Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
1
To explain the testicular cancers features, diagnosis and management
To explain different types of scrotal and testicular infections
To specify the anatomic causes predisposing to torsion, clinical features,
diagnosis, and management
To differentiate torsion from epididymorchitis
To clarify the types of testicular injury and their management.
Causes of acute scrotum:
Epididymitis
Orchitis
Testicular trauma
Testicular torsion
Incarcerated scrotal hernia
Testicular tumor
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
2
•
Cryptorchidism
•
Testicular atrophy.
•
Sex hormones disturbance
•
HIV infection
•
Infertility
•
Family Hx of testicular cancer
•
Past Hx of testicular cancer in the contralateral testis.
Rare, but most common solid malignancy in young males
15-35 years
Any solid testicular mass or acute
hydrocele
in young patient you must rule
out malignancy
Slightly more
common in right
testis (corresponds with slightly higher
incidence of right-sided cryptorchidism)
2-3% bilateral (simultaneously or successively)
Primary
1% of all malignancies in males
Cryptorchidism has increased risk (10-40x) of malignancy
1. 95% are
germ cell tumors
(all are malignant)
A.
seminoma
(35%) types: classic, anaplastic, spermatocytic
B.
NSGCT
(non seminomatous germ cell tumor) types: embryonal cell
carcinoma (20%), teratoma (5%), choriocarcinoma (<1%), yolk sac
(<<1%), mixed cell type (40%)

Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
3
2. 5% are
non-germ cell tumors
(usually benign) types: Leydig (testosterone,
precocious puberty), Sertoli (gynecomastia, decreased libido)
Secondary
male >50 years
usually lymphoma
, leukemia or metastases (e.g. lung, prostate, GI)
Painless
testicular
enlargement
(painful if intratesticular hemorrhage or
infarction)
Dull, heavy
ache
in lower abdomen, anal area or scrotum
Associated
hydrocele
(10%)
Infertility
(rarely presenting complaint)
Gynecomastia
due to secretory tumor effects
Supraclavicular and inguinal
lymphadenopathy
Abdominal mass
(retroperitoneal lymph node metastasis)
Rarely, patients present with
severe pain
and acute enlargement of the testis
because of hemorrhage into a neoplasm
Symptoms of metastatic
disease: abdominal or lumbar pain, chest pain,
dyspnea and hemoptysis
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
4
Local spread follows lymphatics
a)
right testis
to medial, paracaval, anterior and lateral nodes
b)
Left testis
to left lateral and anterior paraaortic nodes
c)
“cross-over
” metastases from right to left are fairly common, but
no reports from left to right
Hematogenous most commonly to lung, liver, bones, and kidney
Diagnosis is established by
pathological evaluation
of specimen obtained by
radical inguinal orchidectomy
Tumour markers
: β-hCG (human chorionic gonadotropin), LDH) lactate
dehydrogenase), AFP(alpha fetoprotein).
Testicular U/S
(hypoechoic area within tunica albuginea = high suspicion of
testicular cancer)
Needle aspiration contraindicated
Testes and scrotum have different lymphatic drainage (the scrotum
drains to the inguinal lymph nodes), therefore trans-scrotal approach for
biopsy or orchiectomy should be avoided.
Clinical:
CXR
(lung metastasis),
markers
for staging (β-hCG AFP , LDH),
CT
abdomen/pelvis (retroperitoneal lymphadenopathy)
Stage I:
disease limited to testis, epididymis, or spermatic cord
Stage II:
disease limited to the retroperitoneal nodes
Stage III:
disease metastatic to supradiaphragmatic nodal or visceral sites
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
5
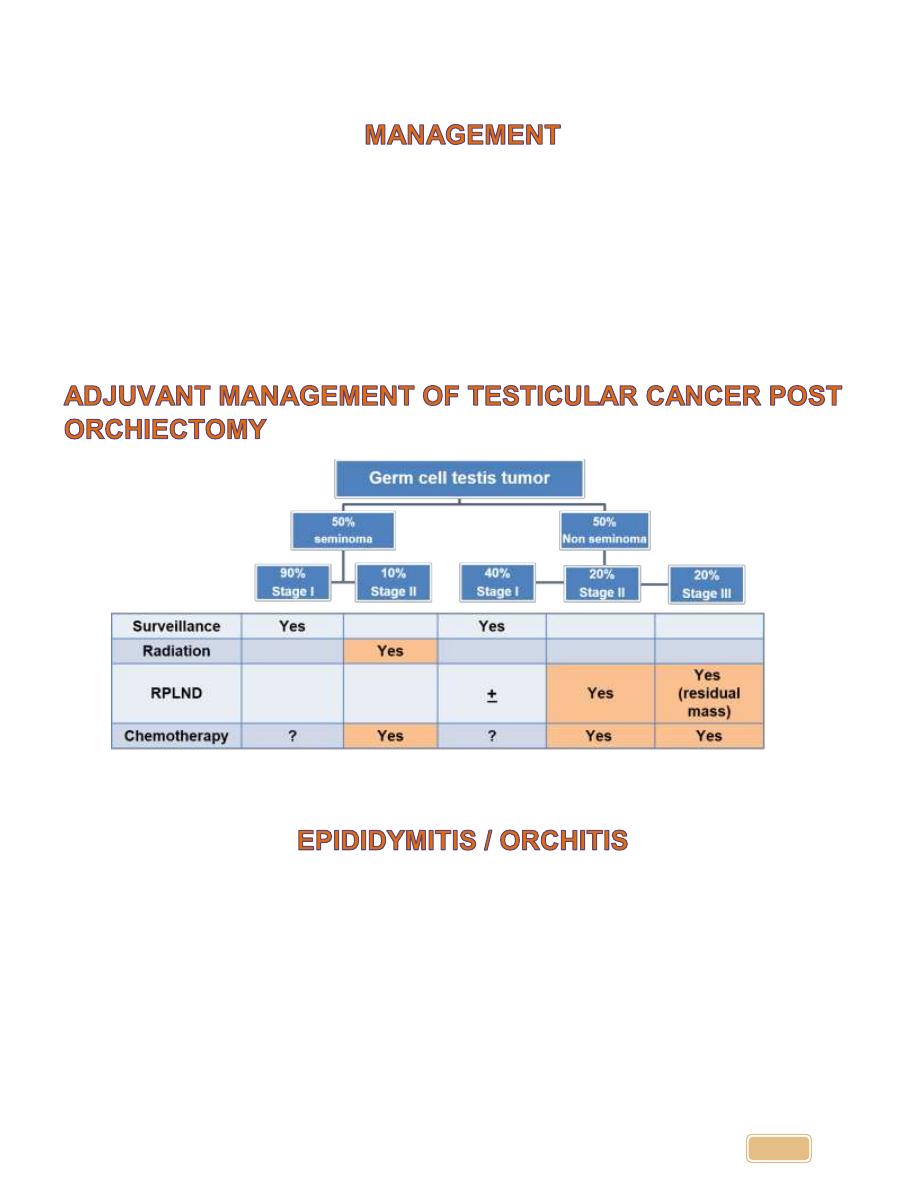
Orchiectomy
through inguinal incision for all stages
Consider sperm banking, testicular prosthesis
Prognosis
99% cured with stage I and II disease
70-80% complete remission with advanced disease
Definition: Clinical syndrome characterized by inflammation of the
epididymis and/or testicles (orchitis rarely exists in the absence of
epididymitis).
