
ADRENAL GLANDS DISEASESTUCOMInternal Medicine Dr. Hasan.I.Sultan
Functional anatomy and physiologyThe adrenal glands lie at the superior pole of each kidney. Each adrenal gland weighs approximately of 4-5 g.
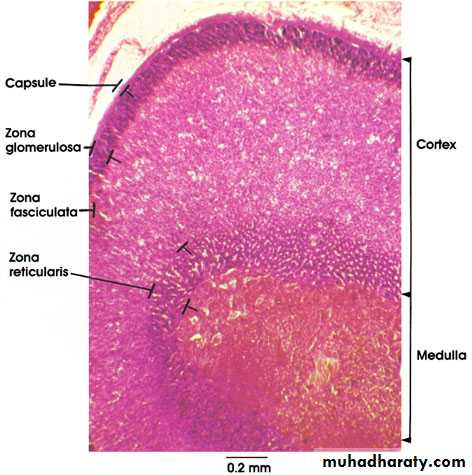
composed of two distinct regions: the cortex and the medulla
adrenal cortex: represents 90% of adrenal gland, consists of three anatomic zones;
Outer zona glomerulosa, which secretes the mineralocorticoid aldosterone
Intermediate zona fasciculata, which secretes cortisol
Inner zona reticularis, which secretes adrenal androgens
The adrenal medulla; represents 10% of adrenal gland, its the center of the adrenal gland, which secrets catecholamines: epinephrine, norepinephrine and dopamine in response to stress and activation of sympathetic nervous system.
The synthesis of all steroid hormones begins with cholesterol and is catalyzed by a series of regulated, enzyme-mediated reactions.
Adrenal gland is under control of:
• Hypothalamic-pituitary-adrenal (HPA) axis; regulate cortisol and androgen production.
• Renin-angiotensin-aldosterone (RAA) system.


Regulation of the hypothalamic-pituitary-adrenal (HPA) axis. CRH, corticotropin-releasing hormone; ACTH, adrenocorticotropic hormone.

Glucocorticoids;
Cortisol is the major glucocorticoid in humansHighest in the morning and lowest in the middle of the night
Increase in state of stress, including any illness
Affect metabolism, cardiovascular function, behavior, and the inflammatory/immune response
Its secretion is stimulated by (ACTH).
Cortisol can also activate mineralocorticoid receptors, but it normally inhibited by 11β-HSD2.

Prereceptor inactivation of cortisol and mineralocorticoid receptor action.
MineralocorticoidsAldosterone is the body's most important sodium-retaining hormone
Under influence of renin-angiotensin-aldosterone system
Renin secretion from the juxtaglomerular apparatus in the kidney is stimulated by low perfusion pressure in the afferent arteriole, low sodium concentrations at the macula densa, or increased sympathetic nerve activity.


Regulation of the renin-angiotensin-aldosterone (RAA) system.
Adrenal androgensAre secreted in response to ACTH
Initiation of puberty (the adrenarche).
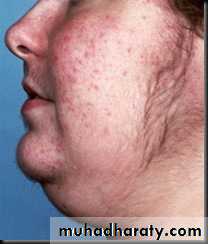
Excess adrenal androgen secretion results in acne, hirsutism, and virilization
Catecholamines:
Are produced mainly by the chromaffin cells of the adrenal medulla and the sympathetic nervous fibers.
Which includes noradrenaline (norepinephrine), adrenaline (epinephrine) and dopamine.
Prepare the body for physical activity (fight or flight response). Some typical effects are increases in heart rate, blood pressure, blood glucose, and sympathetic activation.
No clinical consequences attributable to deficiency of circulating catecholamines.

