
Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
1
GLANDERS :
ETIOLOGY:
1. Burkholderia (Pseudomonas) mallei
EPIDEMIOLOGY
1. Glanders is restricted geographically to Eastern Europe, Asia
Minor, Asia, and North Africa
2. It was more widespread but has been eradicated from most
countries
3. Horses, mules, and donkeys are the species usually affected
4. Humans are susceptible and the infection is usually fatal
5. B. mallei is an obligate parasite and is readily destroyed by
light, heat, and the usual disinfectants
6. Infected animals or carriers that have made an apparent
recovery from the disease are the important sources of
infection
7. Chronic nodular lung lesions, which have ruptured into the
bronchi, infest upper airway passages and nasal or oral
secretions
8. Spread to other animals occurs mostly by ingestion
9. the cutaneous form appears to arise through contamination of
skin abrasions
10.
Horses tend to develop the chronic form, mules and
donkeys the acute form
11.
The disease is more likely when animals are in a
stressed state
12.
Zoonotic implications: infection may gain access
through skin abrasions to produce granulomatous disease and

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
2
pyemia or from inhalation of infectious material and the case
fatality is high
PATHOGENESIS:
1. Invasion occurs mostly through the intestinal wall
2. A septicemia (acute form) or bacteremia (chronic form) is set
up
3. Localization always occurs in the lungs but the skin and nasal
mucosa are also common sites
4. Other viscera may become the site of the typical nodules
5. Deaths in typical cases are caused by anoxic anoxia
CLINICAL FINDINGS:
A. Acute disease
1. There is a high fever
2. cough, and nasal discharge
3. rapidly spreading ulcers appearing on the nasal mucosa
4. nodules on the skin of the lower limbs or abdomen
5. Death due to septicemia occurs in a few days
B. Chronic disease
Three major manifestations are described:
1. Pulmonary
2. Skin
3. Nasal, although the chronic nasal and skin forms
commonly occur together
A. Pulmonary form of disease:
manifests as a chronic pneumonia with cough, frequent
epistaxis, and labored respiration
B. Nasal form of disease:

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
3
1) Lesions appear on the lower parts of the turbinates and
the cartilaginous nasal septum
2) They commence as nodules (1 cm in diameter), which
ulcerate and may become confluent
3) In the early stages there is a serous nasal discharge
which may be unilateral and which later becomes
purulent and blood stained
4) Enlargement of the submaxillary lymph nodes is a
common accompaniment
5) On healing, the ulcers are replaced by a characteristic
stellate scar
C. The skin form
1) is characterized by the appearance of
subcutaneous nodules (1-2 cm in diameter)
2) which soon ulcerate and discharge pus of the
color and consistency of dark honey
3) Thickened fibrous lymph vessels radiate from
the lesions and connect one to the other
D. Animals affected with the chronic form are usually ill
for several months
CLINICAL PATHOLOGY:
1) Mallein test
2) The complement fixation test on serum
3) Demonstration of the organism
NECROPSY FINDINGS:
1) In the acute form there are multiple petechial hemorrhages
throughout the body and a severe catarrhal

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
4
bronchopneumonia with enlargement of the bronchial lymph
nodes
2) chronic form, the lesions in the lungs take the form of miliary
nodules, Ulcers are present on the mucosa of the upper
respiratory tract, Nodules and ulcers may be present in the
skin and subcutis of the limbs
DIFFERENTIAL DIAGNOSIS:
1) Epizootic lymphangitis
2) Ulcerative lymphangitis
3) Sporotrichosis
4) Melioidosis
5) Other causes of pneumonia
TREATMENT:
1. Sodium sulfadiazine has been highly effective
2. Treatment for a period of 20 d was necessary to effect 100%
recovery
CONTROL:
1. Complete quarantine of affected premises is necessary
2. Clinical cases should be destroyed
3. remainder subjected to the mallein test at intervals of 3 weeks
until all reactors have been removed
4. A vigorous disinfection program for food and water troughs
and premises generally should be instituted to prevent spread
while eradication is being carried out
5. Restriction of the movement of horses should be instituted
and the mallein test carried out in horses which may have had
contact with the infected group