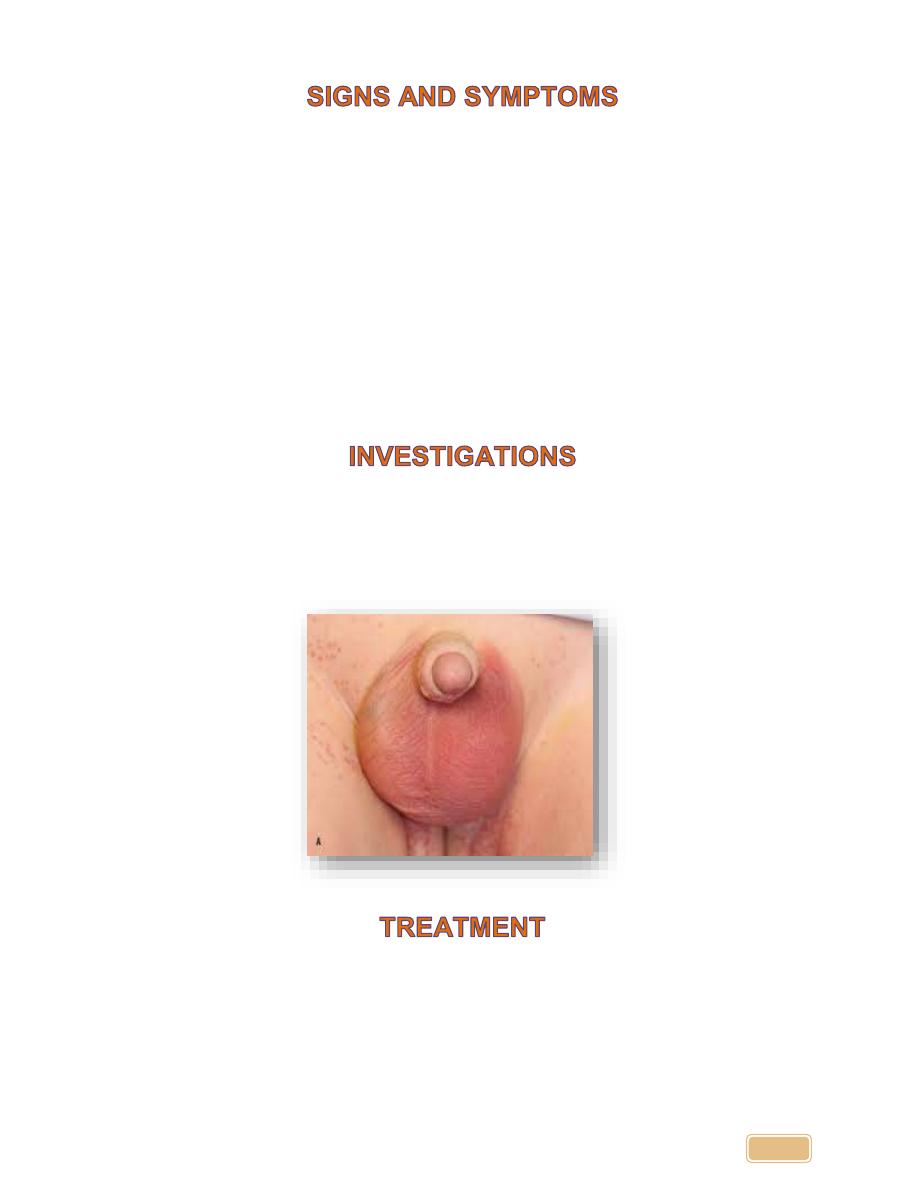
Painful swelling
in the scrotum, usually severe and develops rapidly over 24
to 48 hours (may be even more acute)
Often associated with
dysuria
or
irritative voiding symptoms
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
6
1-
Ascending:
in UTI, instrumentation, catheterization, or after cystoscope
and TUR. E.coli, proteus, staph, strept, and gonococcus.
2-
Blood borne infection
: post mumps.
Bacterial etiology most widely accepted:
E. coli (children)
E. coli (homosexual)
Neisseria gonorrhoeae
Chlamydia trachomatis
Mumps orchitis
rare due to immunization for mumps or occurring in
post-
pubertal boys
older than 10 years, begins 4
– 6 days after onset of parotitis
Testicular
torsion
Hemorrhage into an occult
testicular tumor
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
7
•
urethral
discharge
•
elevated
WBC count
•
History of
lower urinary symptom
, instrumentation or mumps.
•
Acute scrotal and groin
pain.
•
Constitutional symptoms of
fever, rigor & malaise
.
•
Swollen
red and
edematous
scrotal skin.
