


• Facial fractures
طب اسنان \ خامس اسنانجراحة فم \ د. وفاء م9
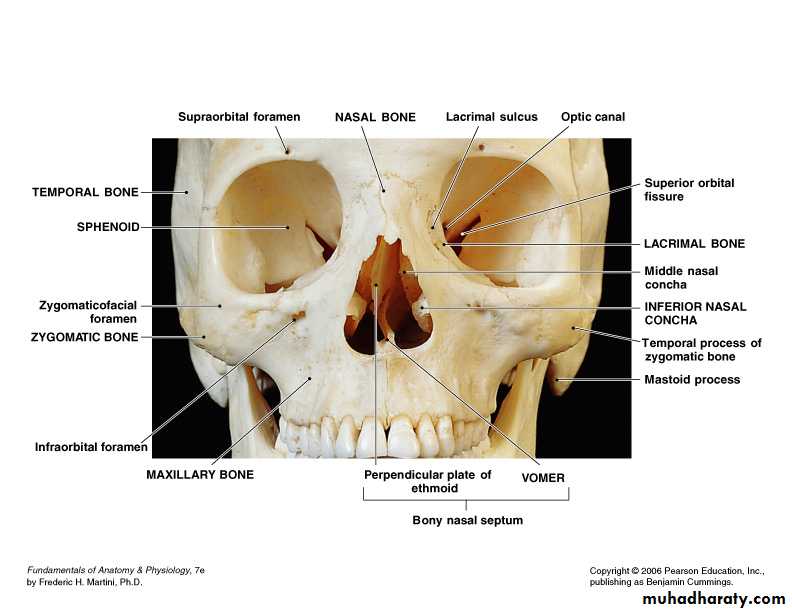
• Anatomy
• The face is composed of 14 bones:• Mandible (1)
• Vomer (1)
• Maxilla (2)
• Zygoma (2)
• Nasal (2)
• Lacrimal (2)
• Palatines (2)
• Inferior Nasal Conchae (2)
• The Small Bones of the Face
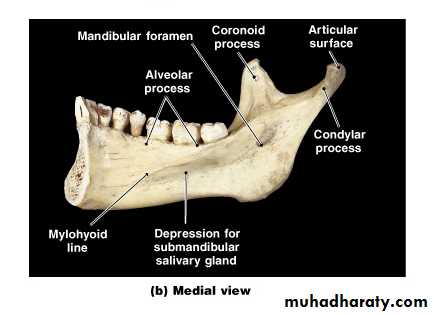
Mandibular bone
Free bone, forming the lower border of the faceTubular long bone bend into blunt V shaped or U shaped bone
Prominent , strongest, and heaviest bone of facial skeleton
It is a membraneous bone
Articulates with the temporal bone
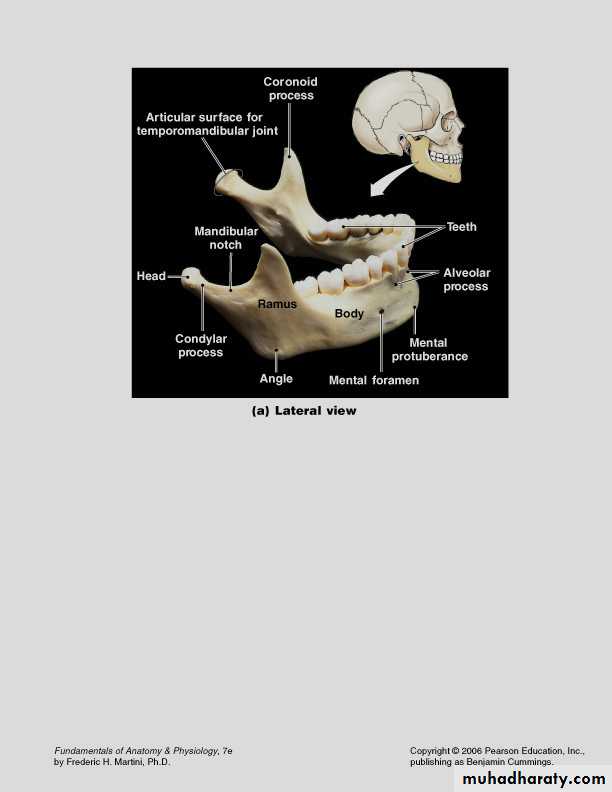
• The Mandible
Maxillofacial traumaEtiology of fractures:
• Fall From Hight (F.F.H.):
• Road Traffic Accident (R.T.A.)• Bullet Injuries (B.I.):
• Fighting
• sports injuries
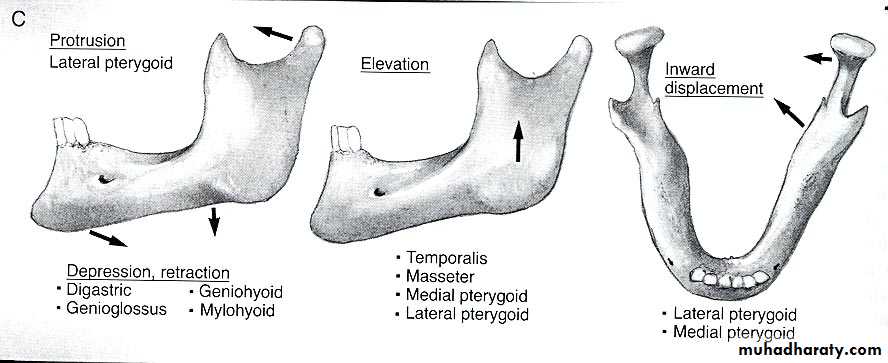
Mandibular Forces
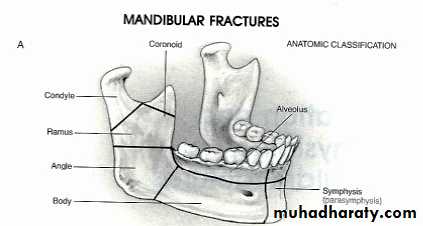
• Areas of weakness of the mandible
The junction of the alveolar bone and basal bone.Symphysis region.
Parasymphysis lateral to the mental prominence.
The angle between the body and the ramus.
Impacted lower 3rd molars.
Excessive long root of the canine.
Neck of the mandibular condyle.
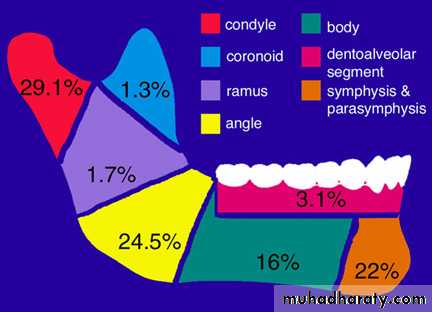
Incidence of fracture mandible
Classification of mandibular fracture
1- General classification:
A- simple (closed).There is no tear in the soft tissues. Like fracture of the coronoid, ramus and edentulous body of the mandible.
B- green stick fracture: Is a variant of simple fracture seen in children in which only one cortical plate is fractured , the other being bent. This is due to elasticity of bone .
C-compound fracture (open fracture):When there is break in the soft tissues. Tooth bearing portion of the mandible nearly always compound into the mouth through the periodontal ligament, and also can compound over the skin.
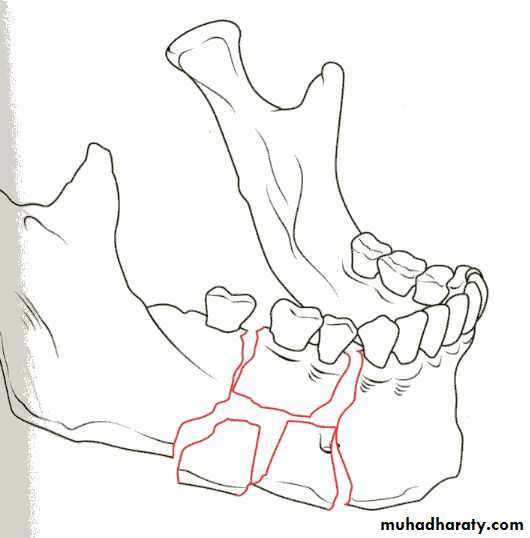
D- comminuted fracture :In which the bone is splintered or crushed into multiple pieces .
E- complicated or complex: When there is soft tissue entrapment at the fracture site like muscle or salivary gland tissues or when there is injury to vital structure like the facial nerve , inferior alveolar nerve.
F- impacted fracture.
G- pathological fracture: Due to preexisting pathological process such as (OKC or osteomyelities, neoplasm and generalized skeletal disease.
2- Classification according to the sites of fractures
Condyle fractureIntracapsular fracture
Extracapsular fracture
High condyle neck fracture
Low condylar fracture
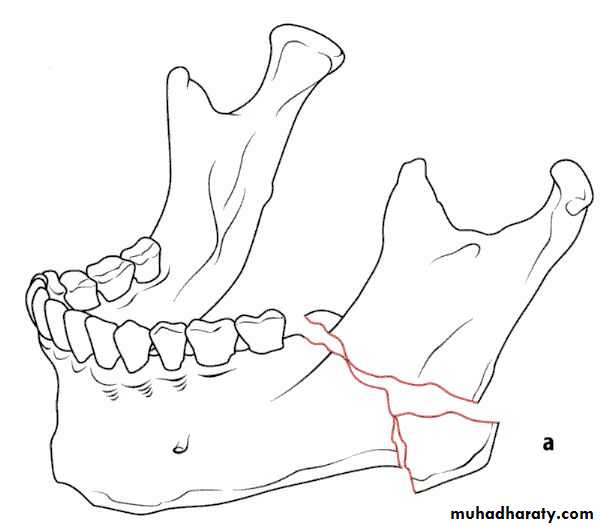
Angle/ ramus fracture (body fracture)
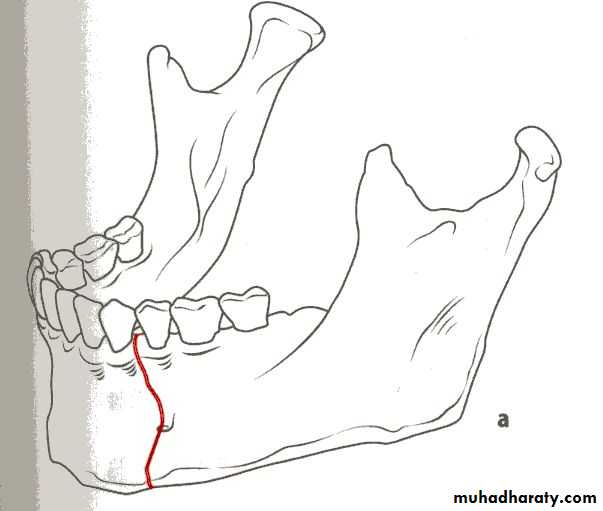
Canine region (parasymphesial fracture)
Midline fracture (symphesis fracture), it usually occur together with bilateral condylar fracture (guardsman fracture)Coronoid fracture (rare)
3- Classification according to the location of the fracture line to the existing teeth in the dental arch.
