arrangement of teeth in complete denture
Dr.shanai m.Important differences between natural and artificial occlusion
Artificial teeth function as a group and occlusal loads are not individually managed.There is no feedback & the denture rests in centric relation. Any prematurity can shift the base.
Malocclusion pose immediate extreme problems.
Non vertical forces damage the supporting tissues.
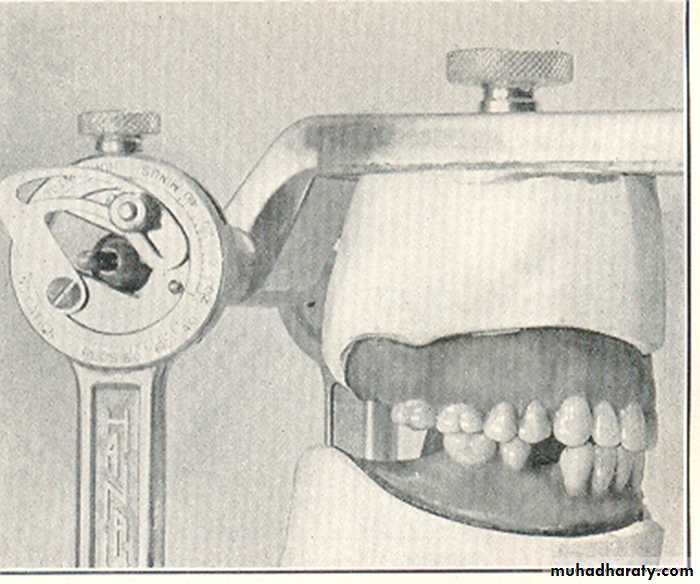
Bilateral balance is mandatory to produce stability of the denture.
Heavy pressure on the 2nd molar will tilt the base on inclined foundation
Natural teeth function independently and each tooth disperses the occlusal load.
Proprioceptive impulses from peridontium avoid the occlusal prematurities.Malocclusion can be nonproblematic for yrs.
Non vertical forces are well tolerated.
Bilateral balance is not necessary & usually considered a interference.
2nd molar favored for mastication owing to leverage & power.
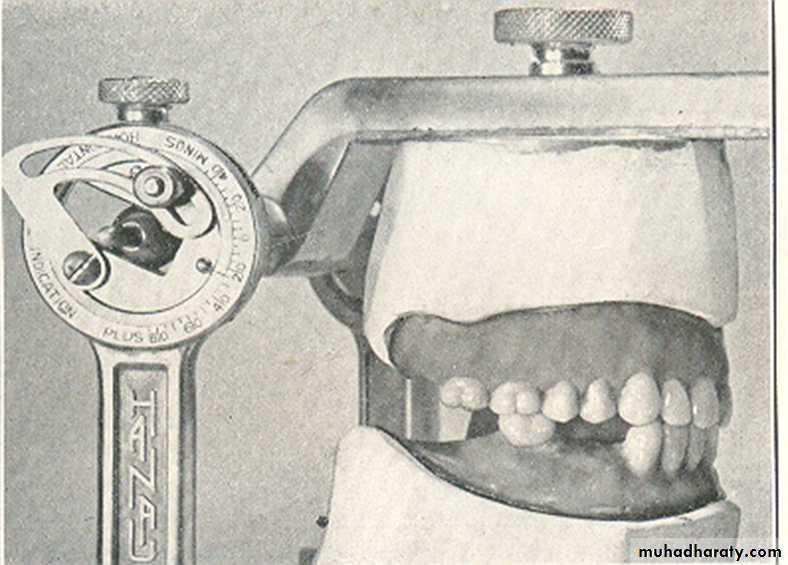
Prior to arrangement of the teeth, we must understand some of the definitions which is related to teeth arrangment 1. CONDYLAR GUIDANCE
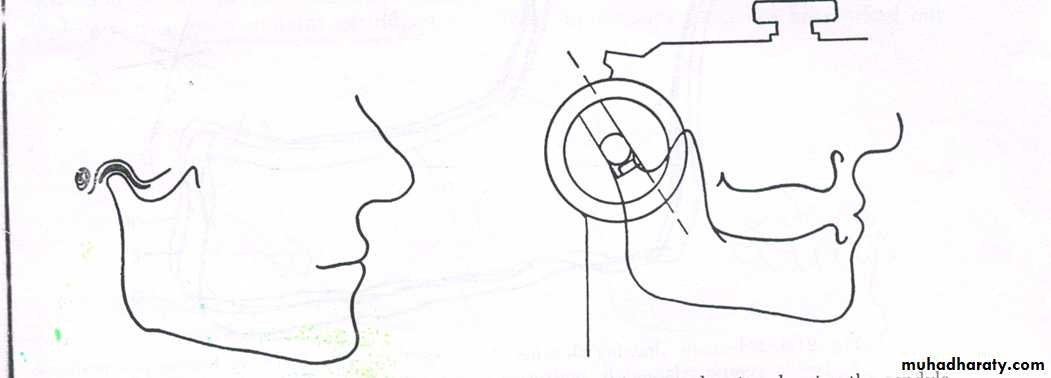
