Urethra congenital anomaly & injuries
Dr. Ammar Fadil1
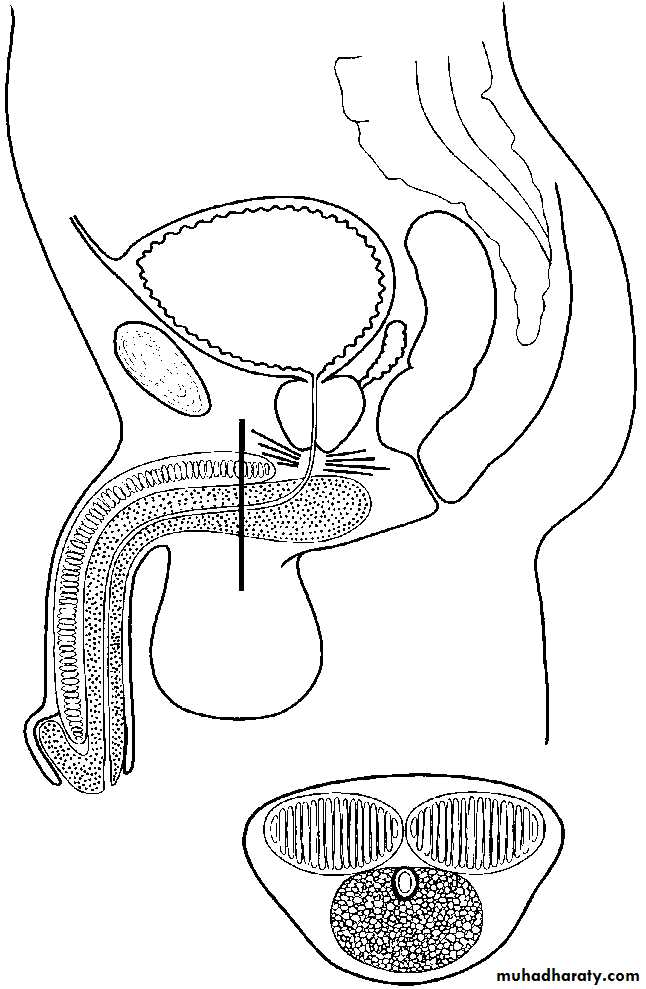
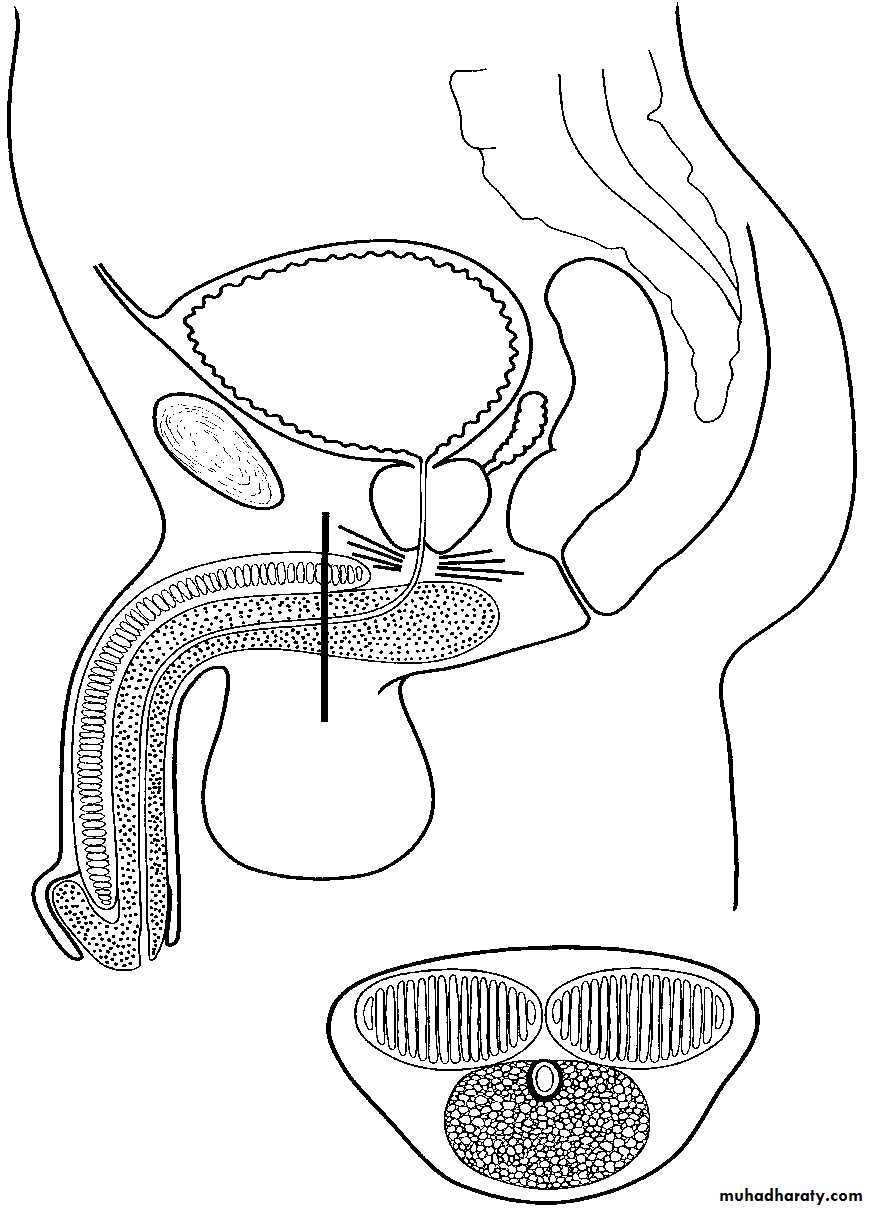
Anatomy
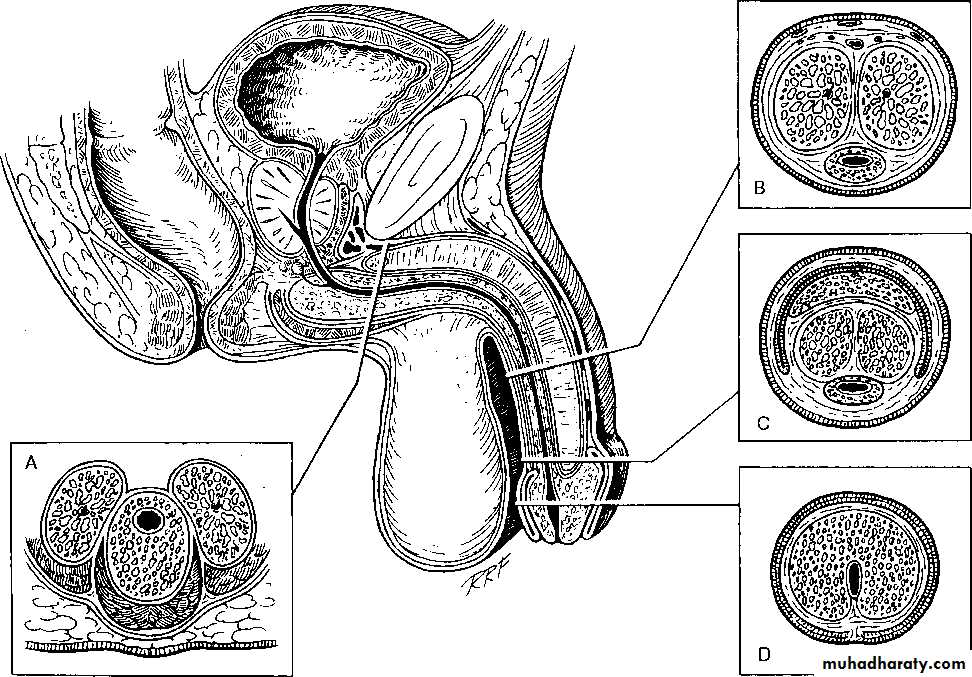
The male urethra is a tubular structure extending from the bladder neck to the