Disorders of adrenal glands
• Cushing's syndrome.• Adrenal insufficiency.
• Other adrenal disease including;
• Congenital adrenal hyperplasia
• Primary hyperaldosteronism
• Phaeochromocytoma
Cushing's syndrome
Cushing's syndrome is a syndrome that reflects excessive tissue exposure to cortisol.Most common cause is iatrogenic; prolonged administration of synthetic glucocorticoids
Non-iatrogenic Cushing's syndrome is rare
Cushing's disease and adrenal tumour are four times more common in women
Ectopic ACTH syndrome is more common in men
Aetiology
ACTH-dependentPituitary adenoma secret ACTH (Cushing's disease)
Ectopic ACTH syndrome (e.g. bronchial carcinoid, small-cell lung carcinoma, pancreatic neuro-endocrine tumour)
latrogenic (ACTH therapy)
Non-ACTH-dependent
Iatrogenic (chronic glucocorticoid therapy for asthma)
Adrenal adenoma
Adrenal carcinoma
Clinical Manifestations
Fat redistribution (dorsocervical and supraclavicular fat pads, centripetal obesity, weight gain) (95%)
Menstrual irregularities (80% of affected women)
Thin skin/plethora (80%)
Moon facies (75%)
Increased appetite (75%)
Hypertension (75%)
Altered mentation (poor concentration, decreased memory, euphoria) (70%)
Diabetes mellitus/glucose intolerance (65%), Striae (65%), Hirsutism (65%), Proximal muscle weakness (60%), Psychological disturbances (emotional lability, depression, mania, psychosis) (50%), Decreased libido/impotence (50%).
Acne (45%), Osteoporosis/pathologic fractures (40%), Virilization (in women) (40%), Easy bruisability (40%), Poor wound healing (40%), Edema (20%), Increased infections (10%) and Cataracts (5%).



Ectopic ACTH syndrome
Very high ACTH level (no negative feedback) is associated with marked pigmentation.Very high cortisol levels overcome the barrier of 11β-HSD2 in the kidney and cause hypokalemic alkalosis that leads to myopathy and hyperglycemia (by inhibiting insulin secretion).
The onset is usually rapid and may be associated with cachexia.
Prereceptor inactivation of cortisol and mineralocorticoid receptor action.

Investigations
Whether the patient has Cushing's syndrome, and to elucidate the aetiology.
There is no place for a random measurement of daytime plasma cortisol.
A-Does the patient have Cushing's syndrome?
1-Urine free cortisol; 24-hr timed collection, normal range depends on assay
50 μg/24 hours --- normal.
100 and 500 μg/24 hours --- Cushing's disease
greater than 500 μg/24 hours --- ectopic ACTH syndrome and cortisol-secreting adrenal adenomas or carcinomas.
2-Diurnal rhythm of plasma cortisol; the plasma concentration is highest in the early morning (between 6:00 and 8:00 am)= 8- 25 μg/dL and lowest around midnight= less than 5 μg/dL.
3-Overnight dexamethasone suppression test (suspected Cushing's syndrome); 1 mg orally at midnight; measure plasma cortisol at 0800-0900 hrs. Plasma cortisol < 60 nmol/l (< 2.2 μg/dl) excludes Cushing's.
4-Low-dose dexamethasone suppression test (to confirm Cushing's syndrome); 0.5 mg 6-hourly for 48 hrs; sample 24-hr urine cortisol during second day and 0900-hr plasma cortisol after 48 hrs
Urine cortisol < 100 nmol/day (36 μg/day) or plasma cortisol < 60 nmol/l (< 2.2 μg/dl) excludes Cushing's
5-Insulin tolerance test; Peak plasma cortisol > 120% of baseline excludes Cushing's.
B-What is the cause of the Cushing's syndrome?1-Basal ACTH levels; are normal or elevated in Cushing's disease and the ectopic ACTH syndrome and are suppressed in adrenal Cushing's syndrome.
2-High-dose dexamethasone suppression test; 2 mg 6-hourly for 48 hrs; sample 24-hr urine cortisol at baseline and during second day
Urine cortisol < 50% of basal suggests pituitary-dependent disease.
> 50% of basal suggests ectopic ACTH syndrome
3-Corticotrophin-releasing hormone test; 100 μg ovine CRH i.v. and monitor plasma ACTH and cortisol for 2 hrs Peak plasma cortisol > 120% and/or ACTH > 150% of basal values suggests pituitary-dependent disease; lesser responses suggest ectopic ACTH syndrome.
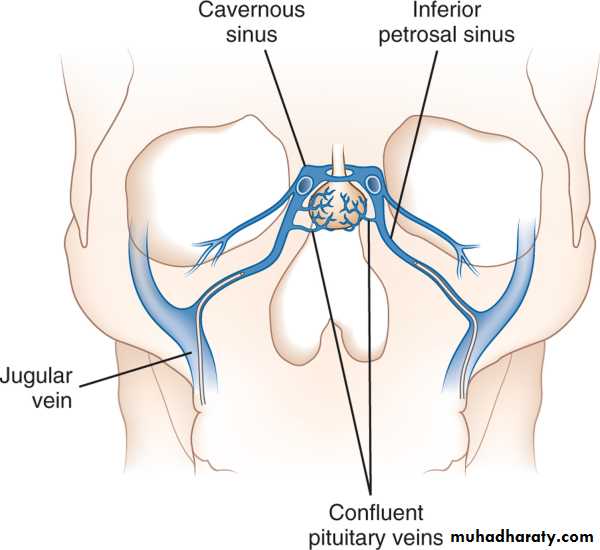
4- Inferior petrosal sinus sampling;
Catheters placed in both inferior petrosal sinuses and simultaneous sampling from these and peripheral blood for ACTH.
> 200% compared to peripheral ACTH, suggests pituitary-dependent disease.
< 150% suggests ectopic ACTH syndrome.
The test is usually performed by vascular radiologists on an outpatient basis. With local anesthesia, femoral catheters are advanced bilaterally up to the inferior petrosal sinuses. After confirmation of catheter location by fluoroscopy, several ACTH samples are drawn simultaneously from the right and left at the same time that a peripheral level is being drawn from an arm vein. CRH can also be injected to provoke ACTH release. Samples are then assayed for ACTH, and the pituitary-to-peripheral ratios are calculated.
5-Imaging
Pituitary gland MRI with gadolinium for localizing a pituitary microadenomas.CT or MRI detects adrenal adenomas or carcinomas
CXR ,CT chest or abdomen.