Mandibular guidance generated by condyle and articular disc traversing contour of glenoid fossa
Condylar guidance is due to path followed by condyle in temporomandibular joint
Obtained by protrusive registration record
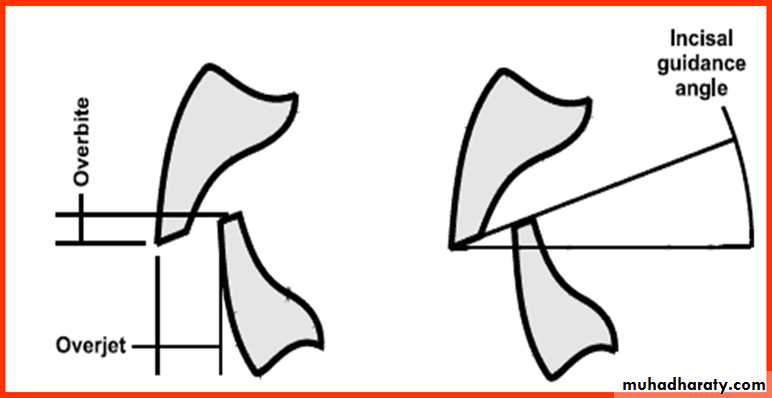
2. INCISAL GUIDANCEINCISAL GUIDE ANGLE: angle formed by intersection of plane of occlusion and line with in sagittal plane determined by incisal edges of maxillary& mandibular central incisors when teeth are in maximum intercuspation .
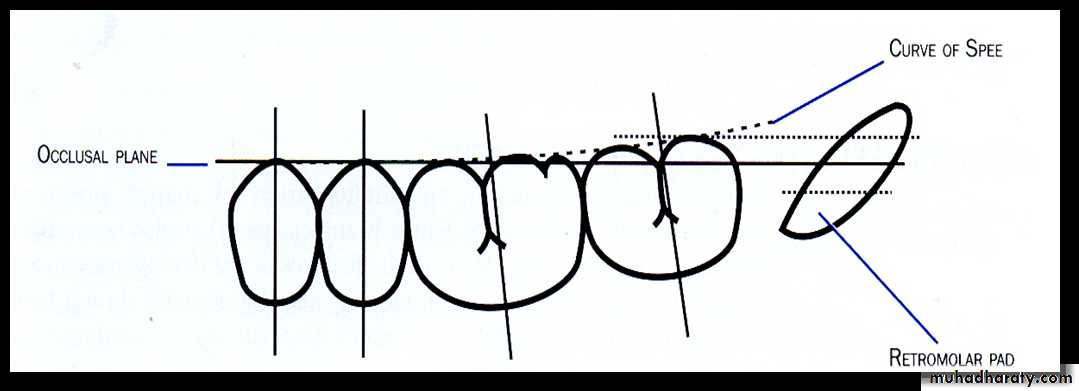
3.PLANE OF OCCLUSION OR OCCLUSAL PLANE
Defined as “An imaginary surface which is related anatomically to the cranium and which theoretically touches the incisal edges of the incisors & the tips of the occluding surfaces of posterior teeth.These landmarks also creates an occlusal plane essentially parallel to the ala-tragus line( Camper`s plane).
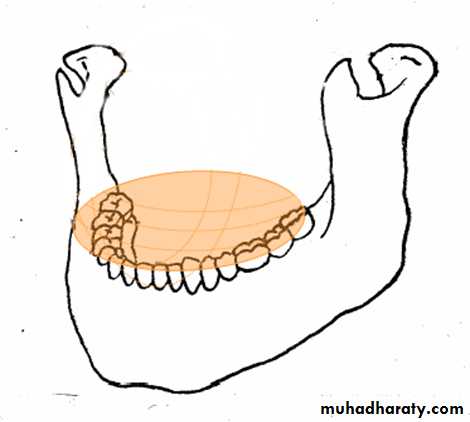
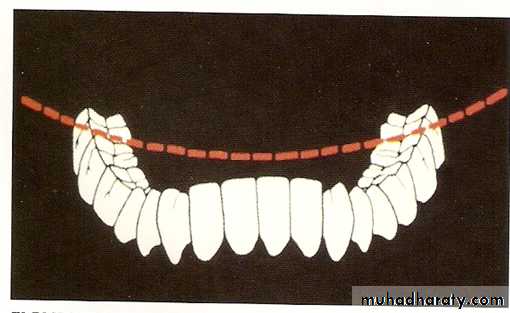
4.COMPENSATING CURVE
“The anterioposterior and lateral curvatures in the alignment of the occluding surfaces and incisal edges of artificial teeth which are used to develop balanced occlusion”.