external urinary meatus at the tip of the glans penis.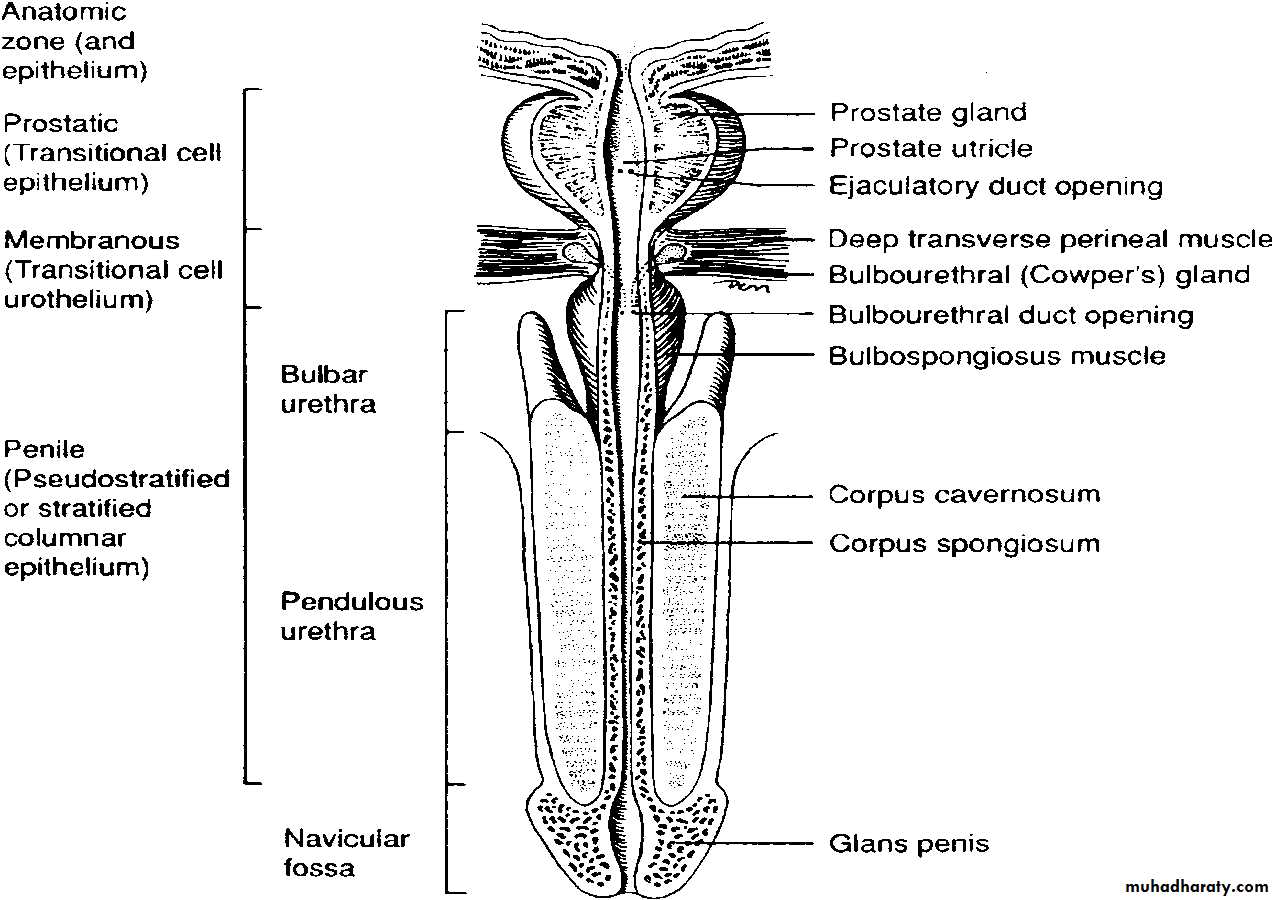
2
The male urethra divided into
• anterior urethra is made up of Bulbar & penile (pendulous) segments , which is surrounded by the corpus spongiosum• Imaging of urethra : RUG
3
The penile urethra, is surrounded by the corpus spongiosum juxtaposed to the
two corpora cavernosa.The distal part of the urethra which passes through the glans penis is named the navicular fossa. The penile urethra ends, is the external urethral meatus.