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
5
EPIZOOTIC LYMPHANGITIS
(PSEU DOGLANDERS, EQUINE BLASTOMYCOSIS, EQUINE
HISTOPLASMOSIS)
ETIOLOGY
1. A fungus, Histoplasma capsulatum var. farciminosum, a
dimorphic
2. Fungal soil saprophyte
EPI DEM IOLOGY:
1. Occurs as outbreaks in horses, donkeys and mules
2. Recorded in parts of Iran, Asia, India, Northern Africa, and
the Mediterranean littoral
3. Most outbreaks occur in autumn and winter
4. Occur if large numbers of horses are gathered together for
military or other purposes
5. Transmission of the fungal spores by direct contact or on
bedding, grooming utensils, horse blankets
6. Biting flies may play a role in the transmission of the disease
7. Infection is reported in humans
PATHOGENESIS
1. After gaining entry through wounds
2. the fungus invades subcutaneous tissue
3. sets up a local granuloma or ulcer
4. spreads along the lymphatic vessels
5. inoculation of the organism into the eye by biting flies lead to
the ocular form of the disease
CLI NICAL FINDINGS
Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
6
1. primarily an ulcerating, suppurative, pyogranulomatous
dermatitis
2. lymphangitis
3. An ocular form of the disease is characterized by an
ulcerating conjunctivitis
4. In the cutaneous form
a) an indolent ulcer develops at the portal of entry
b) making its appearance several weeks to 3 months
after infection occurs
c) A spreading dermatitis and lymphangitis
d) evident as corded lymphatics with intermittent
nodules, develops
e) Nodules rupture, discharging a thick creamy pus
f) Local lymph nodes also enlarge and can rupture
g) Thickening of the skin in the area and general
swelling of the whole limb are common
h) The lesions are quite painless
i) The lesions usually develop on the limbs, particularly
about the hocks
5. Ocular involvement is manifested by keratitis and
conjunctivitis
6. The disease is chronic, persisting for 3-12 months
7. Spontaneous recovery occurs and immunity is solid
CLINICAL PATHOLOGY:
1. Gram-positive, yeast-like cells, with a characteristic double-
walled capsule, are easily found in discharges
2. The organisms are located both extracellularly and
intracellularly in giant cells and macrophages
NECROPSY FIN DINGS:

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
7
1. Lesions are usually confined to the skin, subcutaneous
tissues, and lymph vessels and nodes
DIFFER ENTIAL DIAGNOSIS:
2. Glanders (Burkholderia mallei)
3. Ulcerative lymphangitis (Corynbacterium
pseudotuberculosis)
4. Sporotrichosis (Sporothrix schenckil)
5. Histoplasmosis (Histoplasma capsulatum)
TREATM ENT:
6. Sodium iodide is administered as a 10% solution at a dose of
1 mL per 5 kg intravenously once weekly for 4 weeks
7. Or Amphotericin is administered at a dose of 0.2 mg/kg body
weight every 48 hours for 3 treatments
STRANGLES (EQUINE DISTEM PER)
ETIOLOGY
1. Streptococcus equi subsp. equi (S. equi)
2. is a Gram-positive coccobacillus
EPIDEMIOLOGY
1. Strangles occurs in horses, donkeys, and mules worldwide.
2. Outbreaks are seen in breeding farms and in polo and racing
stables, when the infection is introduced by new arrivals
3. Strangles can affect horses of any age
4. although morbidity rate is usually greater in younger horses
such as foals and weanlings
5. The case-fatality rate without treatment is about 9%