•
Testis and epididymis are swollen
tender
and matted together, mild
hydrocele is present.
•
Scrotal elevation relieves pain (Prehn’s sign +ve)
•
Digital rectal exam
to check for prostatitis recommended
•
Urinalysis
often unremarkable
•
Consider
scrotal ultrasound
with color flow Doppler if torsion,
tumor, or trauma suspected
•
Antibiotics:
for
2 weeks
. If the cause is prostatitis extend up to 30
days
•
bed rest
•
Hydration
•
analgesics
and / or anti- inflammatory agents.
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
8
•
scrotal elevation
is usually effective
•
Always treat the sexual partner if suspected secondary to an STD.
•
Patients may require
hospitalization
for I.V. antibiotics if systemically ill
•
Consider
follow-up scrotal ultrasound
if no resolution with appropriate
antibiotics (
to rule out abscess
)
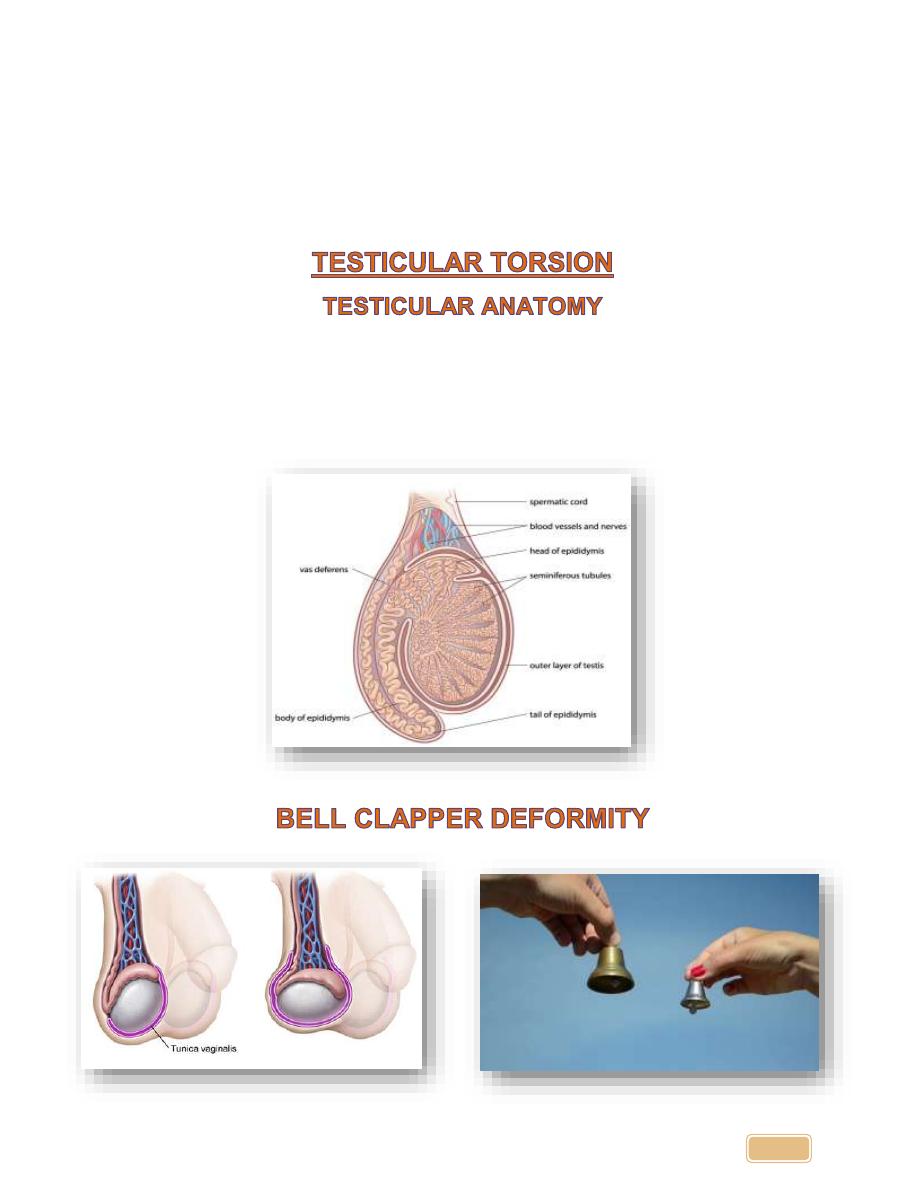
The normal testis is oriented in the vertical axis and the epididymis is above
the superior pole in the posterolateral position.
Most torsions occur due to
bilateral
anatomic abnormality.
Tunica vaginalis has a high insertion
posterior to the testis.
