S1, S2),any extra beat sounds (S3
, S4), or any added sounds murmur(sound of turbulent blood flow in the heart )
HEART SOUNDS
S1 (LUB) caused by closure of MV and TVS2 (DUB) caused by closure of AV and PV
S3 due to rapid ventricular filling
S4 pathological due to forceful atrial
contraction
55 yrs old male presented to the outpatient clinic complaining from chest pain and palpitation for 2 hours duration associated with SOB and poor exercise tolerance, he s known case of HTN,CHF and DM however O\E ;
Conscious and oriented and Temperature 38.5
Soft abdomen
PR 105, BP 110\60 , SPO2 96% , Chest exam revealed
Normal chest contour and Presence of bluish patches over the chest
Chest auscultation shows; vesicular breathing and bilateral basal crepitation and rhonchi
Precordial exam shows ; faint S1 , soft S2, S3 and early systolic murmur
1- mention 4 abnormal auscultatory notes
2- what do we mean by murmur? How could be generated ?