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
8
6. Transmission from infected horses, either directly or by
fomites
Importance:
1. Strangles is one of the most important diseases of horses in
developed countries,
2. because of the deaths
3. because of the disruption of the management of commercial
horse establishments
4. the time necessary to treat affected horses
PATHOGENESIS:
1. M proteins are associated with S. equi adhesion to oral, nasal,
and pharyngeal tissues
2. Bacteria lodge in the pharyngeal and tonsillar lymphoid
tissues where they multiply rapidly
3. Bacteremia may occur
4. Swelling and abscessation of these lymph nods due to
migration of neutrophils into these lymph nodes
5. Death is usually due to pneumonia caused by aspiration of
infected material or asphyxiation secondary to upper airway
swelling
6. Metastatic infection of the heart valves, brain, eyes, joints,
and tendon sheaths or other vital organs may occur and cause
a chronic illness and eventual death
CLINICAL FINDINGS:
C. Acute disease
1. After an incubation period of 1-3 weeks

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
9
2. Suddenly develops with complete anorexia, epression,
fever (39.5-40.soC, 103-105°F)
3. mucopurulent nasal discharge
4. Abscessation of submandibular and retropharyngeal
lymph nodes
5. severe pharyngitis and laryngitis
6. Lymphadenopathy becomes apparent as the
submandibular lymph nodes enlarge and palpation
elicits a painful response
7. Swelled lymph nod may rupture to discharge thick,
cream-yellow pus
8. Swelling of the retropharyngeal lymph nodes may
cause obstruction of the oro- and nasopharynx with
subsequent respiratory distress and dysphagia
9. Purpura hemorrhagica can occur as a sequela to S.
equi infection
CLINICAL PATHOLOGY
1. Leukocytosis with a neutrophilia
2. Hyperfibrinogenemia
3. Hyperproteinemia
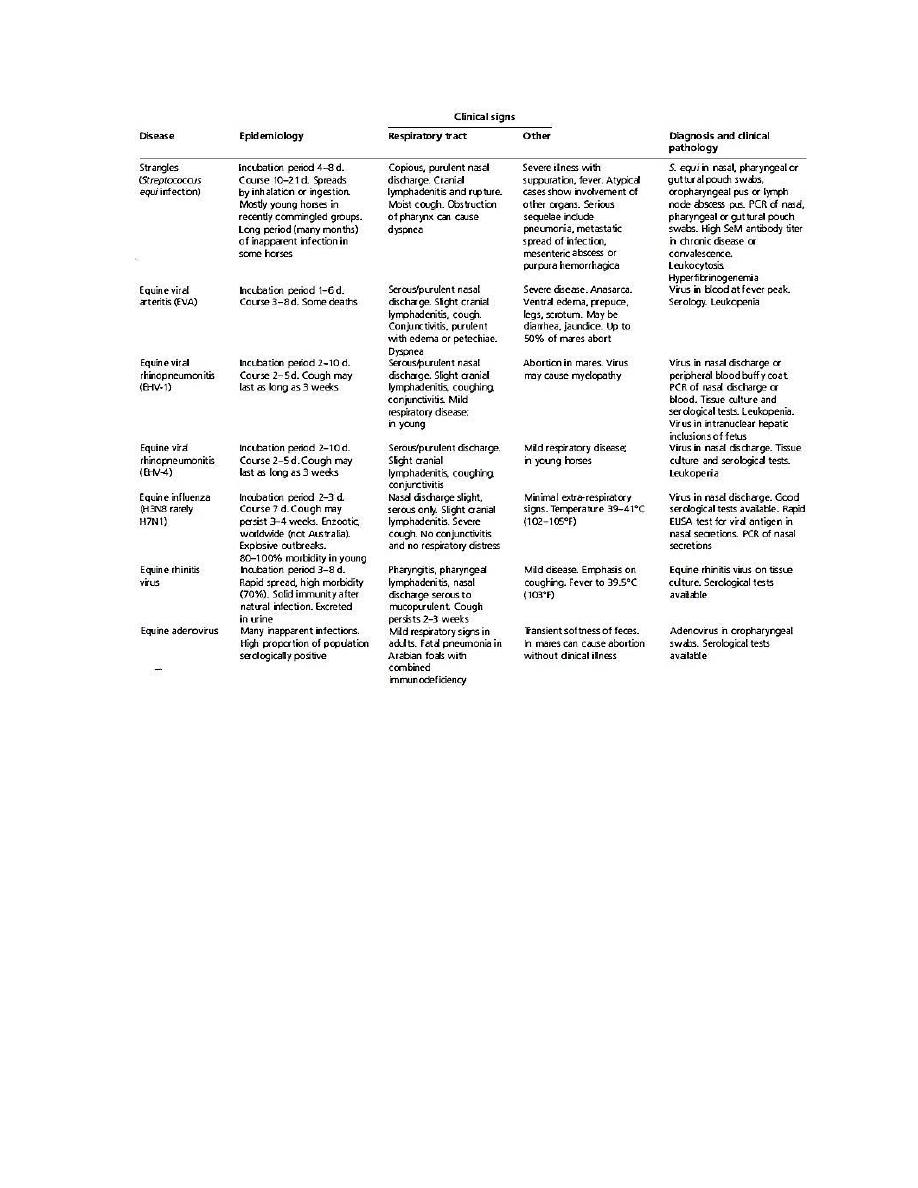
DIFFERENTIAL DIAGNOSIS:
Causes of pneumonia as in the table :
Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
10
TREATMENT
1. Treatment for S. equi infection depends on the stage of the
disease
2. The specific treatment of choice is penicillin
3. procaine penicillin G (22000 IV/kg IM every 12 h)
4. or potassium or sodium penicillin G(22000 IU/kg IV every 6
h)
5. or Tetracycline (6.6 mg/kg IV every 12-24 h)
6. or sulfonamide-trimethoprim combinations (15-30 mg/kg
orally or intravenously every12 h)