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
9
Bell
-clapper deformity Incidence 1:4000
Only
50% salvageable
with testicular loss from either atrophy or orchiectomy
Two peak periods:
first year of life and at puberty
10
times more likely in an undescended testis
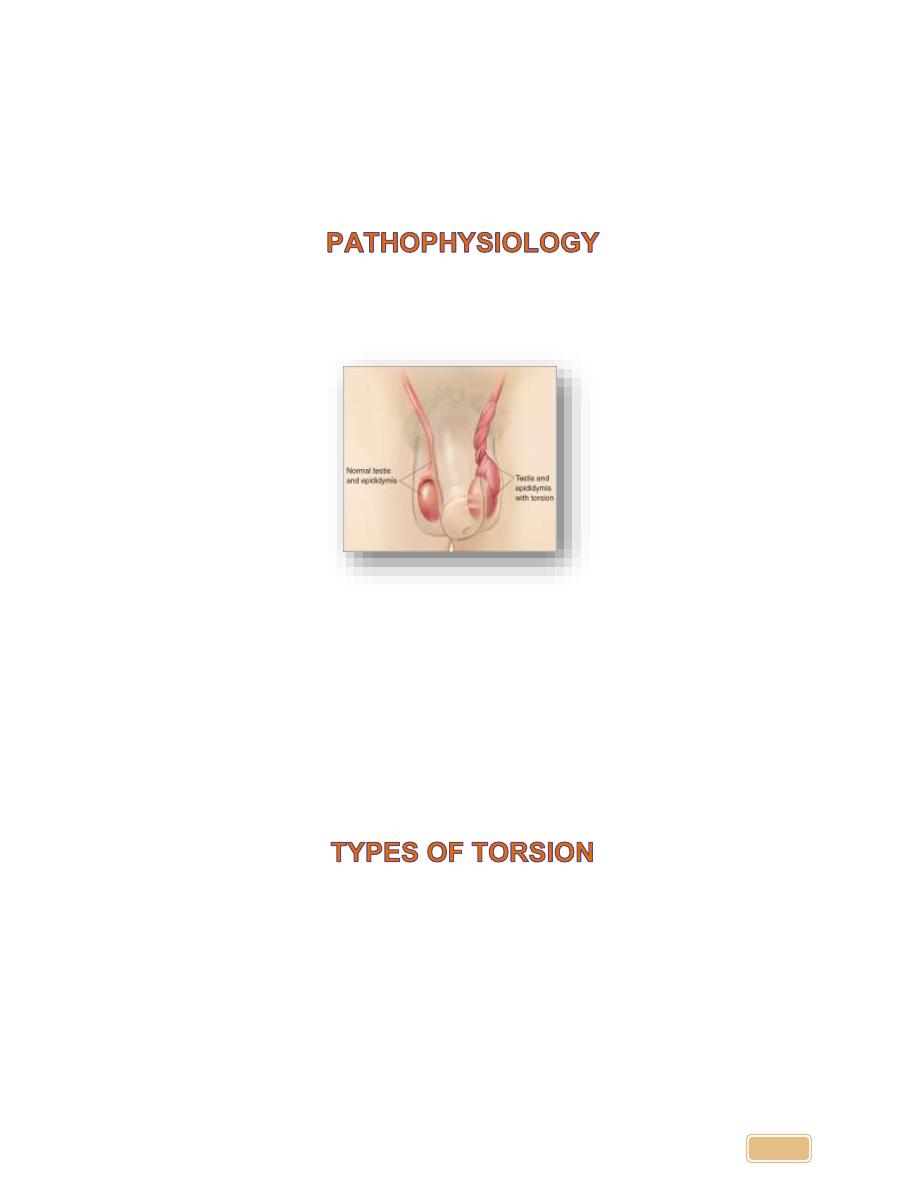
•
Initially venous return is obstructed and then venous thrombosis is
followed by arterial thrombosis
•
Degree of obstruction relates to the degree of rotation
•
Necrosis
develops in testicle with complete obstruction and
infarction
develops after arterial thrombosis
•
Rapid
swelling and edema
of the testis and scrotum, followed by scrotal
erythema
•
Damage
proportional to duration/extent
of vascular obstruction
•
Salvage rate of testis is 80-100% if pain lasts
less than 6 hours
•
Pain > 24 hours is associated with testicular infarction in 80%
1. Intravaginal: the testis rotates within the tunica vaginalis due to bell-
clapper deformity which occurs in puberty.
2. Extravaginal: in which the testis rotates along with the tunica vaginalis
due to poor attachment to the scrotum which occurs in the first year of
life.
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
10
40% report a history of similar pain that resolved spontaneously in the past
Typically no urinary symptoms
Often occurs after exertion or during sleep, cold weather, sport, trauma
•
Sudden onset of
scrotal pain
,but can be
inguinal or lower abdominal
.
May be constant or intermittent. Not
positional
•
Nausea
and
Vomiting
Hemiscrotum
is swollen
,tender, firm
High-riding testis
with
a transverse lie is classic sign
Loss of
cremasteric reflex
–
almost universal
Prehn’s sign
:Relief of scrotal pain by elevating testicle .
NOT
a reliable way
to distinguish
epididymitis from torsion
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
11
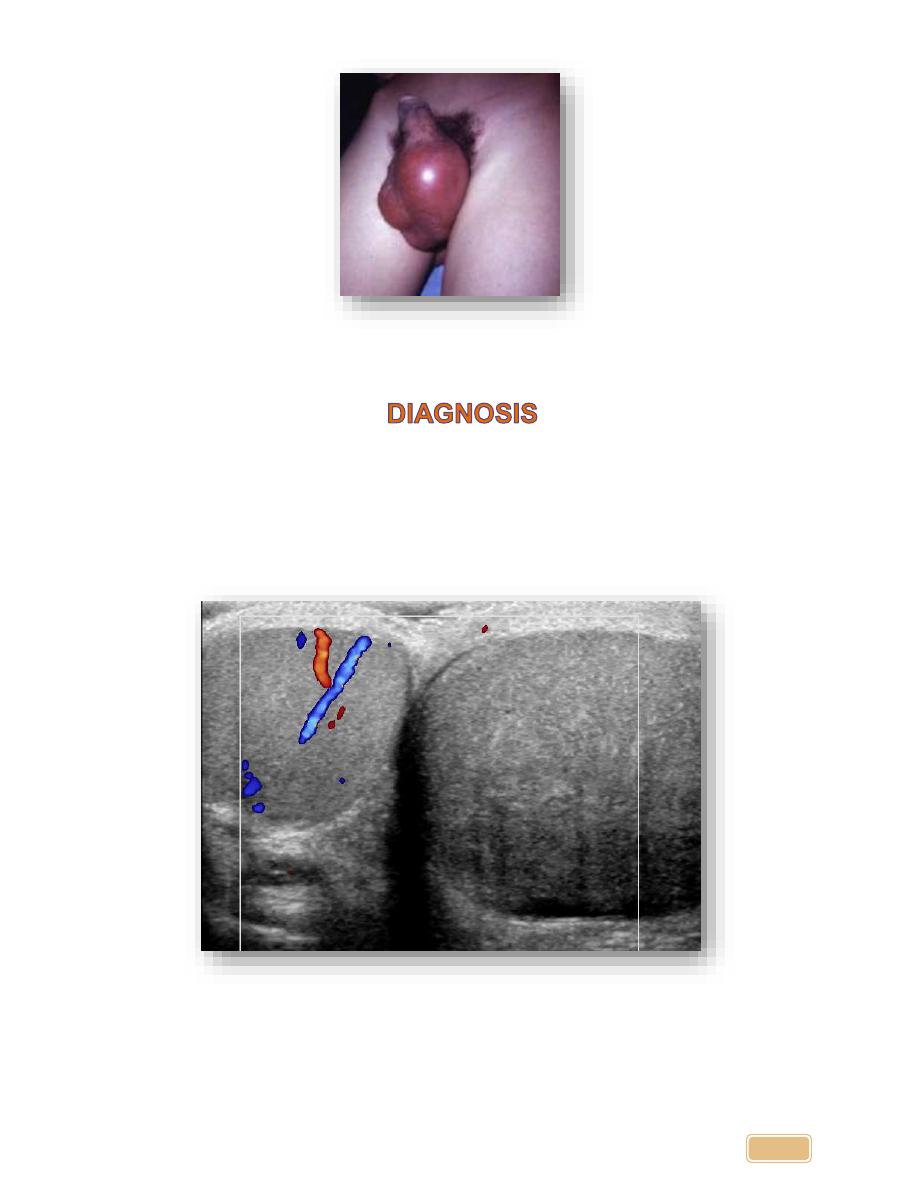
1.