Management
1- Medical therapy; given for a few weeks prior to operation. (inhibit corticosteroid biosynthesis) including metyrapone, aminoglutethimide and ketoconazole.2- Cushing's disease; Trans-sphenoidal surgery with selective removal of the adenoma is the treatment of choice.
Nelson's syndrome (bilateral adrenalectomy in cushing's disease) that leads to pituitary macroadenoma and very high ACTH levels causing pigmentation. Nelson's syndrome can be prevented by pituitary irradiation.

3- Adrenal tumours
Adenomas: are removed surgically
Carcinomas are resected if possible + tumour bed irradiated + adrenolytic drug mitotane
Metastases; cytotoxic chemotherapy
4- Ectopic ACTH syndrome
Localised tumours causing this syndrome (e.g. bronchial carcinoid) should be removed
Non-resectable malignancies, using medical therapy
Adrenal insufficiency
Adrenal insufficiency results from inadequate secretion of cortisol and/or aldosterone.A high index of suspicion is therefore required in patients with unexplained fatigue, hyponatraemia or hypotension.
Aetiology; The most common cause is due to an ACTH deficiency (i.e. secondary adrenocortical failure), usually because of inappropriate withdrawal of chronic glucocorticoid therapy.
Secondary (↓ACTH);
Withdrawal of suppressive glucocorticoid therapyHypothalamic or pituitary disease
Primary (↑ACTH); usually describe as Addison's disease
Common causes;
Autoimmune
Sporadic
Polyglandular syndromes
Tuberculosis
HIV/AIDS
Metastatic carcinoma
Bilateral adrenalectomy
Rare causes;
Lymphoma
Intra-adrenal haemorrhage (Waterhouse-Friedrichsen syndrome following meningococcal septicaemia)
Amyloidosis
Haemochromatosis
Corticosteroid biosynthetic enzyme defects;
Congenital adrenal hyperplasias
Drugs: Aminoglutethimide, metyrapone, ketoconazole, etomidate etc.
Clinical features of adrenal insufficiency
Glucocorticoid insufficiencyMineralocorticoid insufficiency
ACTH excess
Adren androgen insufficiency
Withdrawal of exogenous glucocorticoid
+
-
-
+
Hypopituitarism
+
-
-
+
Addison's disease
+
+
+
+
Congenit adrenal hyperplasia (21 OHase deficiency)
+
+
+
-
Clinical features
Weight loss MalaiseWeakness AnorexiaNausea Vomitingdiarrhoea or constipationPostural hypotensionShockHypoglycaemiaHyponatraemia (dilutional)Hypercalcaemia
HypotensionShockHyponatraemia (depletional)Hyperkalaemia
PigmentationSun-exposed areas Pressure areas, e.g. elbows, kneesPalmar creases, knucklesMucous membranesConjunctivae
Recent scars
Decreased body hair and loss of libido, especially in female





