بسم الله الرحمن الرحيم
ACUTE KIDNEY INJURY
Lecture by :
Dr. Zaidan Jayed Zaidan
Acute kidney injury (AKI), also referred to as acute renal failure, describes the situation where there is a sudden and often reversible loss of renal function, which develops over days or weeks and is usually accompanied by a reduction in urine volume. Approximately 7% of all hospitalised patients and 20% of acutely ill patients develop signs of AKI.

Pathophysiology
In prerenal AKI, the kidney becomes damaged as the result of hypoperfusion, leading to acute tubular necrosis. Renal AKI may be caused by nephrotoxic drugs which can cause acute tubular necrosis and a similar histological picture to prerenal AKI or interstitial nephritis.The other common cause is glomerulonephritis, in which there is direct inflammatory damage to the glomeruli . Postrenal AKI occurs as the result of obstruction to the renal tract, with kidney damage arising as the result of back pressure..Clinical features
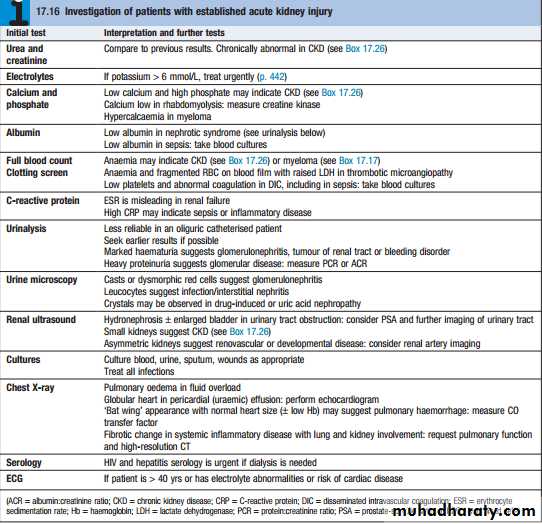
Early recognition and intervention is important in AKI; all emergency admissions to hospital should have renal function, blood pressure, temperature and pulse checkedon arrival and should undergo a risk assessment for the likelihood of developing AKI. This includes looking at coexisting diseases such as diabetes, vascular disease and liver disease, which make AKI more likely, as well as gathering information on drug treatments such as ACE inhibitors and NSAIDs, which may be associated with renal dysfunction. If a patient is found to have a high serum creatinine, it is important to establish whether this is an acute or acuteonchronic phenomenon, or a sign of chronic kidney disease. Previous measurements of renal function can be of great value in differentiating these possibilities.Pre-renal AKI
* hypotension
* signs of poor peripheral perfusion
* History of NSAID ingestion
* Concealed blood loss.
* Postural Hypotension
Renal AKI
Patients with glomerulonephritis usually demonstrate significant haematuria and proteinuria and may have clinical manifestations of an underlying disease,such as SLE or systemic vasculitis.
Post-renal AKI
Patients should be examined clinically to look for evidence of bladder enlargement and should also undergo imaging with ultrasound to detect evidence of obstruction above the level of the bladder. Postrenal AKI is usually accompanied by hydronephrosis, but this can be absent if the ureters are affected by fibrosis or malignancy, or if obstruction of the renal tract occurs in combination with a renal disorder such as acute tubular necrosis that causes reduced urinary flow.



Management

Immunosuppression:
Patients with glomerulonephritis may require immunosuppressive drugs , plasma infusion and plasma exchange. :Renal tract obstruction
In postrenal AKI, the obstruction should be relieved as
soon as possible. This may involve catheterisation in
urethral obstruction, or correction of ureteric obstruction
with a ureteric stent or percutaneous nephrostomy.
Renal replacement therapy:
Conservative management can be successful in AKI
with meticulous attention to fluid balance, electrolytes and nutrition, but renal replacement therapy (RRT) may
be required in patients who are not showing signs of
recovery with these measures.
THANK YOU FOR LISTENING