Class 1: in which teeth are present on both sides of the fractured line.
Class 2: in which teeth are present in one side of the fracture line.
Class 3: in which tooth fragments are edentulous.
Class 1
Class 2
Class 3
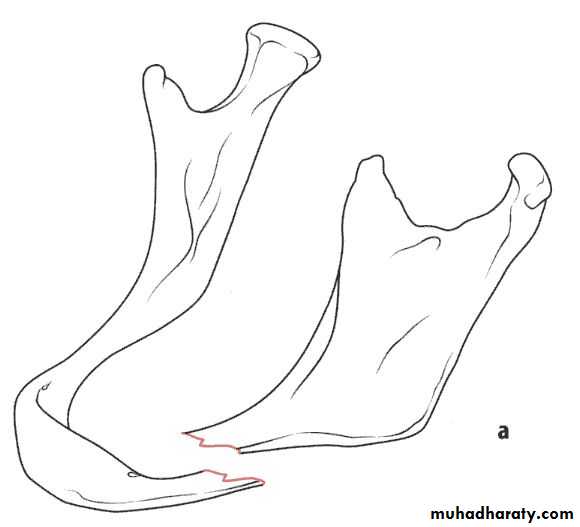
Edentulous Body Fracture
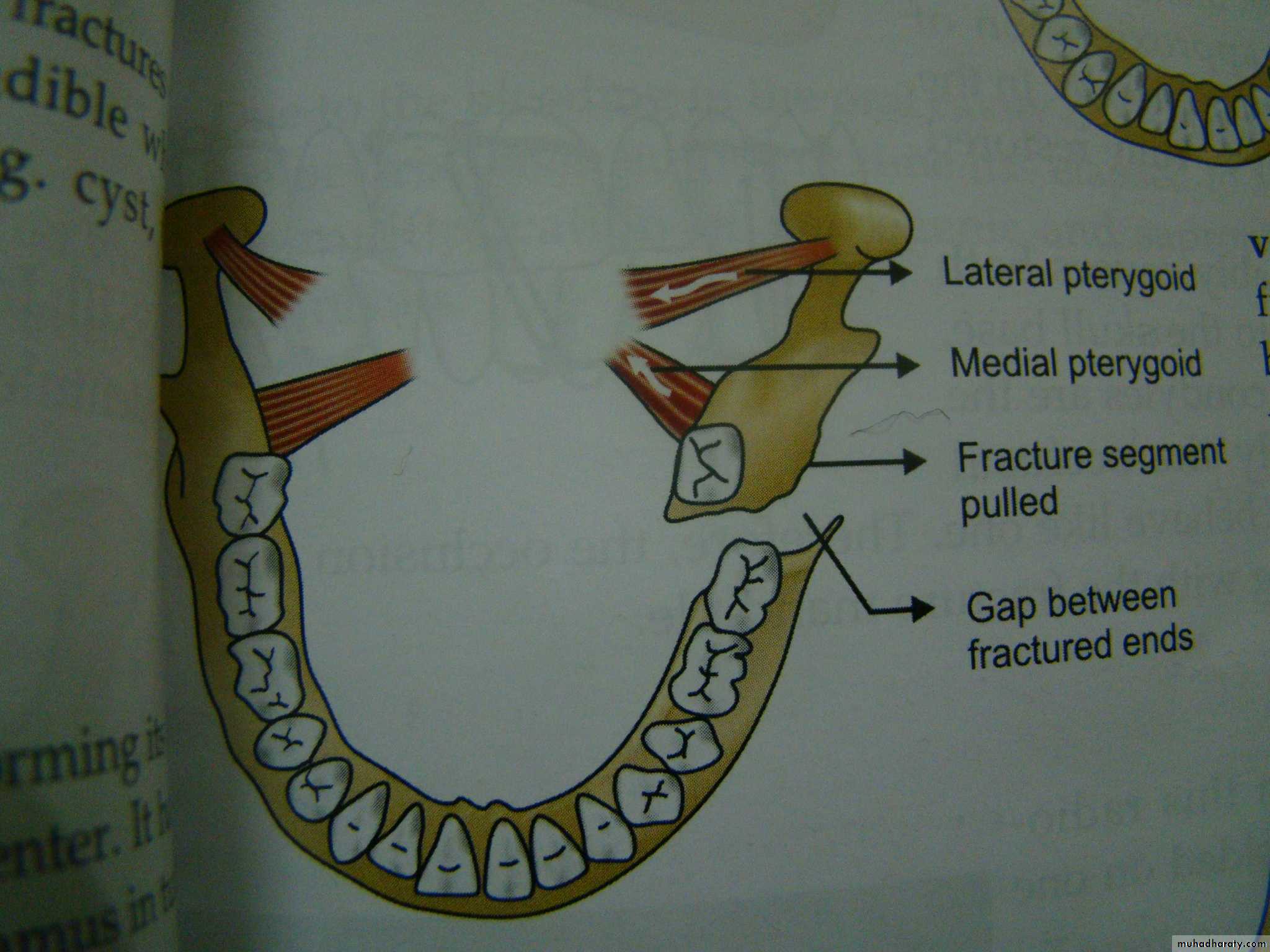
Class 34-classification according to the Direction of the fracture and favourability for the treatment
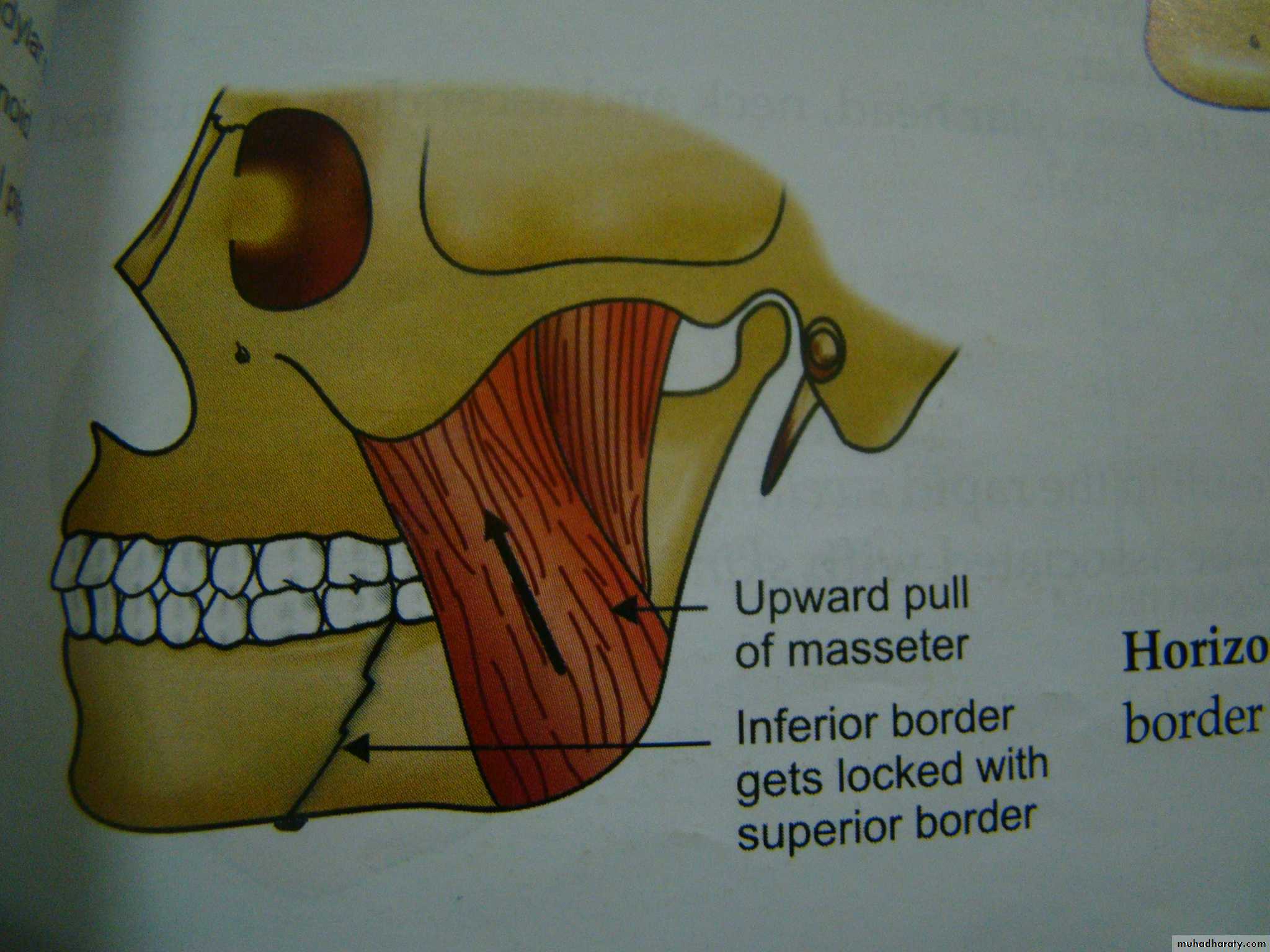
1- Horizontally favorable fracture.
2- Horizontally unfavorable fracture.
3- Vertically favorable fracture.
4- Vertically unfavorable fracture . This classification is aimed toward the angle and body fractures.