Clinical
2.
Doppler
Ultrasononography
now is the test of choice for Diagnosis
of
torsion
.
3.
Radioisotope scans
.
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
12
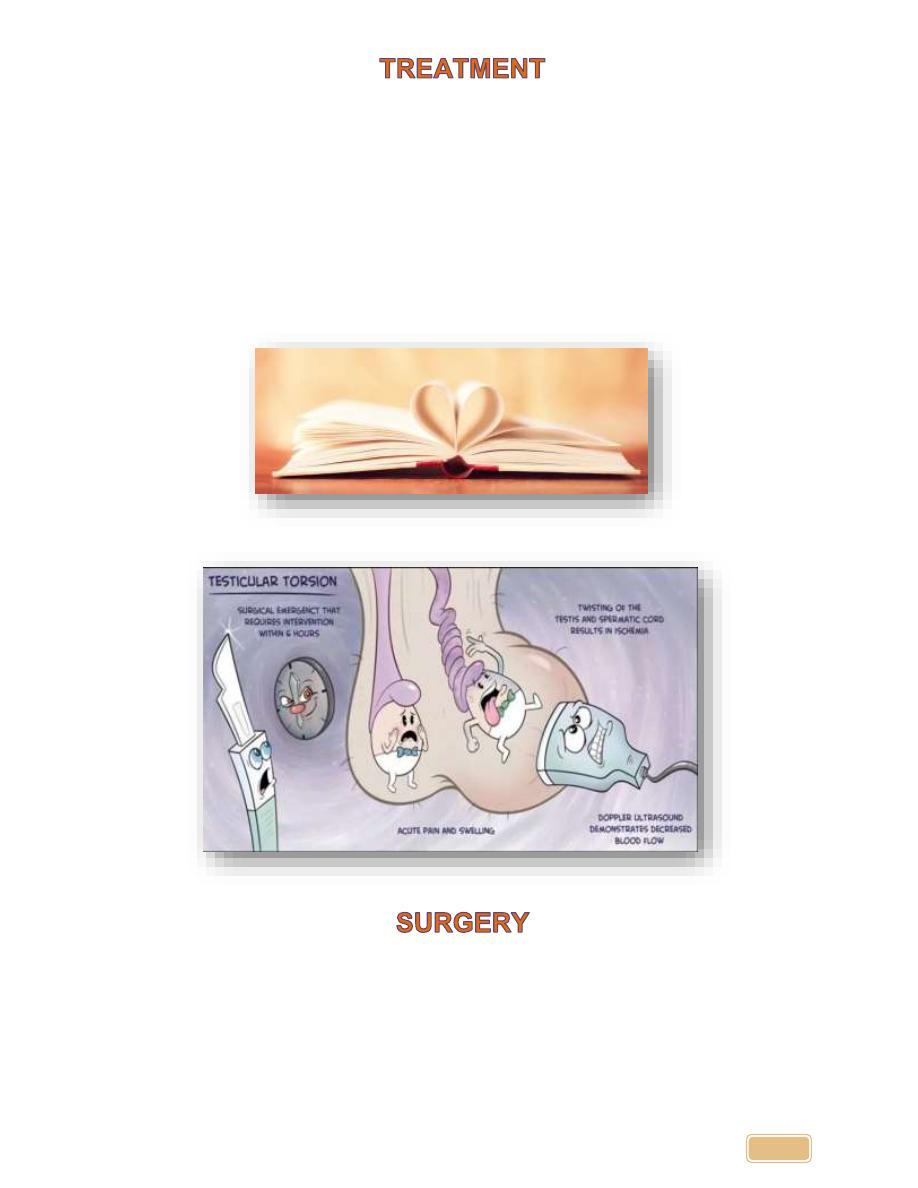
•
Immediate Urologic consultation for
surgical exploration and possible
orchiopexy
if diagnosis is obvious
•
Manual detorsion - Only a temporary action (just do it to relief the pain)
untill you prepare the patient for emergency exploration.
So exploration
and orchiopexy is mandatory even after detorsion.