4
urethral length is between 17 and 20 cm
the prostatic urethral length is 2–3 cm,the membranous urethra 1.5–2 cm, &
the bulbous urethra 3–4 cm (the widest part)
Penile urethral length depends on the length of the penis
5
Posterior urethral valves
Posterior urethral valves are the commonest congenital obstruction of the lower urinary tract.They often have a poor, intermittent, dribbling urinary stream. Urinary infection and sepsis occur frequently
Posterior urethral valves occur only in males
Male fetus
Bilateral hydroureteronephrosis
distended full bladder
6
PUV
7
Imaging
Ultrasoundhydroureteronephrosis, a thick-walled bladder
Micturating cystourethrography MCUG provides the definitive diagnosis,
8
Treatment
achieve urine drainage with eitherurethral catheter (5 to 8Fr infant feeding tube) or
a suprapubic catheter.
Once stabilized valve ablation by endoscope
Most early infant mortality in posterior urethral valves is related to pulmonary hypoplasia
9
Hypospadias
Hypospadias is a congenital penile defect in which the urethra opens onto the ventral part (underside) of the penis, scrotum, or perineum. It is the result of incomplete development of the urethraoccurs 1 in 200–300 boys
most common congenital malformation of the urethra.
The exact etiology is unknown
10
Hypospadias is an association of three anomalies:
• • an abnormal opening of the
• urethral meatus
• • curvature (chordee) of the penis
• • the prepuce is poorly developed ‘hooded prepuce”

11
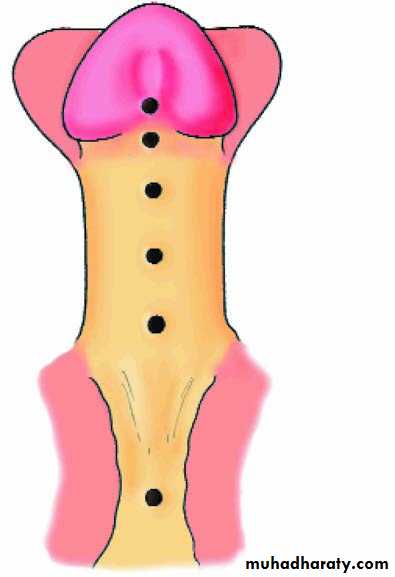
Hypospadias is classified dependent
on the position of the meatus:Distal hypospadias 70 %
• • Glanular
• • Coronal
Mid shaft 10 %
• • Penile
Proximal hypospadias 20 %
• • Penoscrotal
• This is the most severe abnormality. The scrotum is bifid and the urethra opens between its two halves. There may be undescended testes
12



13
Associated anomaly
Meatal stenosisUndescended testis
14
Treatment \Hypospadias repair
Surgery is indicated for hypospadiascorrection of curvature
Re –sitting urethral meatus (creating new urethra)
A variety of plastic surgical procedures is described to correct the chordee and to re-site the urethral opening.
We need Preputial skin and so circumcision should be avoided
Timing varies: at age 1 yr or before 2 yrs
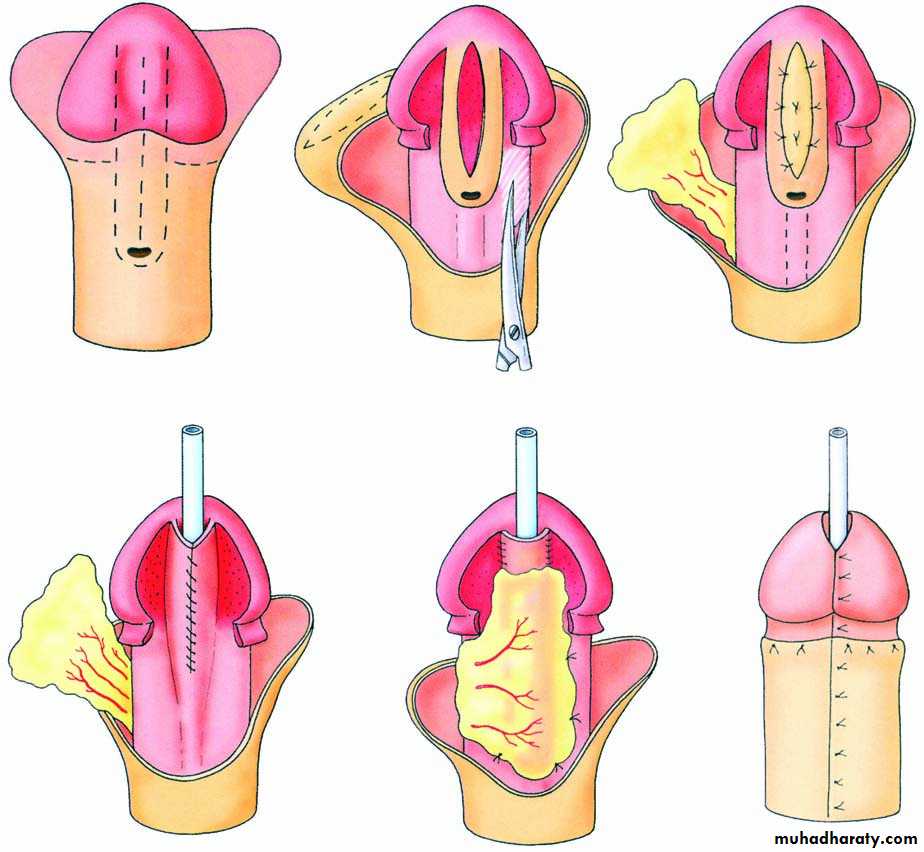
15
TIP (tabularized incised urethral plate)
16
Complications of surgery
Fistulae are the most common complications following hypospadias surgery,Meatal stenosis
Dehiscence of urethral repair