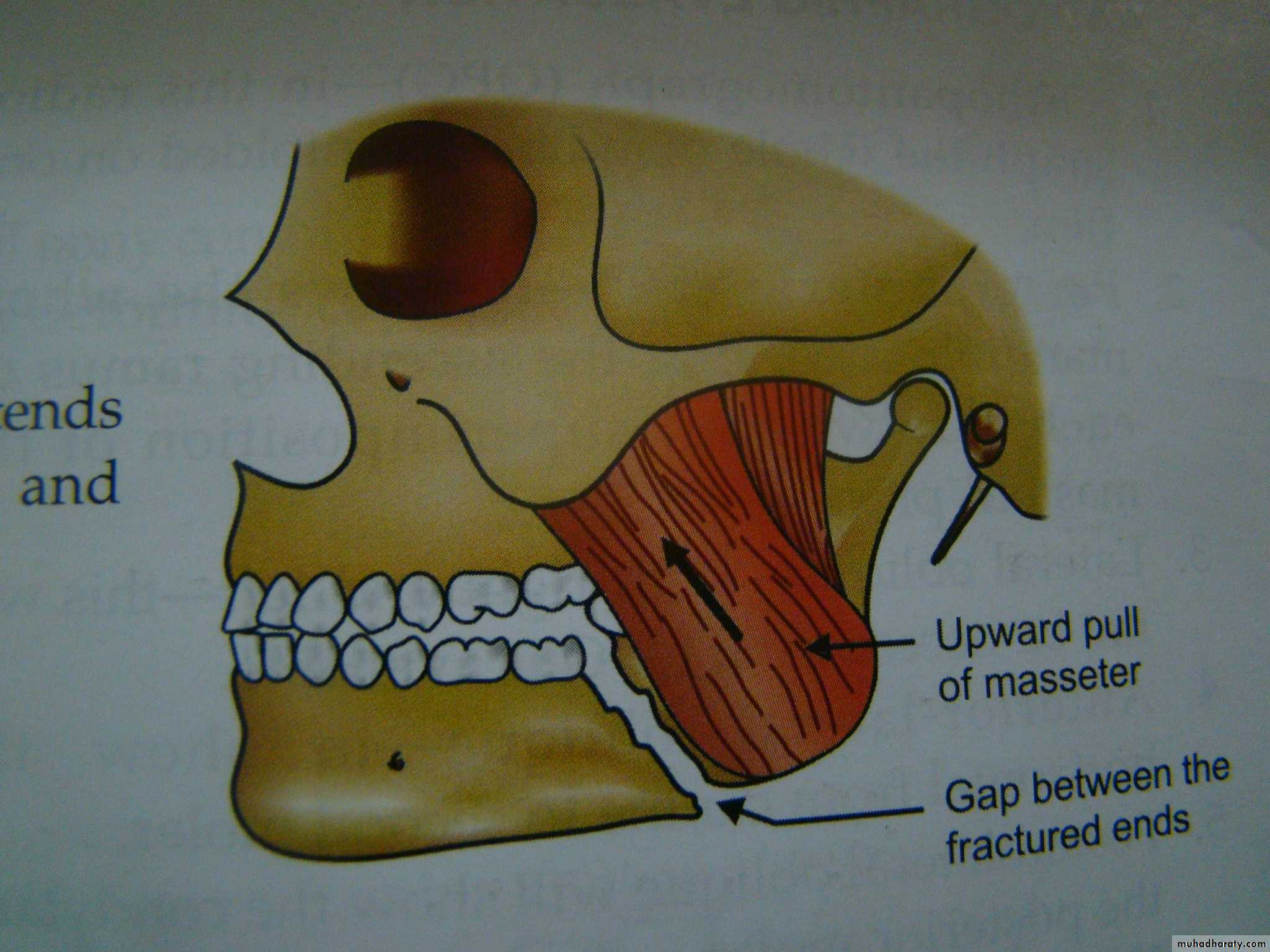
When the muscle pull resist fracture displacement , it is favorable(undisplaced), but, when the muscle pull distract the fragments away from each other resulting in displacement , it is unfavorable.
• Horizontally unfavorable fracture extends from the upper border downwards and backwards.
• Horizontally favorable fracture extend from upper border downwards and forwards.
•
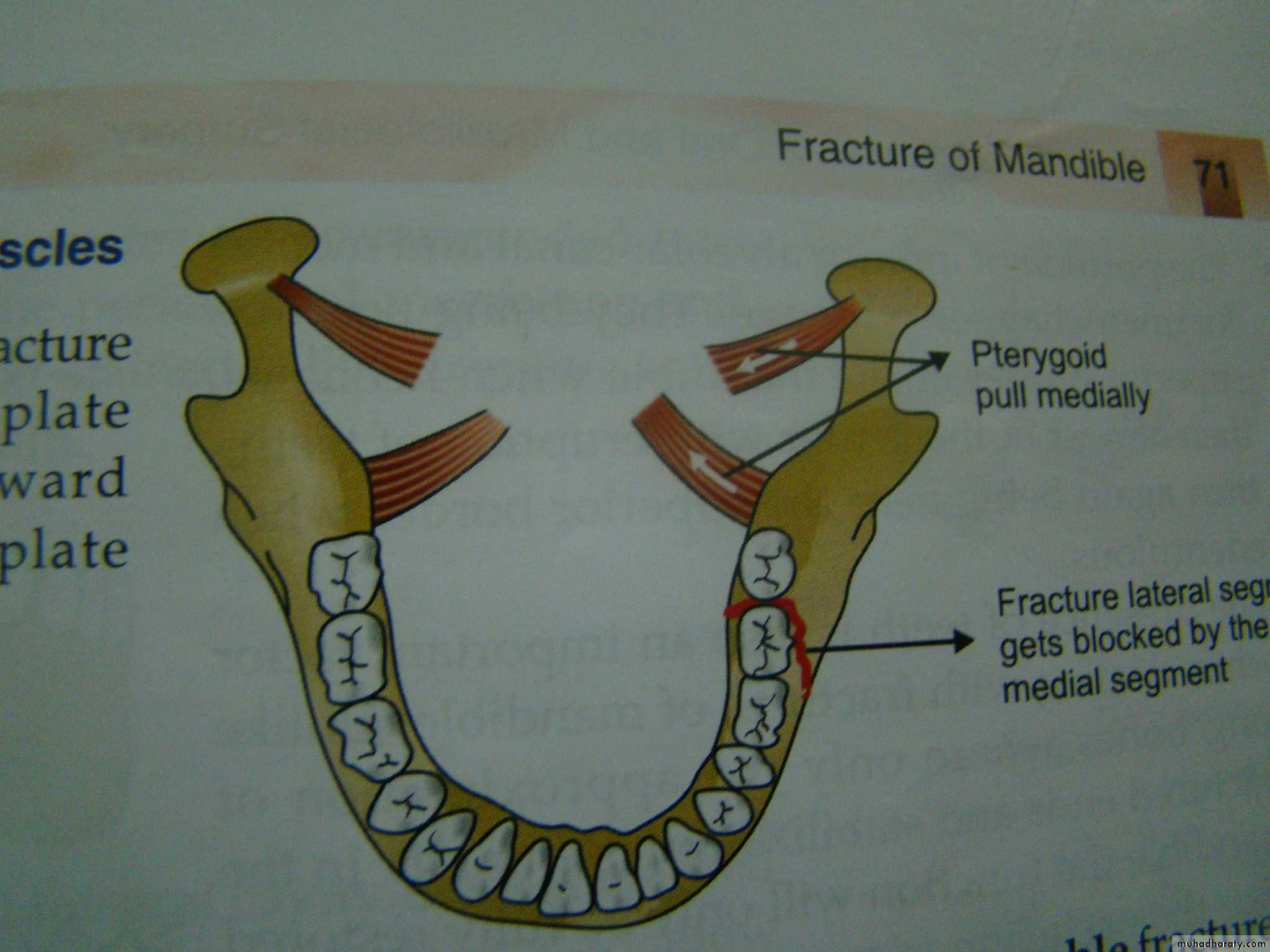
• A vertically favorable fracture runs from the buccal plate anteriorly and backward through the lingual plate posteriorly.
• Vertically unfavourable fracture runs from the lingual plate anteriorly backward through the buccal plate posteriorly.
•
Clinical assessment and diagnosis
History of trauma(traumatized patients with possible head injury) and facial injuries
Clinical Examination
▶ ExtroralInspection (assessment of asymmetery, swelling, ecchymosis, laceration and cut wounds)
Palpation for eliction of tenderness, pain, step deformity and malfunction
▶ Intra- and paraoral
bleeding, heamatoma, gingival tear, gagging of occlussion and step deformity and sensory and motor deficiencyRadiographs
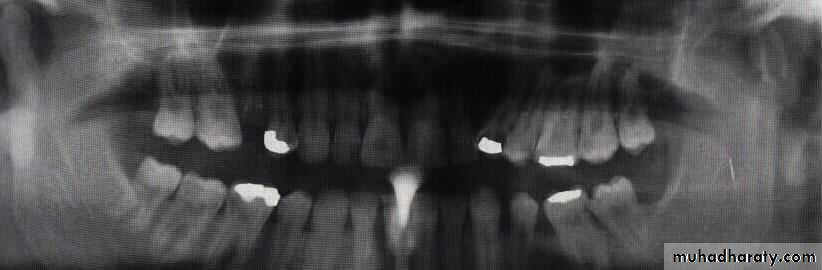
Radiographic evaluation:
Plain radiographOPG
Lateral oblique
PA mandible
AP mandible (reverse Townes)
Lower occlusal
CT scan
3-D CT imaging
MRI




Signs and symptoms of mandibular fracture
Midline fracturePain and tenderness
Swelling and odemea
Development of step deformity
Mental anesthesia (parasthesia)
Heamatoma in the floor of mouth and buccal mucosa
bleeding in the lingual submucosa is one of the most valuable signs of bony injury in the body of the mandible (Colman's sign ).
Soft tissue injury of the chin and lower lip
If associated with condylar fractures
Absence of condyle movement on the controlateral sideDeviation of mandible
Anterior open bite
Gagging of occlussion
Limitation of mouth opening


Management of mandibular fractures
As soon as a patient of facial injuries is brought to the hospital he\she should be examined for :A-airway .
B- breathing.
C- circulation.
D- neurological deficit or disability.
E- exposure and examination of the whole body.
Air-way control
Patency of the airway is ensured by the following measures:1- Position of the patient : Conscious patient will maintain the most comfortable position, but, the semiconscious or unconscious should be placed on a prone or semi prone position.
