Medicine Lecture 4th Year 14-11-2016 Dr.Osamah Muwafk
1
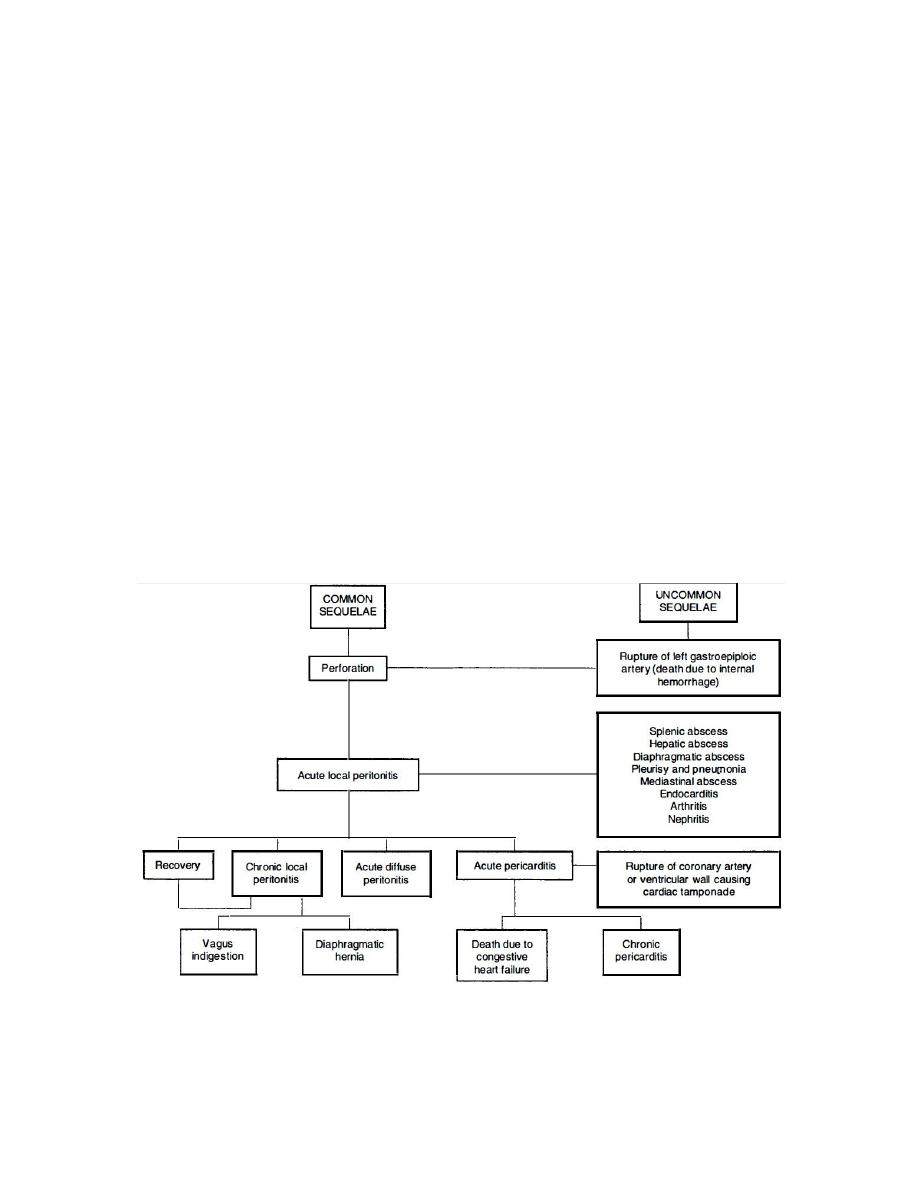
TRAUMATIC RETICULOPERITONITIS:
Perforation of the wall of the reticulum by a sharp foreign body
initially produces an acute local peritonitis, which may spread to
cause acute diffuse peritonitis or remain localized to cause
subsequent damage, including vagal indigestion and diaphragmatic
hernia.
Sequelae of the penetrating foreign body may proceed beyond
the peritoneum and cause involvement of other organs resulting in:
1. pericarditis,
2. cardiac tamponade
3. pneumonia
4. pleurisy and mediastinitis
5. hepatic, splenic or diaphragmatic abscess.
Sequelae of traumatic perforation of the reticular wall