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
11
7. administration of nonsteroidal anti-inflammatory drugs
(NSAIDs) to reduce swelling and provide pain relief
8. application of hot poultices to encourage rupture of abscesses
9. provision of intravenous hydration in animals unable to drink
10. wound care
U LCERATIVE LYMPHANGITIS OF HORSES
ETIOLOGY:
1. Corynebacterium pseudotuberculosis causes the classical
disease
2. It is a soil-borne organism that gains access to tissue through
wounds or insect bites
3. Transmission by direct contact between infected and
uninfected animals
4. by mechanical transmission by houseflies or other diptera
PATHOGENESIS
1. Infection of skin wounds
2. Invasion of lymphatic vessels
3. Development of abscesses along their course
4. Generalized lymph node involve mentis unusual
5. The organism possesses a cytotoxic surface lipid coat that
appears to facilitate intracellular survival and abscess
formation
6. Produces a phospholipase exotoxin that increases vascular
permeability and has an inhibitory effect on phagocytes
Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
12
CLINICAL FINDINGS:
1. Initial wound infection
2. Swelling and pain of the pastern, often sufficient to
cause severe lameness
3. Nodules develop in the subcutaneous tissue,
particularly around the fetlock
4. Infection of lymphatic vessels and the development of
abscesses along their course
5. Spread to other subcutaneous sites on all parts of the
body
6. These may enlarge to 5-7 cm in diameter and rupture
to discharge a creamy green pus
7. The resulting ulcer has ragged edges and a necrotic
base
8. Lymphatics draining the area become enlarged and
hard and secondary ulcers may develop along them
9. Lesions heal in 1-2 weeks
10. Fresh crops may occur and cause persistence of the
disease for up to 12 months
DIFFERENTIAL DIAGNOSIS:
1. Epizootic lymphangitis
2. Glanders
3. Sporotrichosis
4. Rhodococcus equi
TREATMENT:
1. Aminoglycoside group
2. but systemic treatment of infected animals does not affect the
recovery period

Infectious Lecture 4th Year 3-1-2017 Dr.Osamah Muwafk
13
3. Local treatment of ulcers is the usual and most effective
procedure