2- Airway cleaned from foreign bodies , teeth fragments or bone pieces using sucker and gloved fingers.
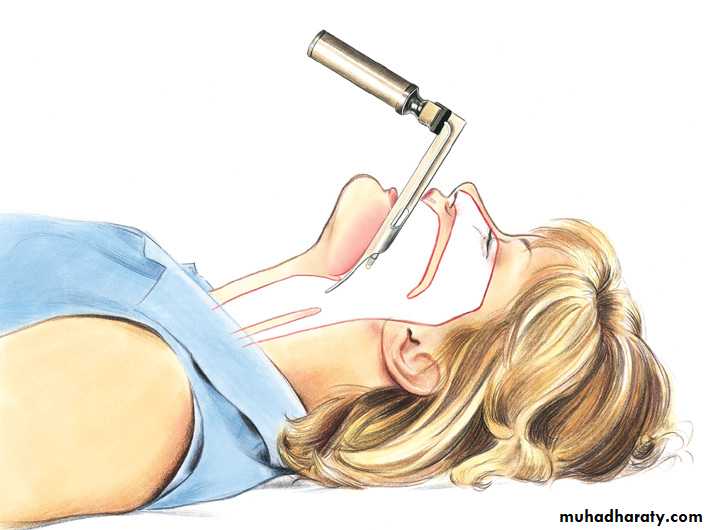
3- Glossopexy :the tongue transfixed at the junction of the ant. 2\3 and post 1\3 using heavy silk suture and attached to the patient chest.
4- Nasopharyngeal airway or oral airway.
5- Any bleeding is controlled.
6- Endotracheal intubation.
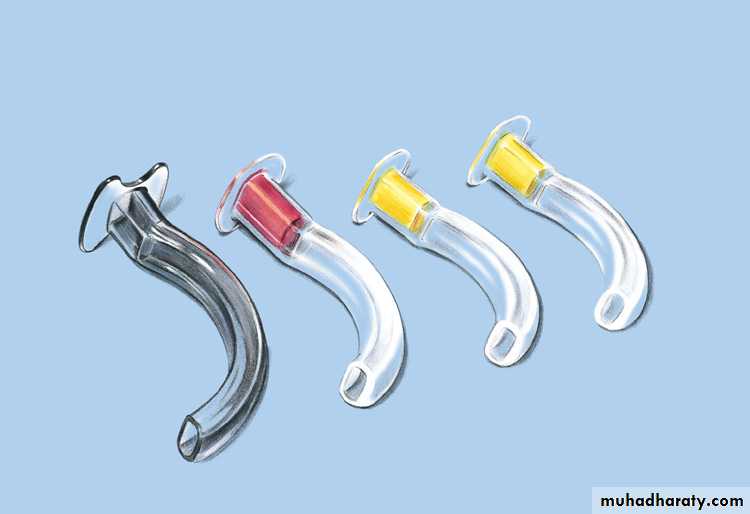
7- Tracheostomy.
8- Cricothyroidotomy.
Open the AirwayPosition
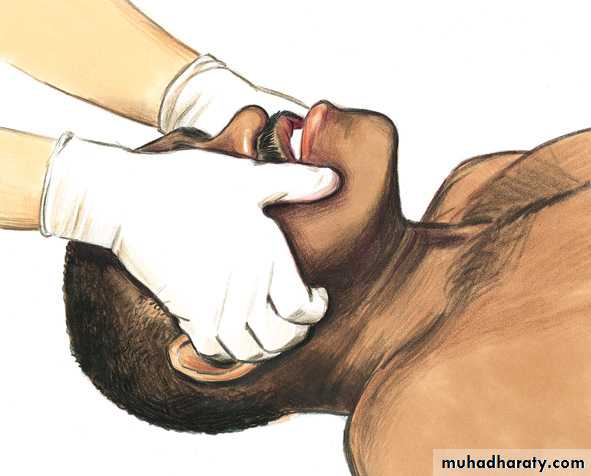
Jaw thrust
Head tilt–chin liftOpen the Airway Oropharyngeal Airway

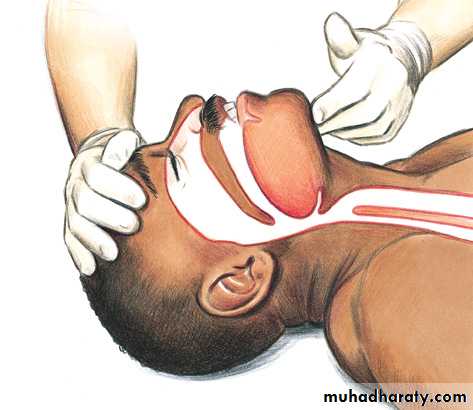
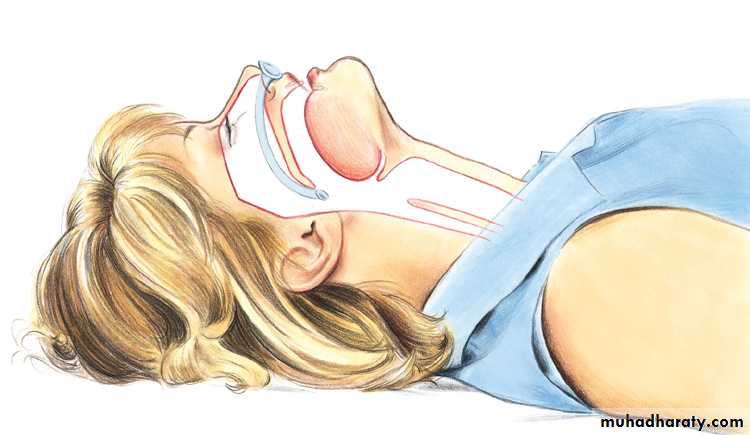
Open the AirwayNasopharyngeal Airway

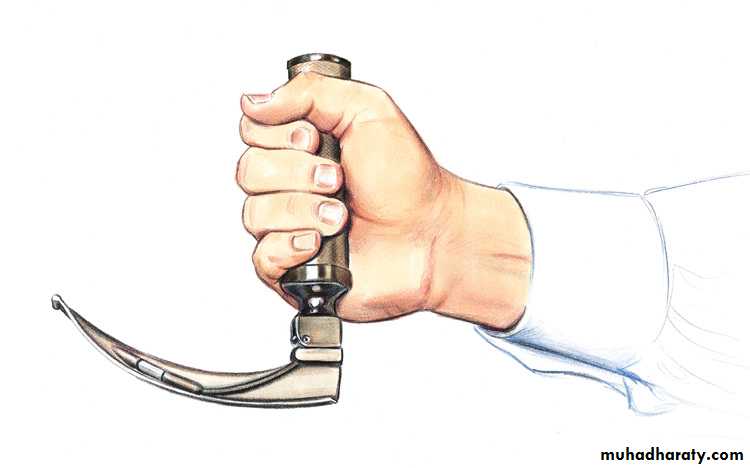
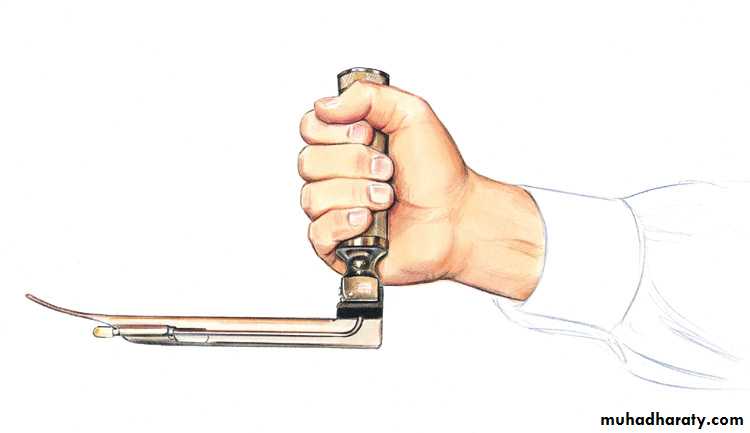
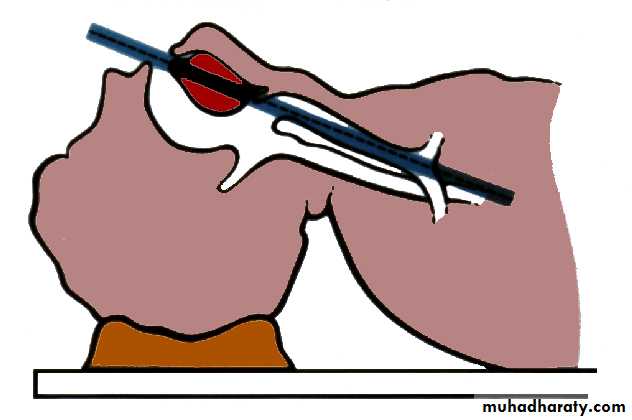
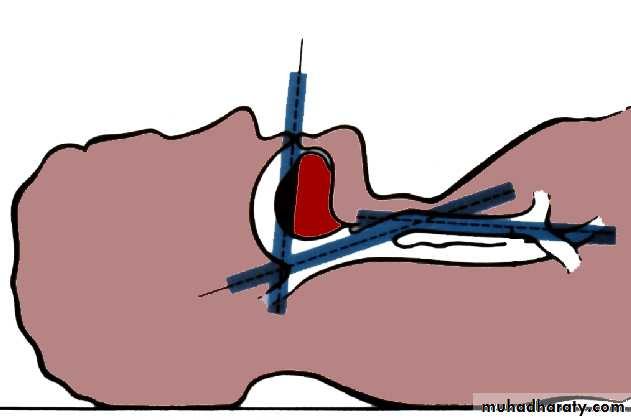
Open the AirwayEndotracheal Intubation “ Laryngoscopes ”

Open the AirwayEndotracheal Intubation “Aligning Axes of the Airway”
Breathing
The main cardio pulmonary mechanism may be affected, if there is another trauma involving the root of the neck or chest , or in case of associated blunt trauma causing rib fracture , then chest tube must be inserted in pneumo hemothorax.Circulation
1- Arrest bleeding: most often temporary reduction of the fractured bone is enough to stop bleeding from the face.2- Blood loss assessment.
3- Blood loss replacement, start with ringers lactate and if necessary plasma expander like heamacil and FFP, until crossed matched blood is available.