Medicine Lecture 4th Year 14-11-2016 Dr.Osamah Muwafk
2
Etiology and Epidemiology :
1. Ingestion of metallic by the animal and located in the
reticulum
2. Penetration of reticulum by foreign objects such as nails and
pieces of wire, including tire wire
3. Adult dairy cattle are most commonly affected
4. The incidence is low in sheep and goats.
Pathogenesis:
1. Lack of oral discrimination by cattle leads to the ingestion of
foreign bodies that would be rejected by other species.
2. Swallowed foreign bodies may lodge in the upper esophagus
and cause obstruction
3. or in the esophageal groove and cause vomiting
4. in most instances they pass to the reticulum
5. honeycomb-like structure of the reticulum provides many
sites for fixation of the foreign body
6. contractions of the reticulum are sufficient to push a sharp-
pointed object through the wall
7. acute local peritonitis
8. fibrous adhesions
9. motility of the reticulum is restored and the animal may
recover fully
10.
reticulum becomes adherent to varying degrees to the
abdominal floor and diaphragm this results in decreased
reticular motility
11.
Persistent local peritonitis
12.
Spread of the inflammation causing generalized or
diffuse peritonitis may occur in cows that calve at the time of
perforation and in cattle that are forced to exercise

Medicine Lecture 4th Year 14-11-2016 Dr.Osamah Muwafk
3
Clinical Findings:
1) acute local peritonitis:
1) Sudden with complete anorexia and a marked drop in milk
yield
2) Subacute abdominal pain
3) reluctant to move and does so slowly.
4) Walking, particularly downhill, is often accompanied by
grunting
5) Arching of the back
6) Defecation and urination cause pain
7) A moderate systemic reaction is common
8) Rumination is absent and reticulorumen movements are
markedly depressed and usually absent
9) Pain can be elicited by deep palpation of the abdominal wall
just caudal to the xiphisternum
2) Chronic local peritonitis
1. the appetite and milk yield do not return to normal after
prolonged therapy with antimicrobials
2. The body condition is usually poor
3. the feces are reduced in quantity and there is an
increase in undigested particles
3) Acute diffuse (generalized) peritonitis:
1. profound toxemia within a day or two of the onset of
local peritonitis
2. Alimentary tract motility is reduced
3. mental depression is marked t
4. he temperature is elevated or subnormal in severe
cases
5. heart rate increases to 100-120/min

Medicine Lecture 4th Year 14-11-2016 Dr.Osamah Muwafk
4
6. painful grunt may be elicited by deep digital palpation
at almost any location over the ventral abdominal wall
7. recumbency and depression
Clinical Pathology
1. Hemogram:
A. In acute local peritonitis
1. a neutrophilia (mature neutrophils above 400/μL)
2. left shift (immature neutrophils above 200/μL)
regenerative left shift
B. In acute diffuse peritonitis
1. aleukopenia (total count below 4000/μL)
2. with a greater absolute number of immature
neutrophils
than
mature
neutrophils
(degenerative left shift)
C. Plasma protein and fibrinogen
D. Abdominocentesis and peritoneal fluid
Other diagnosis methods:
1) metal detection: ferrous metallic foreign bodies can be
detected with metal detectors
2) laparoscopy radiography of cranial abdomen and reticulum
3) ultrasonography of the reticulum
Necropsy findings:
A. Localized traumatic reticuloperitonitis is characterized by
varying degrees of locally extensive fibrinous adhesions
between the cranioventral aspects of the reticulum and the
ventral abdominal wall and the diaphragm

Medicine Lecture 4th Year 14-11-2016 Dr.Osamah Muwafk
5
Treatment
A. Conservative medical therapy:
Antimicrobials: Penicillin or broad-spectrum antimicrobials
given parenterally daily for 3-5 days
B. Rumenotomy
C. Drainage of reticular abscesses
VAGUS INDIGESTION:
Etiology:
1. complications of traumatic reticuloperitonitis:
1) vagal nerve injury
2) reticular adhesions
Pathogenesis:
1) dorsal vagal nerve injury
2) achalasia of the reticulo-omasal orifice (anterior stenosis)
3) inhibited the passage of ingesta from the reticulorumen into
the omasum and abomasum
4) distension of the rumen with pasty and/or frothy contents
5) injury of the pyloric branch of the ventral vagus nerve
resulted in achalasia of the pylorus (posterior stenosis) and
inhibited the flow of ingesta from the abomasum resulting in
abomasal impaction
6) in reticular adhesions a mechanical impairment of reticular
motility and esophageal groove dysfunction
Clinical Findings:
1) Inappetence for several days or complete anorexia

Medicine Lecture 4th Year 14-11-2016 Dr.Osamah Muwafk
6
2) loss of body weight
3) An enlarged 'papple' –shaped abdomen
4) Dehydration and electrolyte imbalance with metabolic
alkalosis
5) Enlarged rumen palpable on rectal examination
6) Scant feces with an increase in undigested particles
7) Vital signs within the normal range
8) Inadequate response to treatment
Treatment:
1) Rumen lavage
2) Rumenotomy