Require re operation
17Epispadias
Epispadias is very rare. In penile epispadias, the opening on the dorsum is associated with upward curvature of the penis. Epispadias usually coexists with bladder exstrophy and other severe developmental defects
18
Urethral injuries
leading often to sequelae such as strictures, impotence, infertility, & incontinence.Anterior urethral trauma
• usually occurs in conjunction with straddle-type injuries to the perineum; the fixed bulbar urethra is crushed.
• The pendulous urethra is less susceptible to traumatic injury because of its mobility,
Posterior urethral injuries
• occurring exclusively as a result of pelvic fracture.
Urological management differs depending on the location of injury.
19
Presentation
Findings that suggest urethral injury include• blood at the urethral meatus ( cardinal sign)
• genital or perineal hematoma,
• pelvic fracture,
• penetrating penile injury,
• inability to void, &
• distended bladder.
20
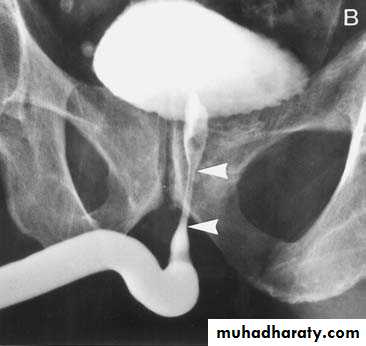
Diagnosis
All patients with a suspected urethral injury should undergo a retrograde
urethrogram (RUG)
21
Classification of Urethral Injury
• Classification based on t he extent of injury• a. No urethral tear --urethral contusion
• b. Partial urethral tear
• c. Complete urethral transection
2. Classification based on location
• a. Anterior urethral injury--- bulbar
• b. Posterior urethral injury– pelvic #
22
Anterior Urethral Injury
arise from blunt or penetrating trauma. the most frequently injured segment is Bulbar urethraBulbar urethral injury
• a. Usually caused by a straddle injury (falling astride onto a fence ) ,bicycle accidents, kicks to perineum or a direct blow to the perineum in which the urethra is crushed against the pubic bone.
• b. May present with a "butterfly" shaped hematoma on the perineum and ascrotal hematoma (blood confined to Colles' fascia attachments).
23

24
Treatment
Anterior urethral injuries are usually managed by bladder drainage (witha suprapubic tube or
trial to pass urethral catheter (single trial)
25
Initial treatment Anterior urethral injuries are usually managed by bladder drainage (with a suprapubic tube or urethral catheter
26
Delayed reconstruction
Stricture management depends on location, severity, and extent of the stricture.Options include
• Metal dilation,
• internal urethrotomy,
• excision with primary end-to-end anastomosis,
27
Posterior Urethral Injury
The posterior urethra consists of the prostatic and membranous urethra.