Deficit
The neurological evaluation of the patient should then be carefully done, and any deficit in the patients neurological condition carefully recorded( Glasgow comma scale). This will form the base from which the patients condition can be evaluated. If he / she is improving or deteriorating can be assessed with regular neurological evaluation.
Narcotic analgesic should be avoided.

Exposure for examination
The whole body should be examined very carefully as soon as not to miss out on any other important injury ( intra oral or extra oral). If other body parts are injured the concerned specialist should be called for. Then in consultation final treatment planning should be done.Principles of treatmentsimilar to elsewhere fractures in the body
Reduction of fragments in good positionImmobilization until bony union occurs (3-6 weeks)
These are achieved by:Close reduction and immobilization
Open reduction and rigid fixation
Other objective of mandible fracture treatment:
Control of bleedingControl of infection
Soft tissue repair
DebridmentIrrigation with saline and antibiotics
Closure in layers
Dressing
Reduction and fixation of the jaw
▶ Close reduction and IMF (traditional method by means of manipulation)▶ Open reduction and semi-rigid fixation (using inter-osseous wirings)
▶ Open reduction and rigid fixation (using bone palates, osteosynthesis)
Objective:
Restoration of functional alignment of the bone fragments in anatomically precise position utilizing the present teeth for guidance
Definitive treatment
Goals of the treatments• Rapid bone healing
• Return of normal appearance
• Masticatory function
• Restoration of speech
• Acceptable esthetic
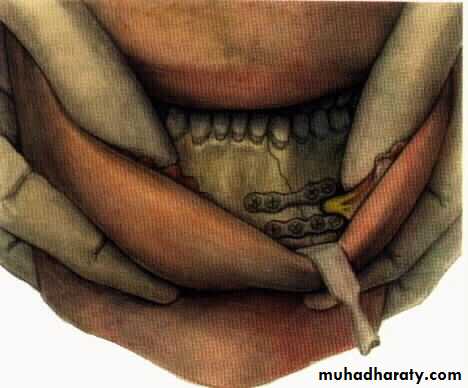
Reduction
Closed reduction involves the blind manipulation of the fracture without directly exposing the fracture site and using the teeth and occlusion as guides to proper positioning.
Open reduction : The fracture site is surgically exposed to allow direct inspection of fracture reduction and alignment.
Open reduction of the fracture can be achieved in two ways :
1- inter maxillary fixation .
2- free hand manipulation
Fixation
Once the fracture is properly aligned , fixation is used to stabilize the position of the fracture site to allow healing.1- External fixation: It does not permit direct control of bone fragments, which are stabilized in a blind manner, frequently resulting in imprecise anatomic alignment and prolonged secondary bone healing via large callous formation .
2- Internal fixation : In which the bone is reached either through intra oral or extra oral approach.
Principle of mandibular fracture
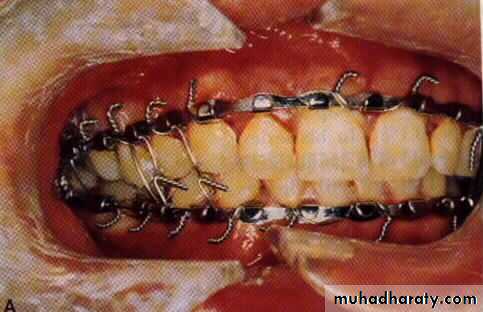
• Closed reduction with indirect skletal fixation : Dependent on splinting of the mandible to maxilla to restore centric occlusion (maximal intercuspation)• 1. IMF ( Prefabricated arch bar )
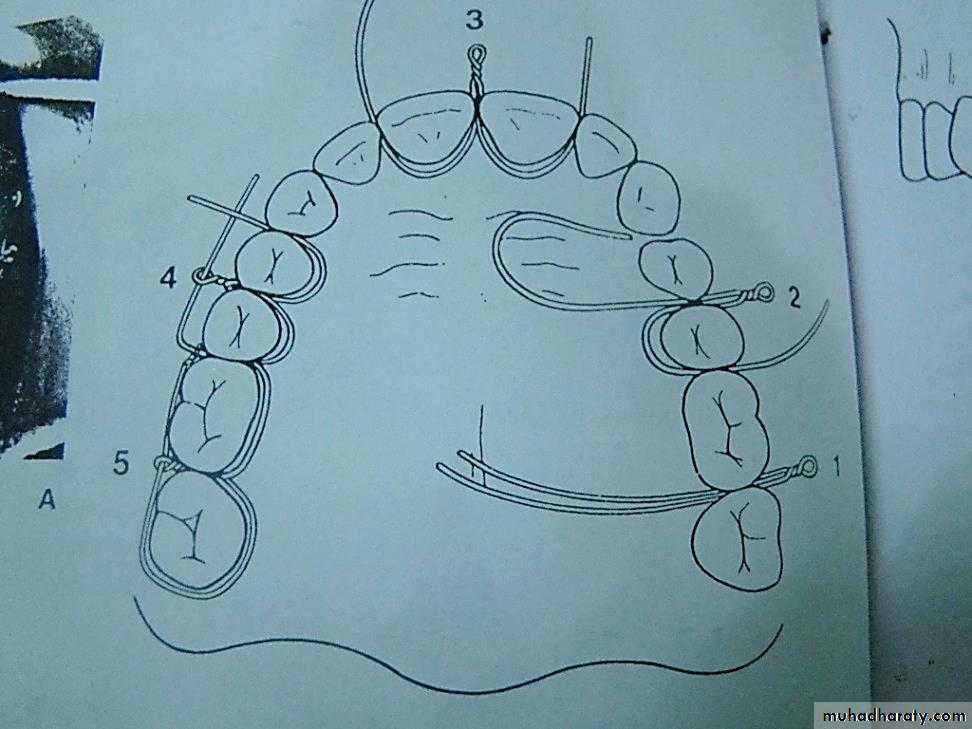
• 2. Ivy loop or interdental eyelet wiring
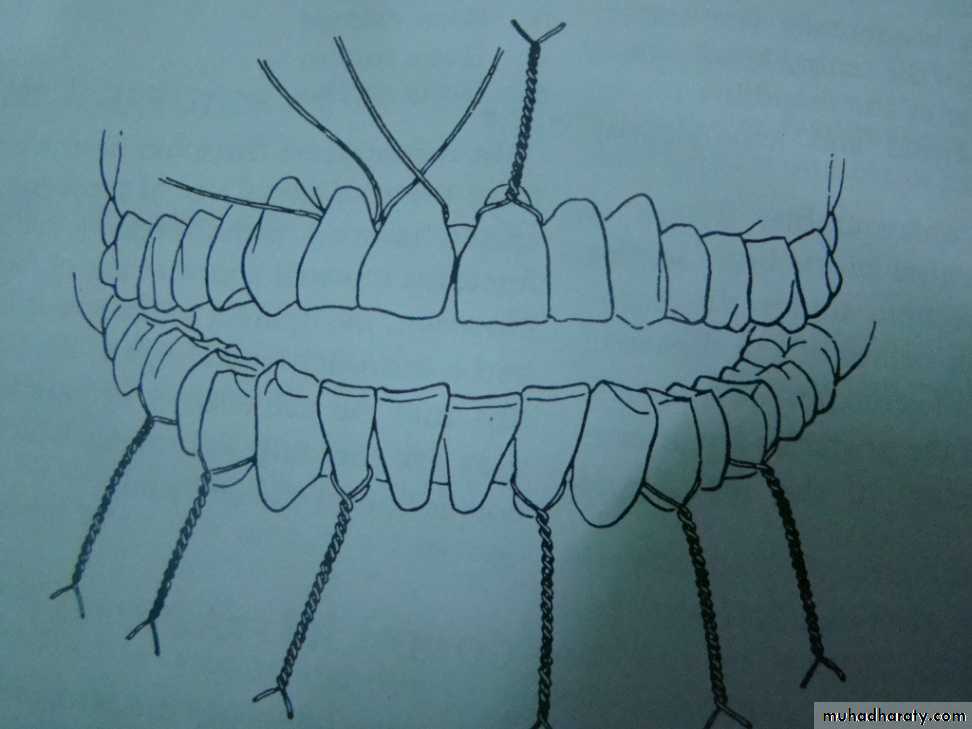
• 3. Continuous multiple loop wiring
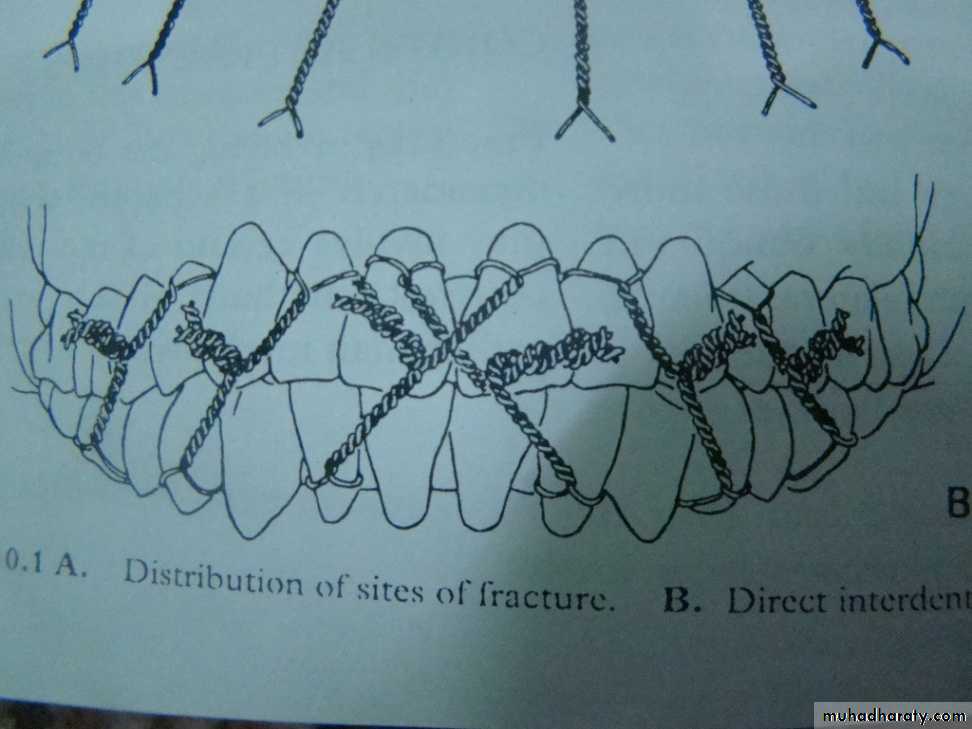
• 4. Direct dental wiring .