Determined by inclination of posterior teeth and their vertical relationship to occlusal plane.
The primary function thus of compensating curve is to provide balancing contacts for protrusive mandibular movements. TYPES OF COMPENSATING CURVES
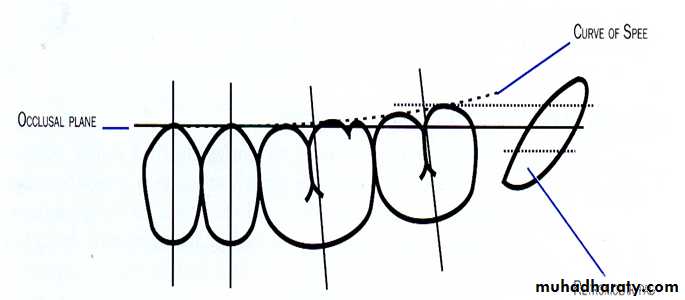
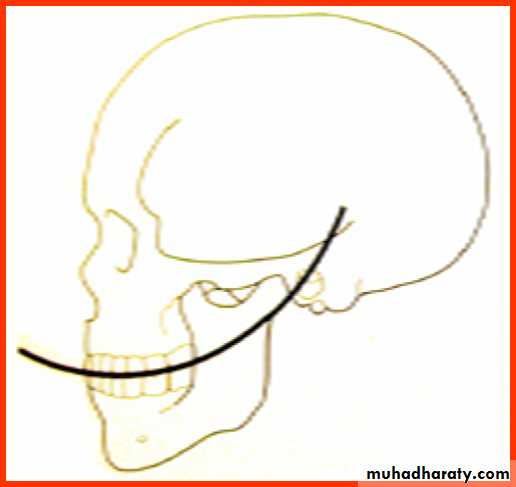
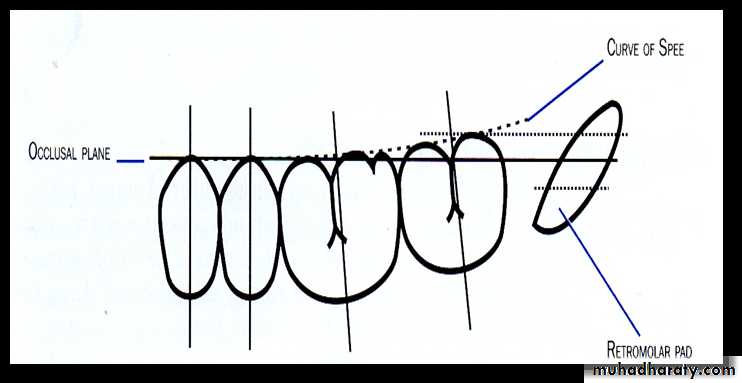
ANTERIOPOSTERIOR: ( Curve of spee )
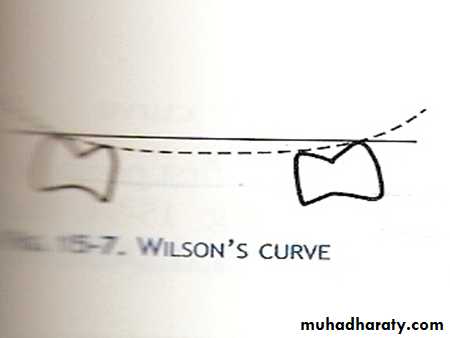
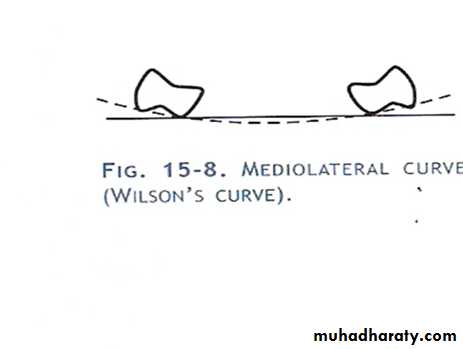
MEDIOLATERAL: (Wilson’s curve)
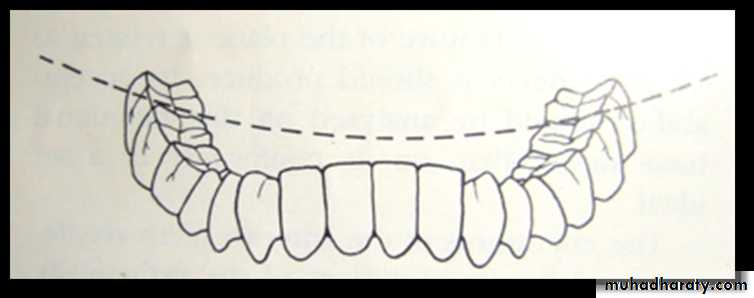
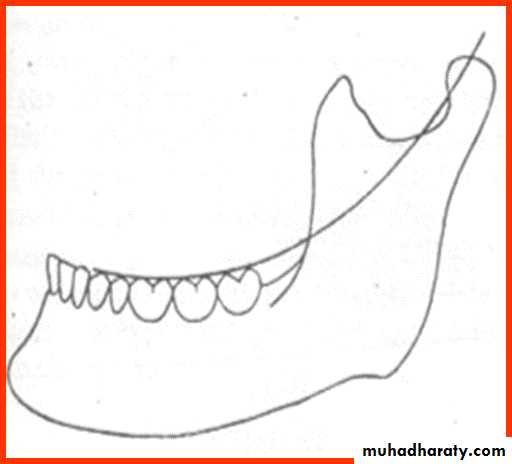
Curve of spee
beginning with the cusp tip of the mandibular canine and following the buccal cusp tips of the premolar and molar teeth, continuing through the anterior