Acute adrenal crisis
Circulatory shock with severe hypotensionHyponatraemia, hyperkalaemia and, in some instances, hypoglycaemia and hypercalcaemia.
Muscle cramps, nausea, vomiting, diarrhoea and unexplained fever may be present.
The crisis is often precipitated by intercurrent disease, surgery or infection.
Treatment should not be delayed pending results of investigations.
Investigations
A- Assessment of glucocorticoids;
1- Random plasma cortisol is usually low in patients with adrenal insufficiency, but it may be within the normal range yet inappropriately low for a seriously ill patient.
2- ACTH stimulation test
Diagnosis of primary or secondary adrenal insufficiency
Assessment of hypothalamic-pituitary-adrenal axis in patients taking suppressive glucocorticoid therapy
Dose; 250 μg ACTH (Synacthen) by I.M. injection at any time of day
0 and 30 minutes for plasma cortisolNormal subjects plasma cortisol > 460 nmol/l (∼170 μg/dl) either at baseline or at 30 minutes
B- Assessment of mineralocorticoids;
plasma renin activity is high, with plasma aldosterone is low. Hyponatraemia and Hyperkalaemia.


Tuberculosis cause adrenal calcification seen on plain abdominal X-ray
Management1- Glucocorticoid replacement;
Cortisol (hydrocortisone) is the drug of choice, given by mouth, 15 mg on waking and 5 mg at ∼1800 hrs.
An adrenal crisis; intravenous hydrocortisone succinate 100 mg and intravenous fluid (normal saline and 10% dextrose for hypoglycaemia). Parenteral hydrocortisone should be continued (100 mg I.M. 6-hourly) until gastrointestinal symptoms abate before starting oral therapy.
2- Mineralocorticoid replacement;
fludrocortisone from being metabolised by 11β-HSD2 and thereby confers a longer half-life and access to mineralocorticoid receptors. The usual dose is 0.05-0.1 mg daily
In adrenal crisis, however, rapid replacement of sodium deficiency is more important than administration of fludrocortisone. Intravenous saline should be infused as required to normalise haemodynamic indices
Advice to patients on glucocorticoid replacement
1-Intercurrent stress; e.g. Febrile illness-double dose of hydrocortisone2-Surgery;
Minor operation; hydrocortisone 100 mg i.m. with pre-medication
Major operation; hydrocortisone 100 mg 6-hourly for 24 hours, then 50 mg i.m. 6-hourly until ready to take tablets
3-Vomiting; Must have parenteral hydrocortisone if unable to take by mouth
4- Steroid card; Patient should carry this at all times give information regarding diagnosis, steroid, dose and doctor
5- Bracelet; Patients should be encouraged to buy one of these