Almost all posterior urethral injuries are caused by pelvic fracture from blunt trauma. Urethral injury occurs in 10% of men with pelvic fractures.
28
Pelvic fracture


29
DX
The diagnosis of posterior urethral injury is suggested by a history of pelvic fracture,
• Triad of pelvic fracture, blood at the meatus and inability to void are diagnostic of urethral injury
RUG
30
Posterior Urethral Injury
The prostate and bladder are often pushed cephalad by hematoma, resulting in a high-riding prostate on rectal exam " pie in the sky" bladder on cystogram.
The continuity is disrupted by intervening scar tissue.
31
Initial treatment
Acute management of these patients should be directed at hemodynamic resuscitation, bony fixation, &bladder drainage via suprapubic cystostomy catheter.
these patients almost always develop urethral obliteration
A period of urethral rest at least 3 months after injury , so that the tissues have a chance to stabilize and delineate
32
Delayed treatment
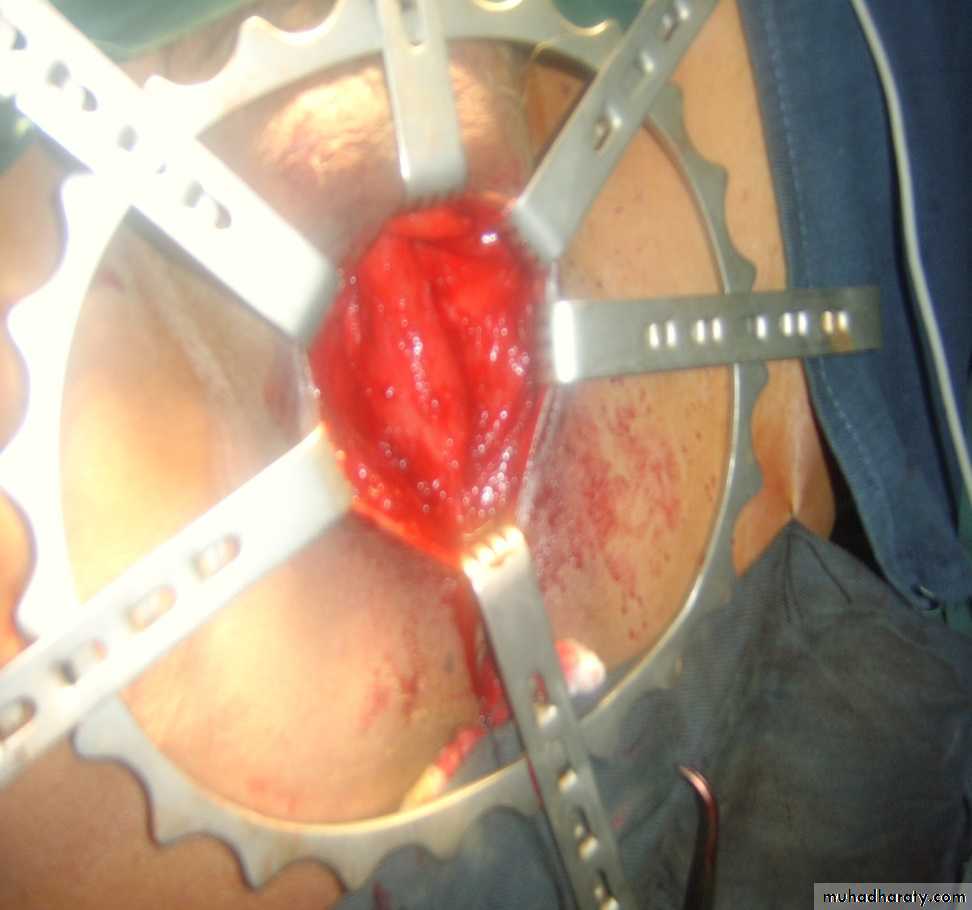
The surgical approach is usually a perineal incision with excision of the strictured area and end to end anastomosis. (urethroplasty)33
Urethroplasty

34
Iatrogenic urethral injury
Most commonly result from traumatic urethral instrumentationTraumatic Foley catheter removal without prior balloon deflation.
Theses injuries usually result in minor contusion that heal with few sequalae.
Treatment by single trial of catheter insertion if failed suprapubic cystostomy
35