•
Most torsions occur lateral to medial
,therefore detorsion should be
attempted in a medial to lateral direction
-
“
open the book
”maneuver
•
Imaging if diagnosis unclear, should NOT
delay
exploration if high
suspicion exists
Exploration
If
viable
:detorsion with fixation to the scrotal wall
If
Gangrene
:orchiectomy
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
13
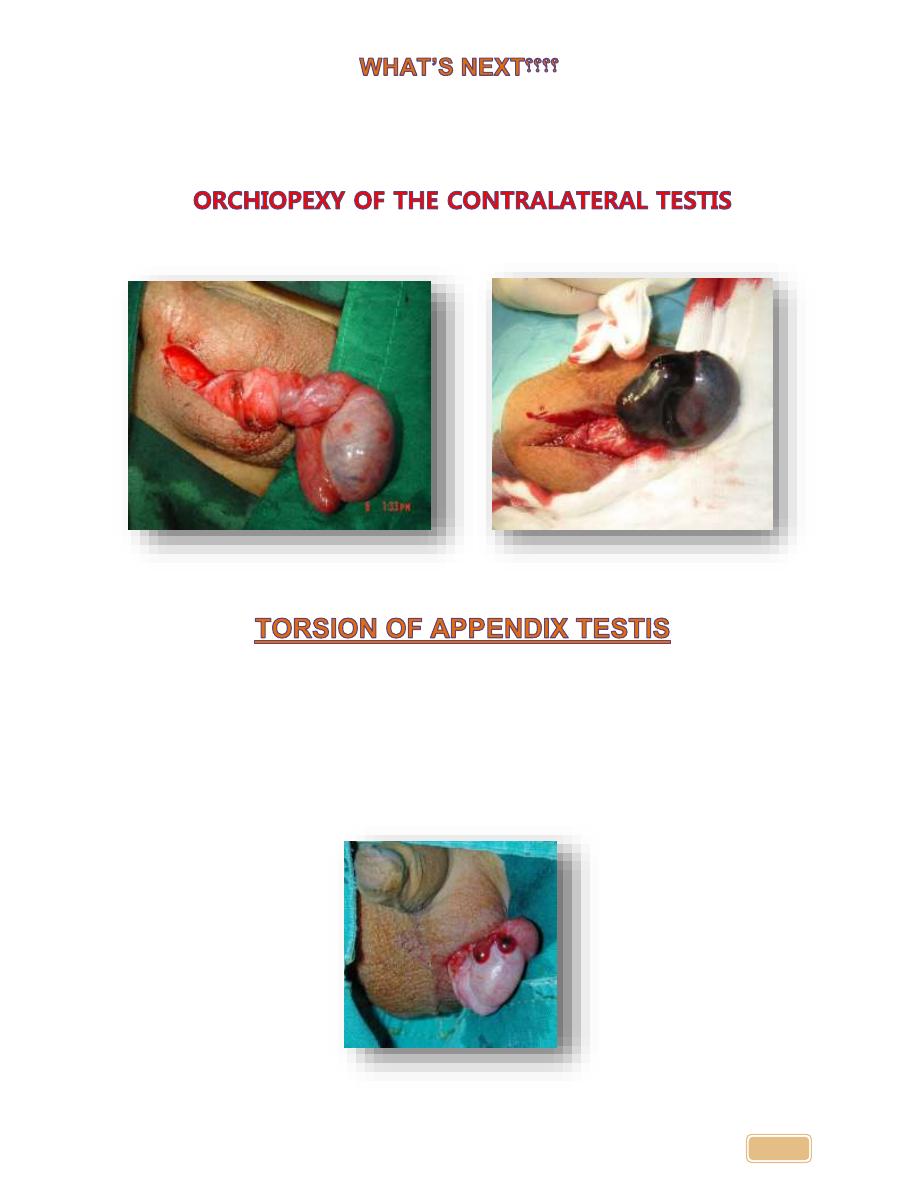
Was the problem solved???
Don’t you ever ever ever forget to do
Because bell-clapper deformity is a bilateral anomaly
•
Torsion of appendages is more common than
testicular torsion
•
Testicular and Epididymal appendages are
vestigial remnants of
the
wolffian and mullerian ducts respectively
•
Most frequent in pre-adolescent males 3-13, appendix testis
occur
more than
epididymal appendix
•
Cause unclear
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
14
•
Discrete, painful testicular mass
•
Symptoms less severe than torsion
.
•
No
nusea ,vomiting, or fevers
•
blue dot sign
•
Scrotal Support
•
Rest
•
Analgesia
•
Expect resolution of symptoms in 7-10 days with degeneration of