border of mandibular ramus, ending with the anterior most portion of the mandibular condyle.contacts buccal and lingual cusp tips of molars on each side of arch
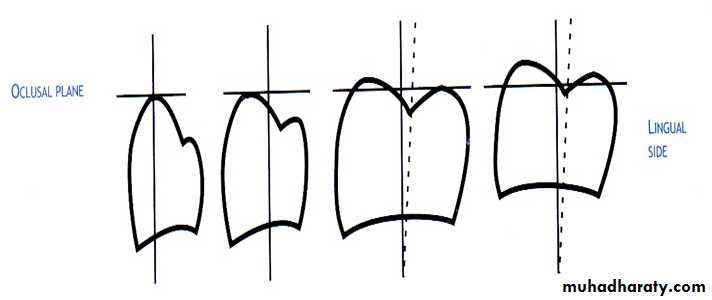
In mandibular arch -results from inward inclination of lowerposterior teeth-making lingual cusps lower than buccal cusps –curve being concave
In maxillary arch-results from outward inclination of posterior teeth-making buccal cusp higher than lingual cusps-curve being convex
Curve of wilson
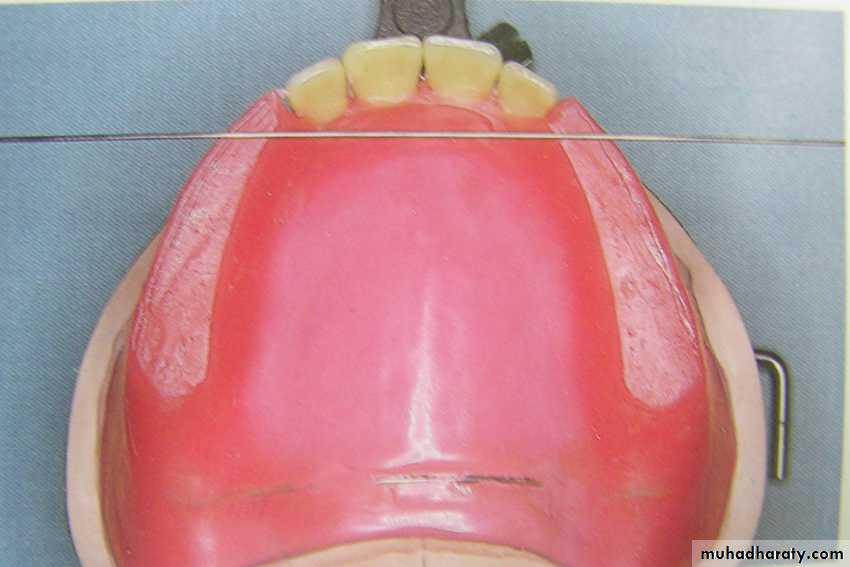
Guidelines for horizontal placement of anterior teeth
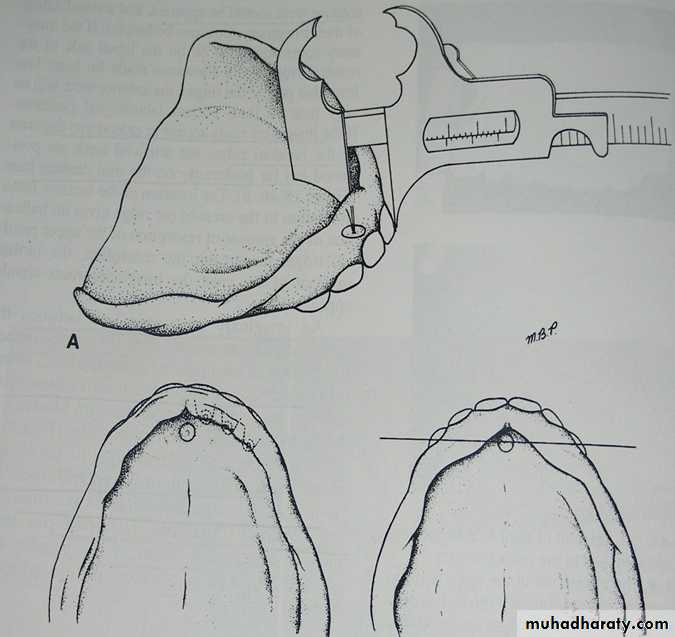
Role of incisive papilla & mid palatal sutureLabial surface of maxillary incisors is approx. 8 to 10 mm anterior to incisive papilla.