• 5- risdon wiring.
• 6. Circummandibular wiring (edentulous) p’t
• 7. occlusal splint (children)
Close reduction
Arch bars
Jelenko
Erich pattern
German silver notched
Cap splints
▶ IMF prior to rigid fixation
▶ For the purpose of close reduction
Close reduction


Dental wiring:
Direct wiring
Eyelet wiring
Local anesthesia or sedation
Minimal displacement
IMF for 6 weeks
Treatment can be performed under GA or LA and when surgery is contraindicated
• A 15 cm length of pre stretched (10%) 0.35 mm diameter soft stainless steel wire is passed around a tooth emerging through the inter dental spaces.
• With the wire placed around the neck of the tooth the two ends are tightened by twisting together . An adequate number of teeth are wired in a similar fashion in both jaws.
Direct dental wiring
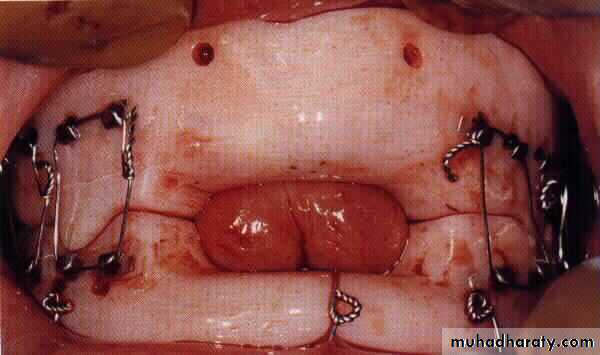
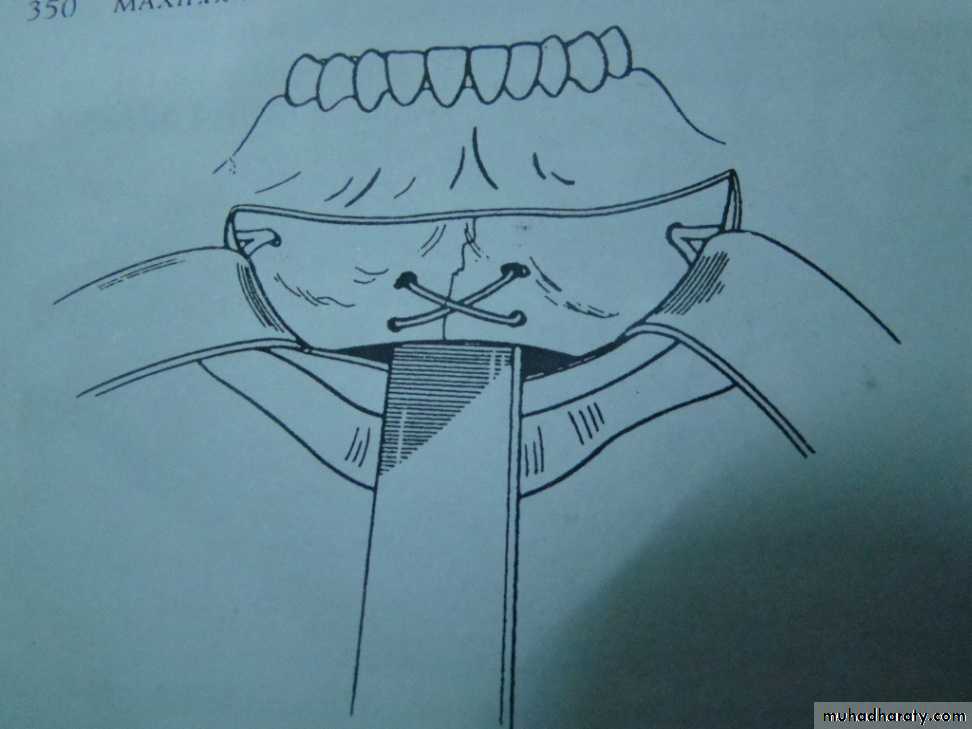
Circummandibular wiring ( splinting)
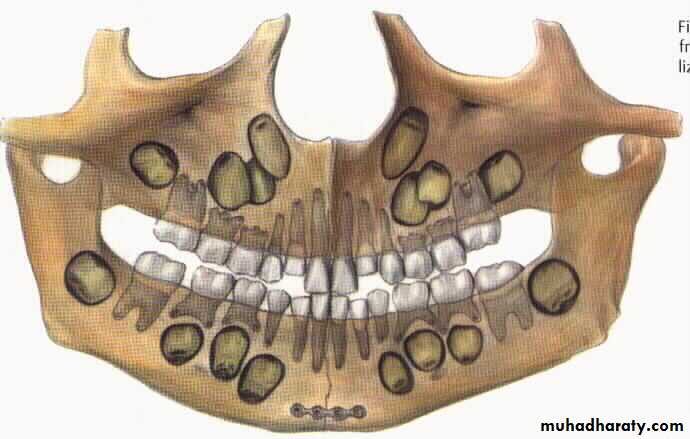
It is indicated in the young children and for edentulous patient.In children below 12 years age cap splints are made and circumferential wiring done so that injury to the tooth buds can be avoided.
Similarly in edentulous patient , who also have a compromised blood supply, and no teeth to give inter maxillary fixation, this technique is very helpful.
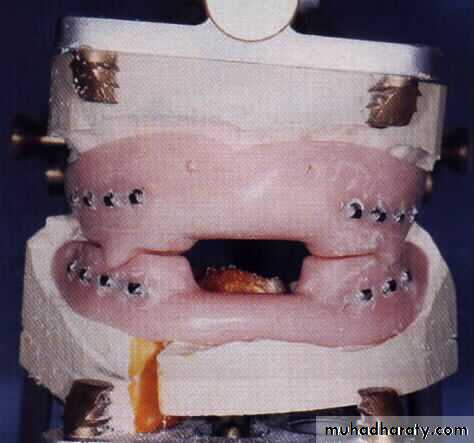
Gunning’s splint
Old modalityEdentulous patient
Rigid fixation is not possible
To establish the occlusion


Open reduction and fixation
Intraoral approachExtraoral approach
▶ Submandibular approach

Indications for Open Reduction
• Displaced unfavorable fractures through the angle of the mandible.• Atrophic edentulous mandibles, minimal cancellous bone, and poor osteogenesis and healing potential.
• Complex facial fractures requiring a stable mandibular base. These fractures require the mandibular segments to be reconstructed first with open reduction and fixation.
• Condylar fractures. While condylar fractures are generally treated with closed reduction, a specific group of individuals benefits from surgical intervention. Bilateral or unilateral condylar fractures when splinting is not recommended because of concomitant medical conditions or in an edentulous patient when splints are unavailable or impossible because of alveolar ridge atrophy.