appendages
•
Testicular torsion is a urological
emergency
•
Bell clapper deformity is a bilateral
high insertion of the tunica vaginalis
•
Diagnosis
:examination and doppler study
•
Manual detorsion is done if possible
before surgery (open the book)
•
Exploration with fixation/orchiectomy
•
Fixation of the contralateral testis
•
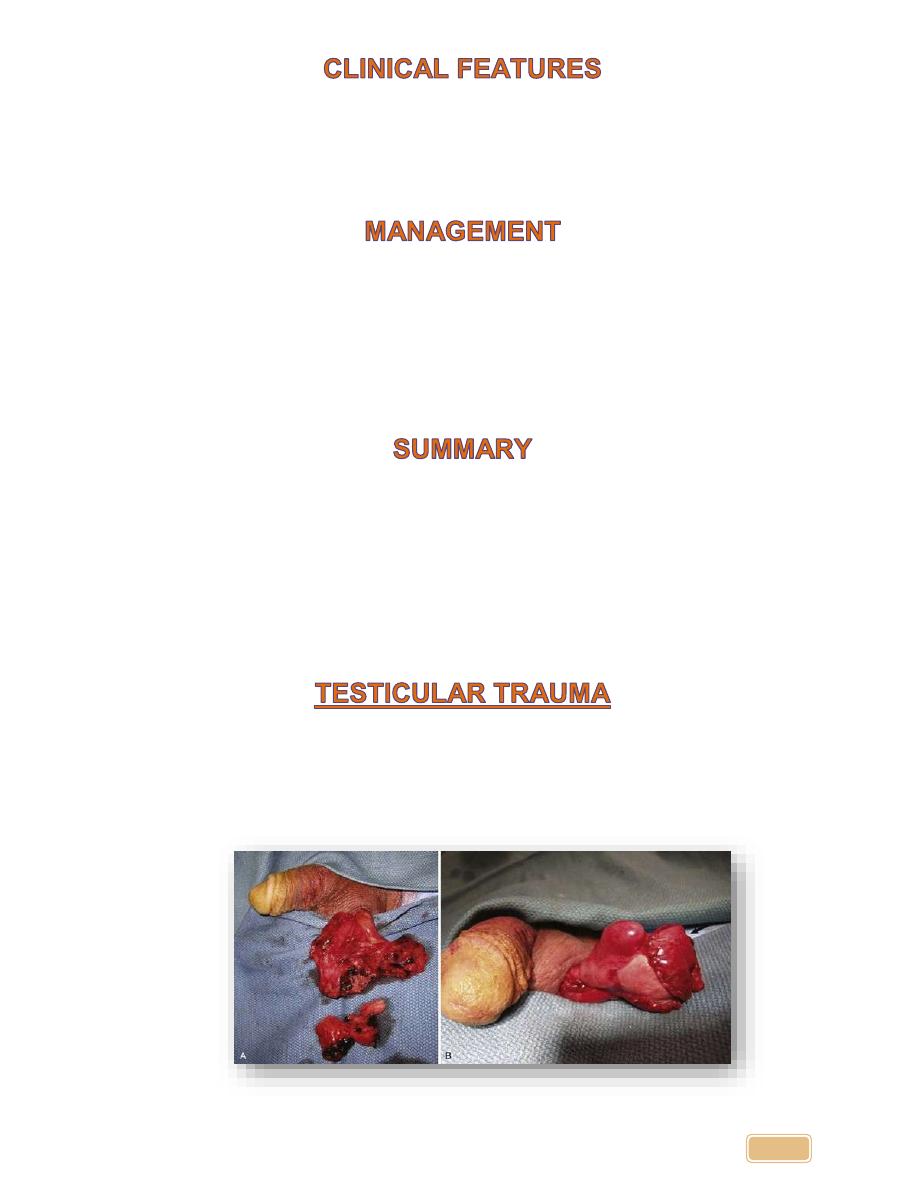
Testicular
rupture results when there is laceration of the tunica
albuginea of the testis
,such that testicular parenchyma may extrude.
•
It may occur from
either
blunt or penetrating trauma
.
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
15
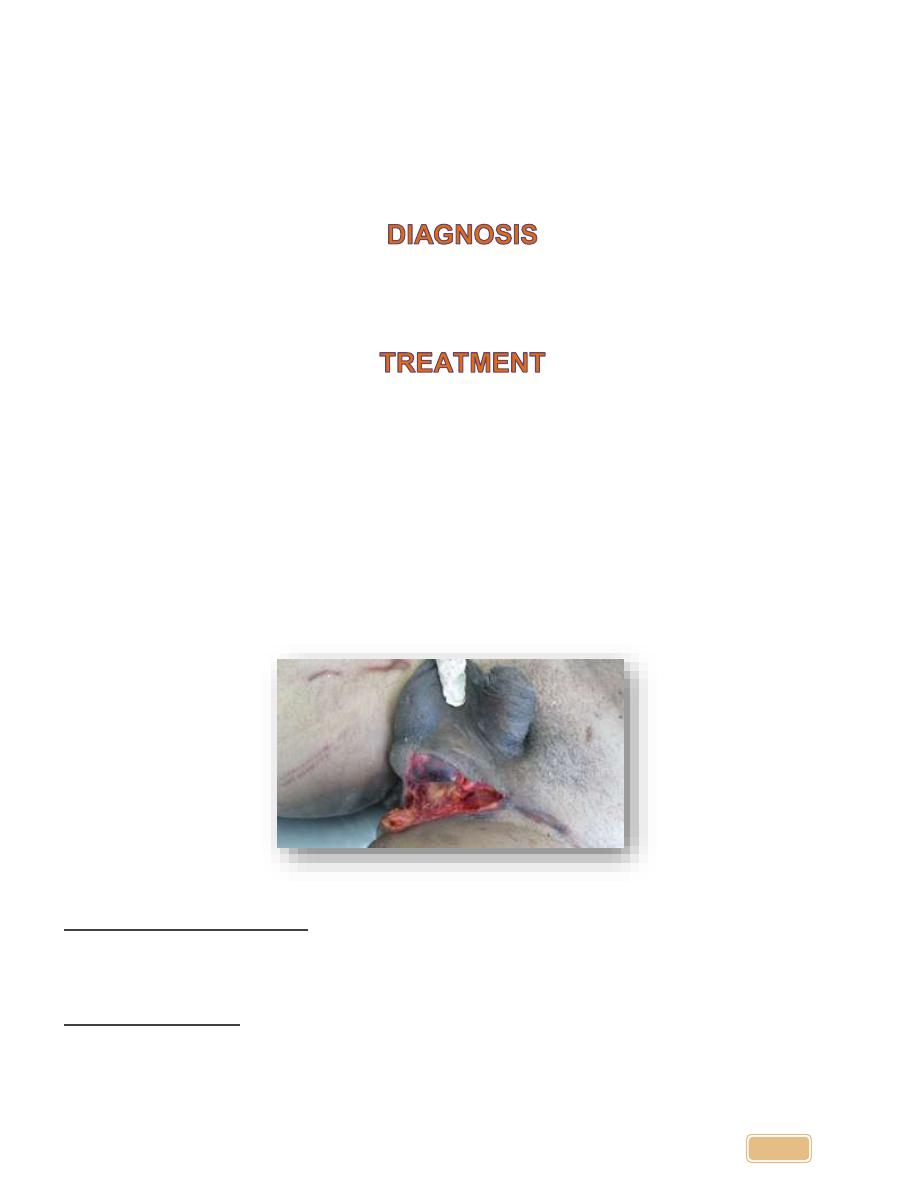
•
In
cases of
blunt trauma
,however, the incidence of testicular rupture
varies widely, and depends on the forces exerted, the mechanism of
injury, and testis mobility
.
•
Following blunt injury, the physical examination findings may include
swelling, tenderness or ecchymosis
.
1.
History, mechanism of injury
2.
Scrotal Ultrasonography
•
Testicular
rupture requires
surgical
repair
.