A transverse line bisecting the middle of I.P. passes through the tip of canine.
Cuspid eminences
When cuspid eminences are visible on cast, a line marking the distal of eminences coincide with distal margin of cuspids.
Relationship of lower lip to anterior teeth
Lower canine & Ist premolar should be even with lower lip at the corner of mouth.
Guideline to position posterior teeth
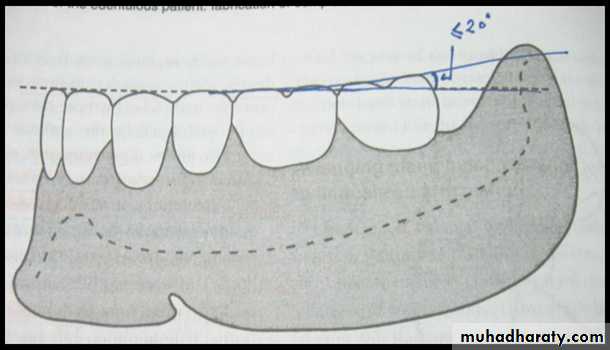
Retromolar pad
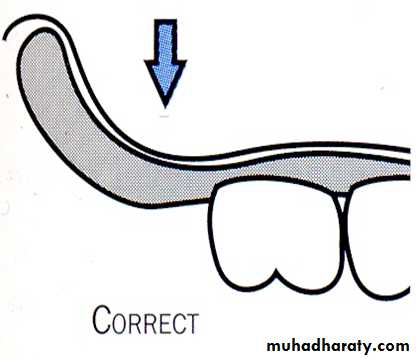
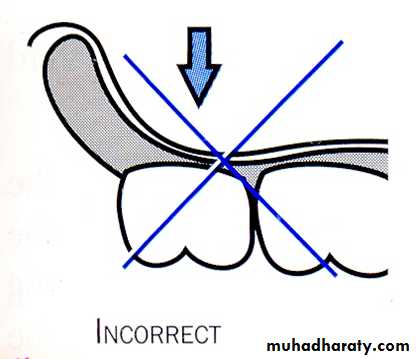
The maximum extension posteriorly of any artificial tooth is anterior border of Retromolar pad. to avoid having a tooth over an incline which results in denture sliding.
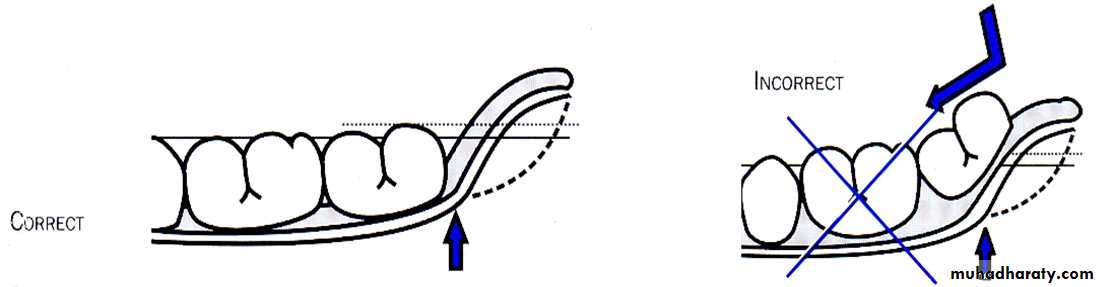
posterior occlusal plane should be at the level of 2/3 the height of retromolar pad
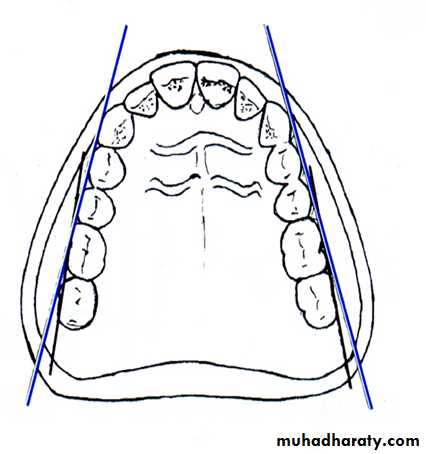
Maxillary Tuberosity
Teeth should not be set on the Tuberosity as it can lead to lever imbalance and might lead to cheek bite in posterior region.Relationship with tongue
Buccal Limit
Teeth should not be set too far off the ridge.