Primary hyperaldosteronism
Hypertensive patients with hypokalaemia (including hypokalaemia induced by thiazide diuretics), poor control of blood pressure with conventional therapy, or presentation at a young age, or family history of early onset hypertension.Most patients with Primary hyperaldosteronism have Idiopathic bilateral adrenal hyperplasia, while only minority have adrenal adenoma secreting aldosterone (Conn's syndrome)
Clinical features
Asymptomatic
Sodium retention may cause oedema.
Hypokalaemia causes muscle weakness (or even paralysis, especially in Chinese), polyuria (secondary to renal tubular damage which produces nephrogenic diabetes insipidus) and occasionally tetany (because of associated metabolic alkalosis and low ionised calcium).
B.P is elevated but accelareted phase is rare.
Investigations
Biochemical;Hypokalaemia and elevated bicarbonate. Plasma sodium is usually in upper end of normal range.
Measurements of plasma renin activity and aldosterone . renin is low and aldosterone level is high.
Localisation;
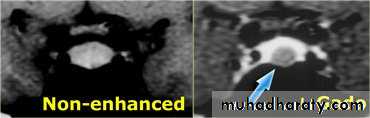
Abdominal CT: to localize the tumour.
adrenal CT should only be performed when the biochemistry supports the diagnosis of adrenal tumour.



• Conn's adenoma. A-CT scan of left adrenal adenoma (arrow). B- 131Iodo-norcholesterol scan showing uptake in left adrenal adenoma (arrow). C-The tumour is 'canary yellow' because of intracellular lipid accumulation.
Management
Idiopathic bilateral adrenal hyperplasia: Mineralocorticoid receptor antagonists (spironolactone or eplerenone) or potassium sparing diuretics are used.Conn's adenoma;
Medical therapy few weeks before unilateral adrenalectomy.
Phaeochromocytoma
This is a rare tumour of chromaffin tissue that secretes catecholamines and is responsible for less than 0.1% of cases of hypertension.Rule of tens
∼10% are malignant
∼10% are extra-adrenal (i.e. elsewhere in the sympathetic chain)
∼10% are familial

Clinical features
These depend on the pattern of catecholamine secretionHypertension (usually paroxysmal; often postural drop of blood pressure)
Paroxysms of:
Pallor (occasionally flushing)
Palpitations
Sweating
Headache
Anxiety (fear of death-angor animi)
Abdominal pain, vomiting
Constipation
Weight loss
Glucose intolerance
Complication of hypertension: e.g. stroke, myocardial infarction, left ventricular failure, hypertensive retinopathy or accelerated-phase hypertension.
Familial syndromes associated with phaeochromocytoma including neurofibromatosis, Von Hippel-Lindau syndrome and MEN type 2.
Investigations
Biochemical; Measuring the hormones (adrenaline/epinephrine, noradrenaline/norepinephrine and dopamine) in plasma or their metabolites (e.g. vanillyl-mandelic acid (VMA), conjugated metanephrine and normetanephrine) in urine.Samples should be collected during a period of attacks.
Localisation; abdominal CT or MRI.


CT scan of abdomen showing large left adrenal phaeochromocytoma. The normal right adrenal (white arrow) contrasts with the large heterogeneous phaeochromocytoma arising from the left adrenal gland (black arrows).

Mottled brown tan mass is the neoplasm filling up the adrenal medulla. • Blue arrow points to residual normal medulla. • Yellow arrows point to golden yellow adrenal cortex. • Black discoloration around the specimen is india ink applied to assess the margins of the specimen
Management
Surgery is the curative treatmentPatient should be prepared before surgery for at least 6 weeks with oral α-blocker phenoxybenzamine and restoration of normal plasma volume.
During surgery sodium nitroprusside and the short-acting α-antagonist phentolamine are useful in controlling hypertensive episodes which may result from anaesthetic induction or tumour mobilisation
Post-operative hypotension may occur and require volume expansion and, very occasionally, noradrenaline (norepinephrine) infusion.
Thanks
Quiz
Q1- List the complications of GERD.Q2- A 24 year old man with iron deficiency anemia, weight loss and chronic diarrhea present to you complain from an itchy vesicular rash on his elbows. What is the diagnosis?
Q3- List the extraintestinal features of active ulcerative colitis.
Q4- A 50 year old male present with massive hematemesis and splenomegaly. What is the diagnosis?
Q5- Which of the following tests most reliable distinguish active hepatitis B from carrier state?
A-HBs Ag B-anti HBc Ab C-HBc Ag D-HBe Ag