• Open reduction
• Intraosseous wiring + IMF (3 to 8 weeks)• Rigid internal fixation (plating) these method use bone plates, bone screws or both to fix the fracture.
• Lag screw.
• Inter medullary pinning.
• External pin fixation in patients with extensive comminution or infected fracture
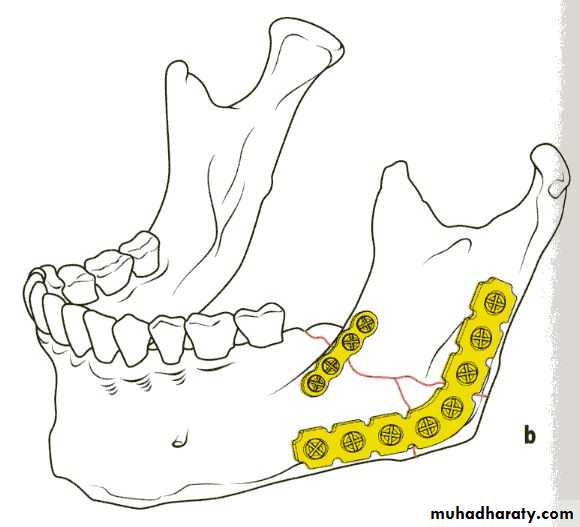
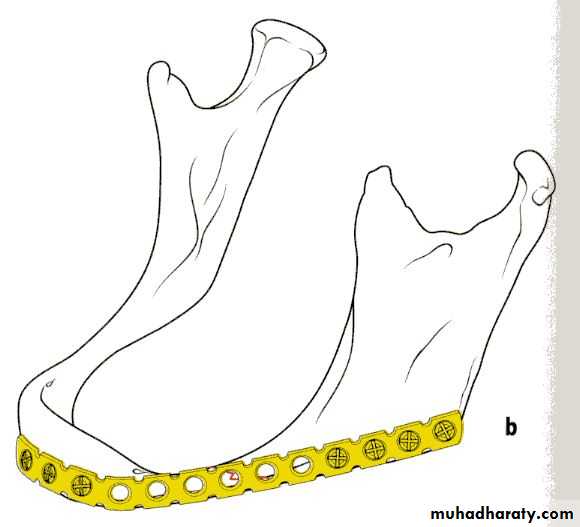
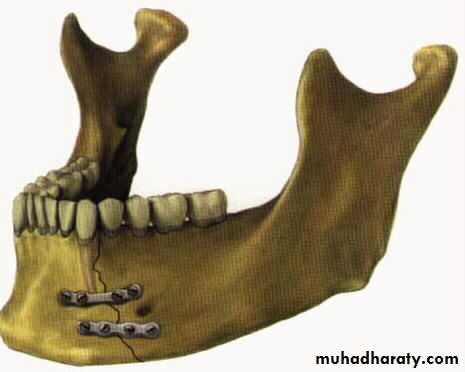
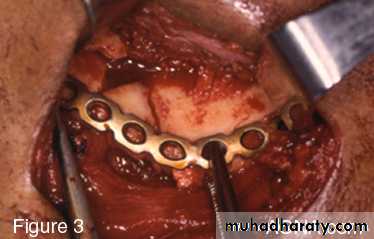
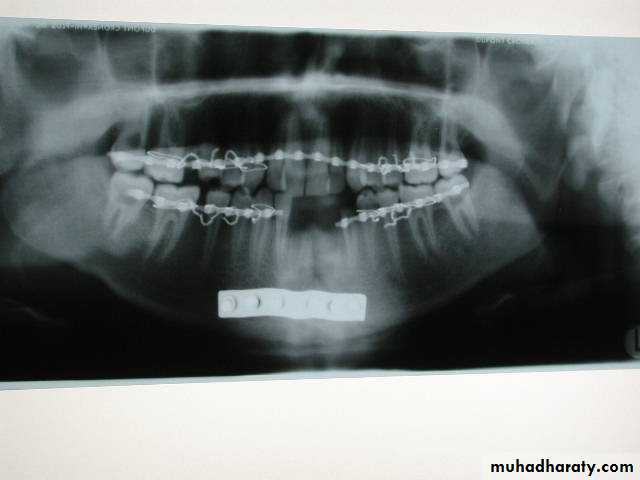
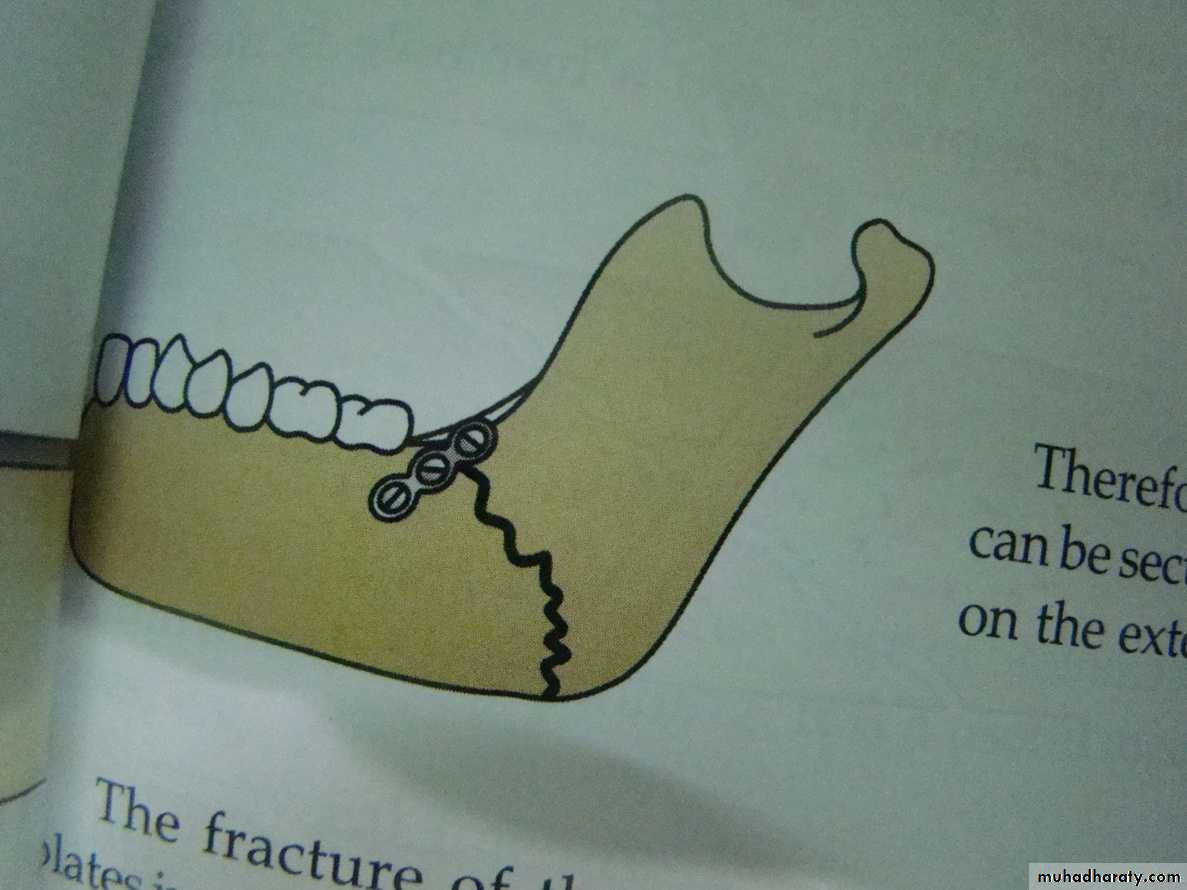
Plating
If teeth are present IMF is done ; then incision is made and bone is reached either extra orally or intra orally.The fractured ends are approximated and screw holes are made such that at least 2 screws can be placed on either side of the fracture.



The champy,s technique of plate fixation
1- Use mono cortical screw fixation ; place a minimum of 2 screws on each side of the fracture.2- The more posterior the fracture the more higher the plate should be placed . The more anterior the fracture , the closer the plate should be placed to the lower border.
3-To avoid devitalization of bone , place plates supra periosteally in atrophic edentulous mandible and extensively comminuted fracture.
In plating posterior mandible single upper border plate is enough for fixation. While in plating anterior mandible , two plates are required to help counter the torsional forces of fracture in this location.
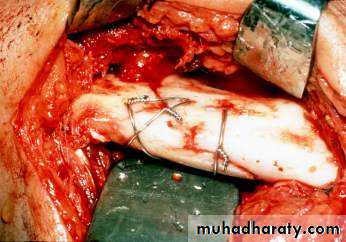
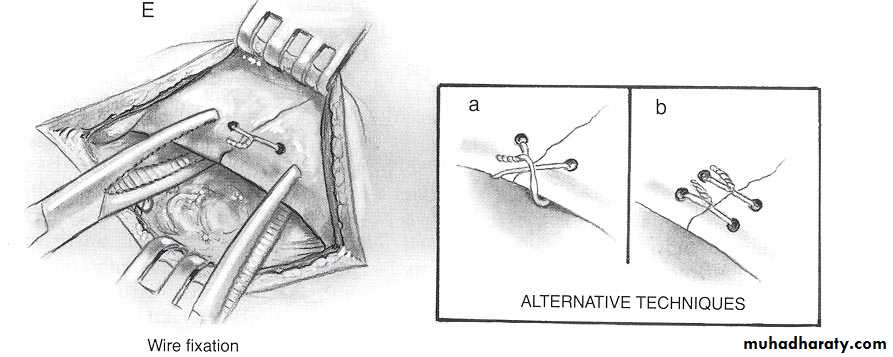
Intra osseous Wiring
If teeth are present ,IMF is done to correct occlusion . Mandible is opened , fracture ends are approximated .Bur holes are made which penetrate both cortices .wire is passed through and tightened. Once immobilization is satisfactory the incision is sutured and dressing done.Open reduction – non rigid fixation
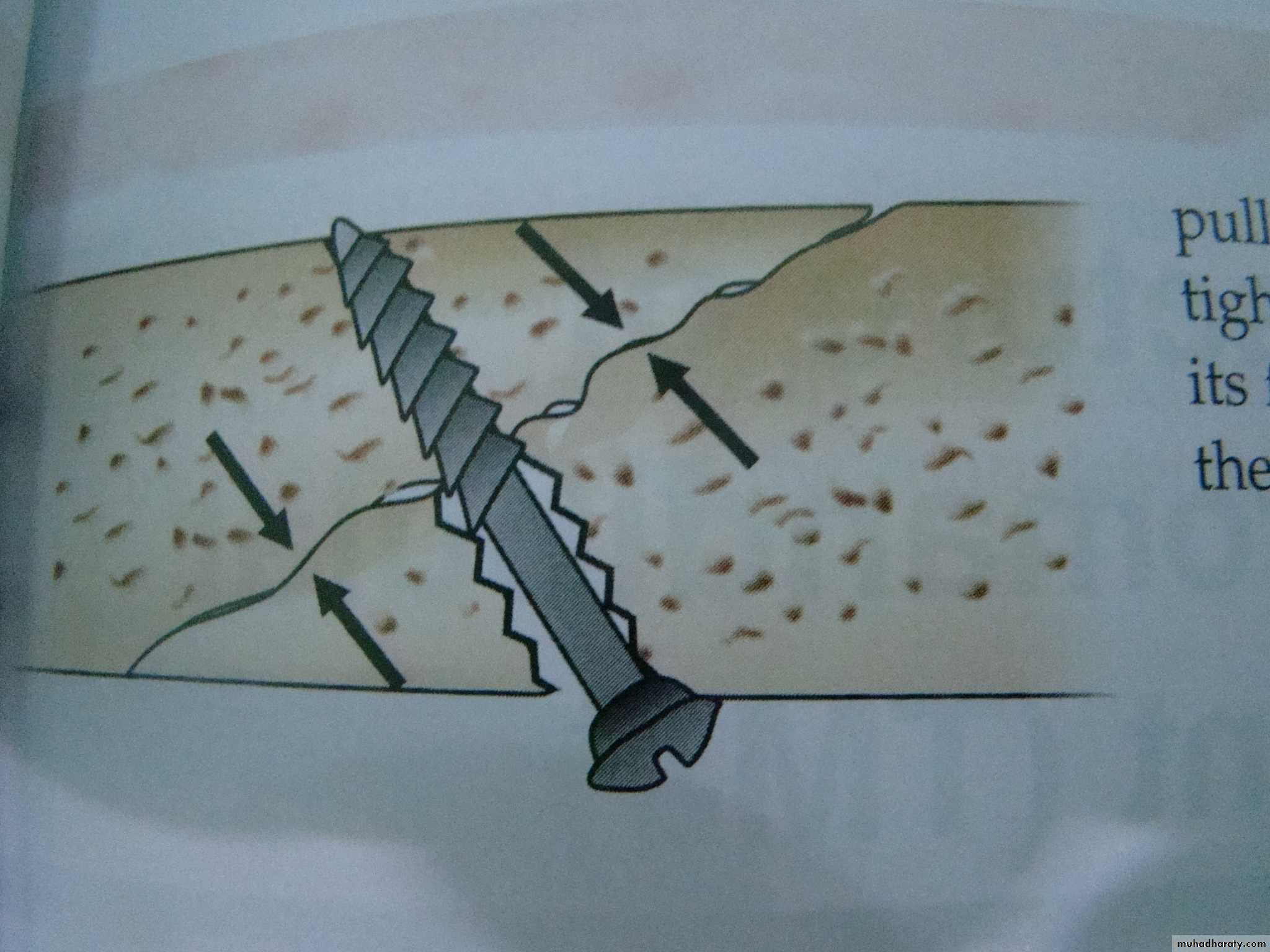
Lag screw
This is specially indicated in oblique fracture. The lag screw is special screw which has threads only in one half, the half near the head of the screw is smooth.Once the fractured ends of the mandible are approximated a bur hole is made obliquely through both the cortices.