Placing too far Buccally can cause:
Cheek Biting
Esthetic problems due to obliteration of Buccal corridor.
Denture instability due to lever imbalance & muscle function.
Lingual Limit
Lingual cusps of molars are in alignment with Mylohyoid ridge.
Placing too far lingually can cause
Crowding of tongue.
Tongue biting.
Imbalance due to tongue function.
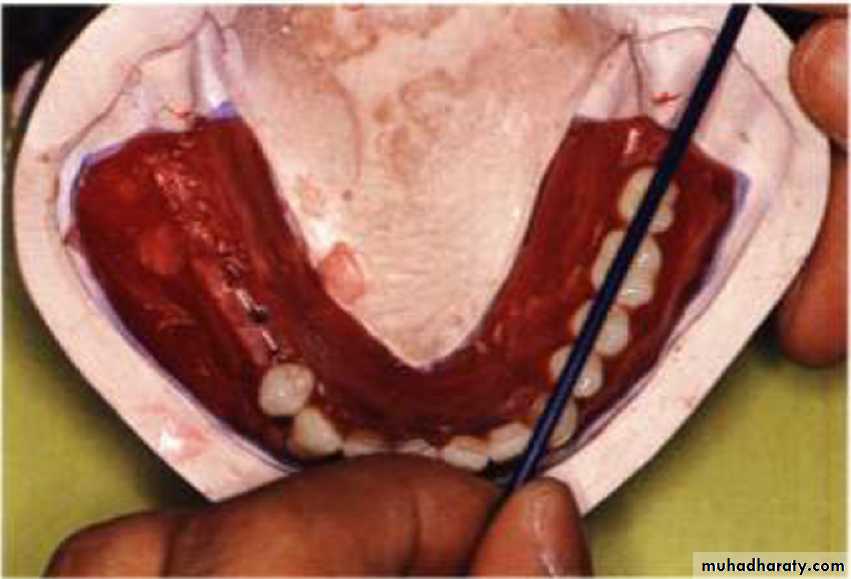
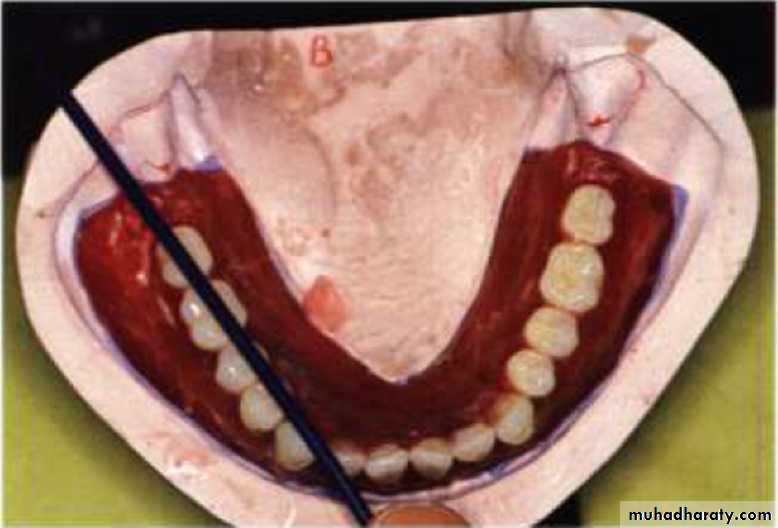
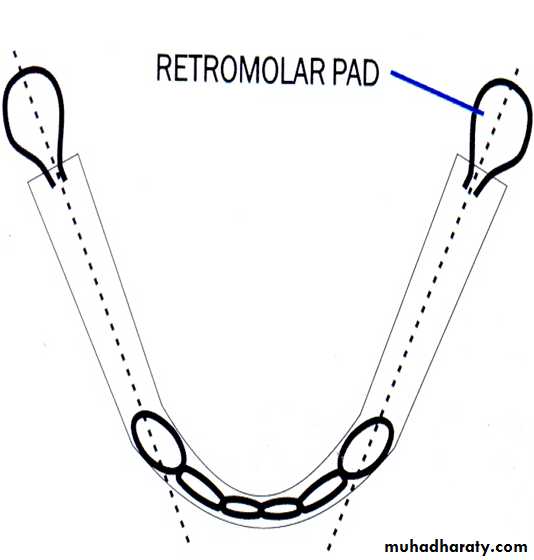
Canine-retromolar Pad Reference Line
From tip of Canine to center of Retromolar pad. This designates centre of mandibular Ridge.Central fossae of mandibular Posterior teeth should coincide with this line OR
This in turn corresponds to maxillary palatal cusps .