•
Large or painful
hematoceles may benefit from
drainage
.
•
For
intratesticular hematoma
( intact tunica albuginea, localized
hematoma within an otherwise intact testis) or local tenderness
(contusion
,)
a)
Observation
b)
Rest
c)
cold
packs
d)
and
analgesics .
For
penetrating trauma
a vertical incision may be easily
extended into the groin to expose the
spermatic cord
.
For
blunt trauma
a transverse incision over the injured
scrotal compartment is effective .
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
16
Torsion of the testes
Epidiymorchitis
• History:
• Sudden pain.
• Awake patient from sleep.
• Not associated with Constitutional
symptoms.
• No Irritative symptoms.
• History:
• Gradual pain.
• Associated with Constitutional
symptoms like fever, rigor, dysuria
because it is due to infection.
• Irritative symptoms.
• Exam:
• Testes lie transversely at the neck or
scrotum.
• No signs of inflammation.
• Cremasteric reflex is lost.
• Elevation of the testes not relieve the
pain (because it is ischemic pain).
• Cause secondary hydrocele in late
stage.
• Exam:
• Testes hang down.
• There are signs of inflammation on
the scrotal skin.
• Cremasteric could be preserved.
• Elevation of the testes may relieve
the pain (because it is hanging pain).
• Investigations:
• GUE normal.
• WBC normal.
• US (most important investigation).
• Doppler US (decreased blood flow).
• Investigations:
• GUE show UTI.
• WBC elevated.
• US (most important investigation).
• Doppler US (increased blood flow).
• Treatment:
• Note: always torsion need
exploration due to gangrene (you
have 6 hours only).
• Torsion = exploration.
• If viable testis = do orchiopexy.
• If gangrenous = do orchiectomy.
• The other testis should also be fixed
because the anatomical
predisposition is bilateral.
• In the first hours, it may be possible
to untwist the testis manually, then
early orchiopexy to avoid recurrent
torsion
• Treatment:
• Conservative therapy
• Antibiotics
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
17
Type
Varicocele
Spermatocele
Hydrocele
Testicular
torsion
Inguinal
hernia
Definition
• Dilatation and
tortuosity of
pampiniform
plexus
• A benign, sperm
filled epididymal
retention cyst
• Collection of serous
fluid that results
from a defect or
irritation in the
tunica vaginalis
• Twisting of the
testicle causing
venous occlusion
and
engorgement as
well as arterial
ischemia and
infarction
• Protrusion of
abdominal
contents
through the
inguinal canal
into the
scrotum
Etiology
• 15% of men
• Due to
incompetent
valves in the
testicular veins
• 90% left sided
• Multiple theories,
including:
• Distal obstruction
• Aneurysmal
dilations of the
epididymis
• Agglutinated
germ cells
• Usually idiopathic
• Found in 5-10% of
testicular tumours
• Associated with
trauma/infection
• Communicating:
patent processus
vaginalis, changes
size during day
(peds)
• Non-
communicating:
nonpatent
processus vaginalis
(adult)
• Trauma
• Cryptorchidism
•
“
Bell clapper
deformity
”
• Many occur in
sleep (50%)
• Necrosis of
glands in 5-6 h
• Indirect:
(through
internal ring,
often into
scrotum)
• Congenital:
Direct (through
external ring,
rarely into
scrotum)
• abdominal
muscle
• Weakness
Hx/P/E
•
“
Bag of worms
”
• Often painless
• Pulsates with
Valsalva
• Non-tender,
cystic mass
• Transilluminates
• Non-tender,
intrascrotal mass
• Cystic
• Transilluminates
• Acute onset
severe scrotal
pain,
• swelling
• Hi and transverse
testicle
(horizontal lie)
• Negative Phren
’
s
sign
• Absent
cremasteric
reflex
• A small bulge
in the groin
that may
increase in size
and disappear
when lying
down
• Can present as
a swollen or
enlarged
scrotum
• Discomfort or
sharp pain
–
especially
when straining,
lifting, or
exercising
Investigations
• P/E
• Valsava
• P/E
• U/S to rule out
tumor
• U/S to rule out
tumor
• U/S with color
flow Doppler
probe over
testicular artery
• Decrease uptake
on radioisotope
scan.
• Hx. and P/E
• Invagination of
the
• scrotum
• Valsalva
Dr. Ali Wafaa Al-Wefy M.D. Al-Mustansiriya University
18
Treatment
• Conservative
• Surgical ligation of
testicular veins
• Percutaneous vein
occlusion
(balloon,
sclerosing agents)
• Repair may
improve sperm
count/motility 50-
75%
• Conservative
• Avoid needle
aspiration as it
can lead to
infection,
reaccumulation
and spilling of
irritating sperm
within scrotum
• Excise if
symptomatic
• Conservative
• Needle drainage
• Surgical
• Emergency
surgical
exploration and
bilateral
orchiopexy
• Orchiectomy if
poor prognosis
• Surgical repair
Condition
Pain
Palpation
Additional findings
Torsion
+
Diffuse tenderness
Horizontal lie of testicle
Absent cremasteric reflex, negative
Prehn’s sign
Epididymitis
+
Epididymal tenderness
Present cremasteric reflex, positive
prehn’s sign
Orchitis
+
Diffuse tenderness
Present cremasteric reflex, positive
prehn’s sign
Hematocele
+
Diffuse tenderness
No transillumination
Hydrocele
_
Testis not separable from
hydrocele, cord palpable
Transillumination, Hx of trauma
Spermatocele
_
Testis separable from
spermatocele, cord palpable
Transillumination
Varicocele
_
Bag of worms
No transillumination, increases in
size with Valsalva, decrease in size
if supine
Indirect
inguinal hernia
_ (
+ if
strangulated)
Testis separable from
hernia, cord not palpable,
cough impulse may transmit,
may be reducible
No transillumination
Tumor
_ (
+ if
hemorrhagic)
Hard lump/ nodule
Generalized/
dependent
oedema
_
Diffuse swelling
Often post-operative or immobilized,
check for liver dysfunction