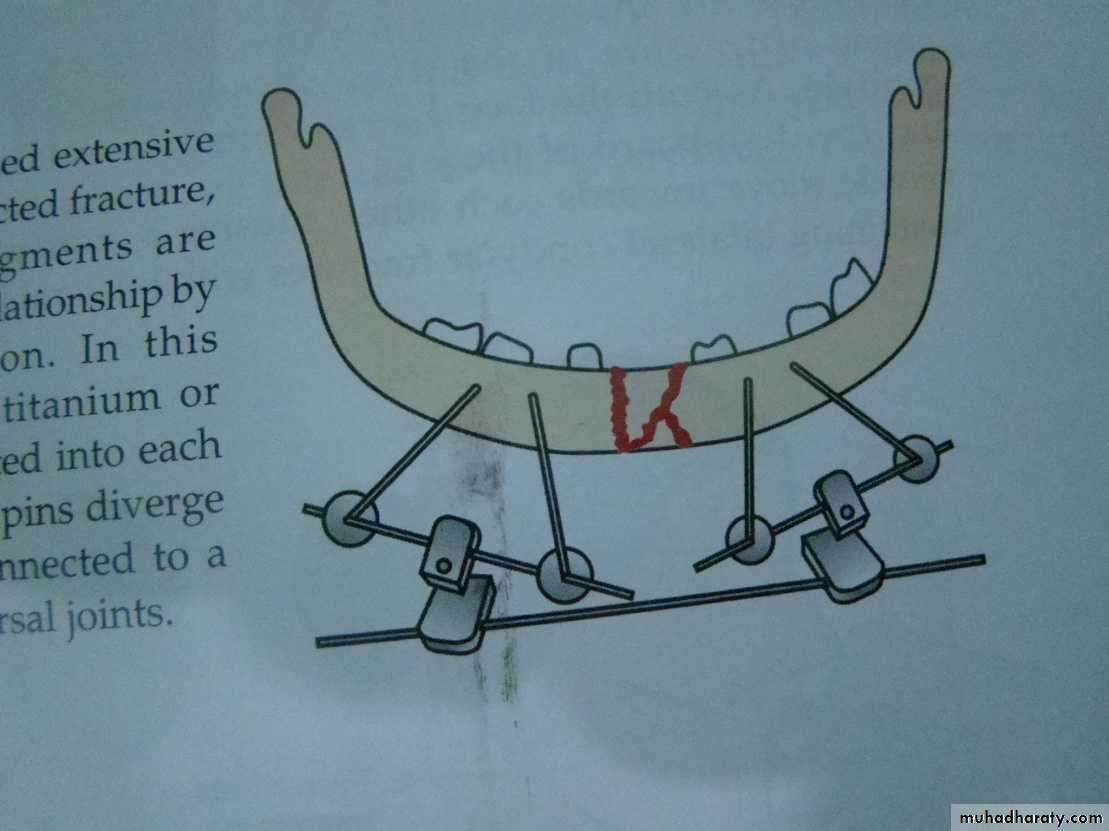
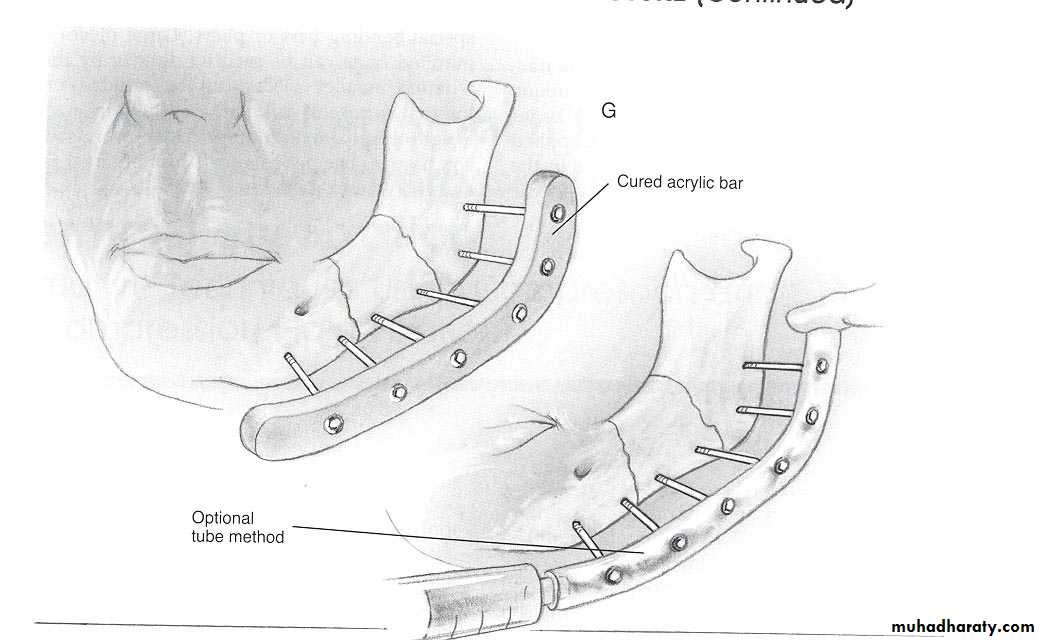
External pin fixation
In patients that have sustained extensive comminuted fracture or there is infected fracture , some times the major fragments are maintained in their proper relationship by using external pin fixation.This technique a pair of 3 mm titanium are inserted into each major bone fragment.
These pin diverge from each other but are connected to a cross bar by means of universal joint.
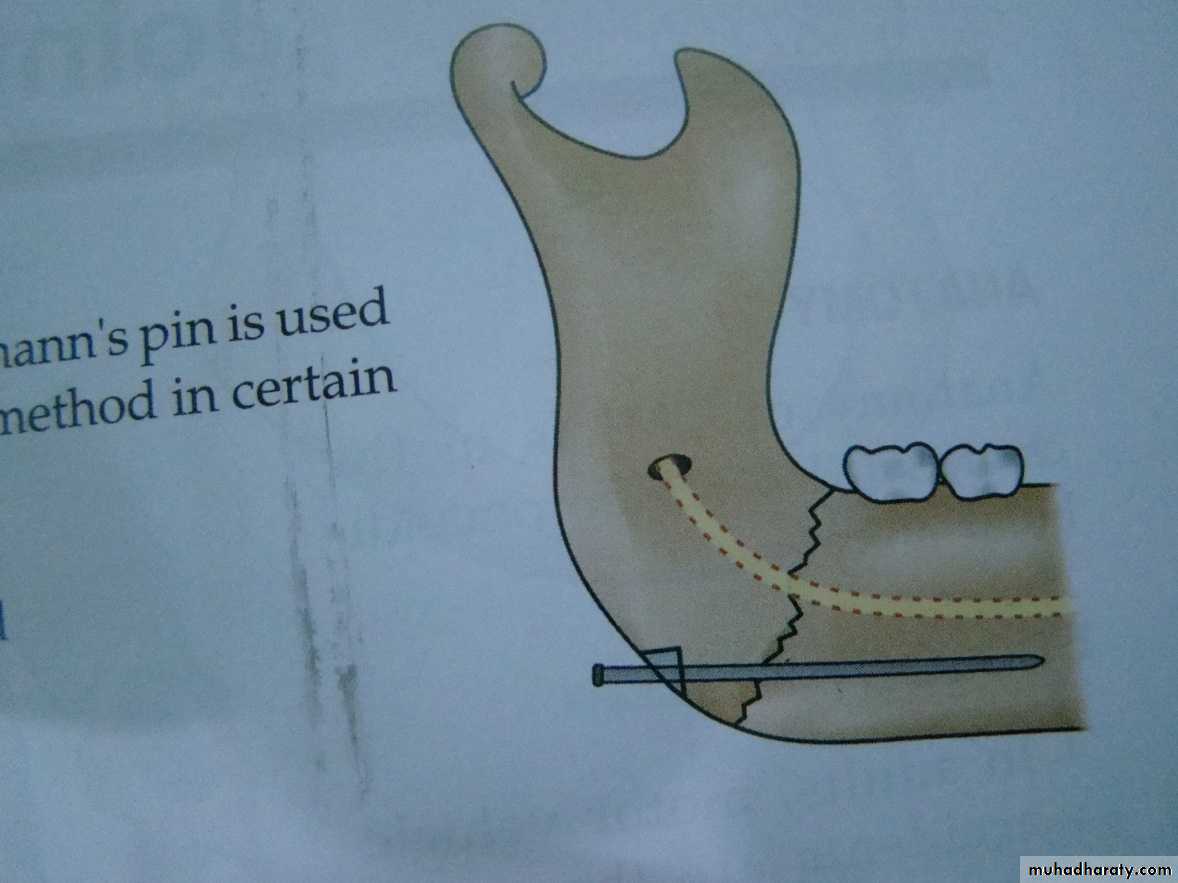
Inter medullary pinning
A 2 mm diameter Kirschner wire or Steinmanns pin is used for intra medullary pinning. It is a useful method in certain cases, e.g1-symphyseal fracture.
2- in cases where IMF is contra indicated
3- unstable fractures.
4- pathological fractures.
Management of teeth retained in fracture line
Good quality intra-oral periapical radiographInsinuation of appropriate systemic antibiotic therapy
Splinting of tooth if mobile
Endodontic therapy if pulp is exposed
Immediate extraction if fracture becomes infected
Follow up for 1 year and endodontic therapy if there is a loss of vitality
Absolute indications for removal of tooth
Longitudinal fracture
Dislocation or subluxation from socket
Presence of periapical infection
Infected fracture line
Acute pericoronitis
Relative indications
Functional tooth that would be removedAdvanced caries or periodontal diseases
Doubtful tooth which would be added to existing denture
Tooth in untreated fracture presenting more than 3 days after injury
Fracture mandible in children
Close reductionOpen reduction and fixation
Plating at the inferior border
Resorbable plates