Individual orientation of maxillary teeth
Five important factors are involved in positioning anterior teeth. They are:1. Anterior slope - Labial inclination.
2. Mesiodistal inclination - Mesial or distal tilt.
3. Inferior-superior positioning to a horizontal plane - Above/below plane of occlusion.
4. Rotation on a long axis - Turning tooth on its center axis.
5. Antero-posterior positioning - How far labially or lingually (in or out) the an
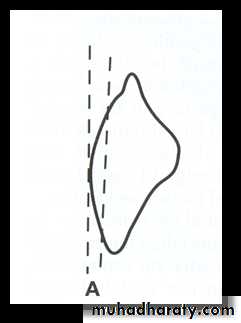
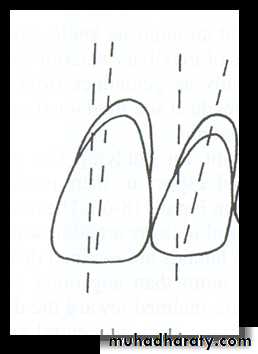
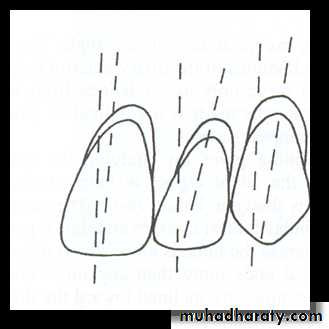
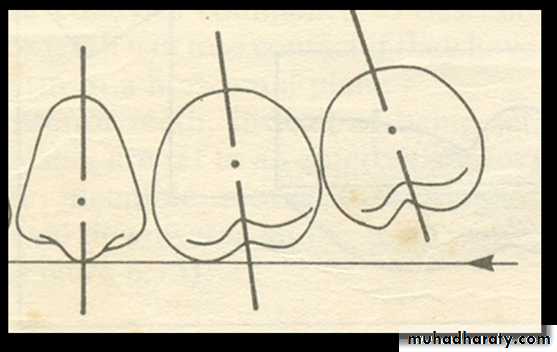
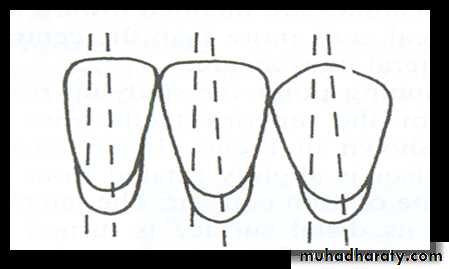
Maxillary Central Incisor technique:
The long axis of the tooth is perpendicular to the horizontal
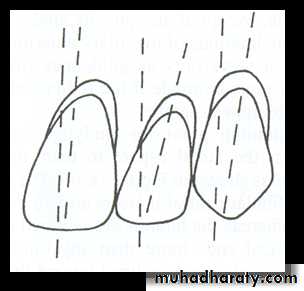
mesiodistal inclination
The maxillary central incisor is placed, so that the long axis shows a slight distal inclination, when viewed from front.
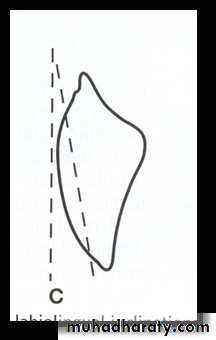
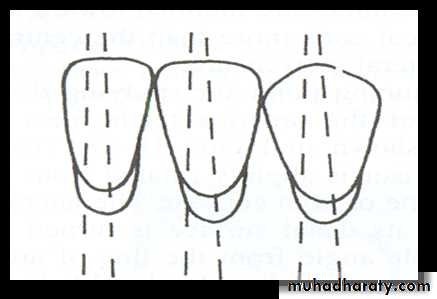
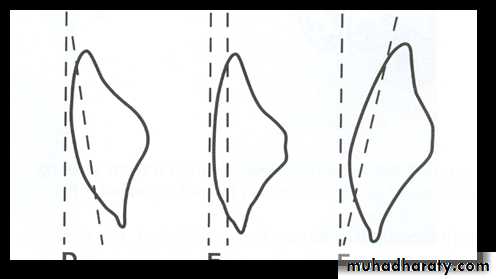
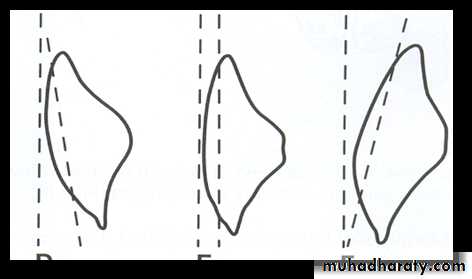
Labio-lingual inclination:
The neck of the tooth should be slightly depressed when viewed from this side, the tooth slopes (incisal edge ) towards the labial side.
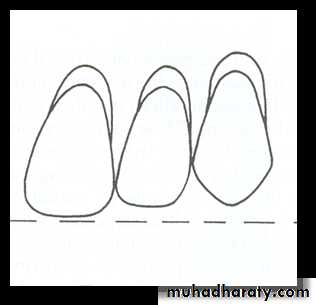
The incisal edge:
Is in contact with the occlusal plane.

Teeth is set on the occlusal rim
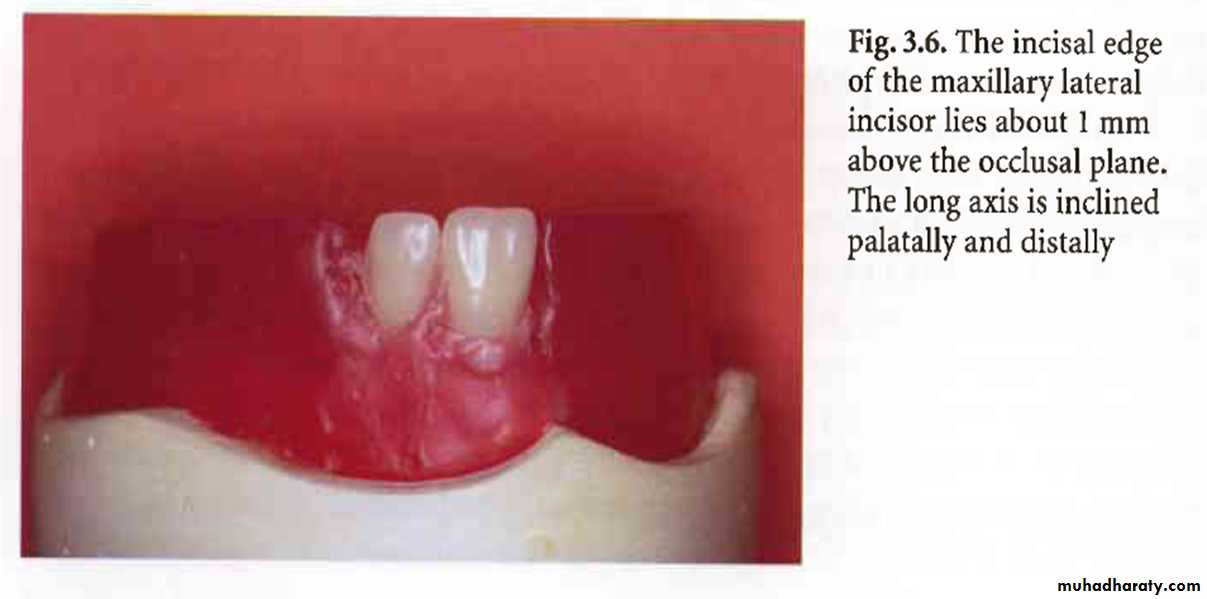
Maxillary Lateral Incisor:Mesio-distal inclination:
The maxillary lateral incisor is placed with its long axis inclined notes able distally when viewed from the front.
Labio-lingual inclination:
The neck of the maxillary lateral incisor is depressed (of the neck) more than the central incisor, although the labial surface will be nearly in line with the central incisor.
The incisal edge:
is ½ to 1mm above the level of the occlusal plane.
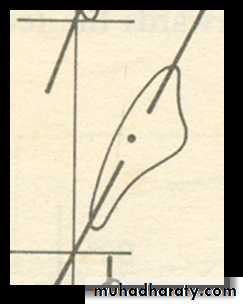
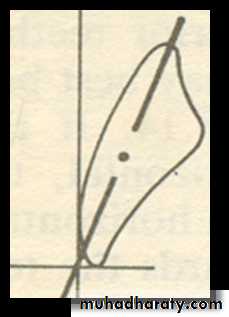
Maxillary Canine :
• Mesio-distal inclination:• The maxillary canine is placed so that the long axis has slight distal inclination from the front view.
• Labio-lingual inclination:
• The neck of the maxillary canine is prominent. The tooth axis is vertical (straight ) when viewed from the side.
The cusp tip:
• Is in contact with the occlusal plane.
• The maxillary canine has two planes on the labial surface;
• mesial plane should follow the contour of the anterior teeth
• while the distal plane will be in line with the posterior teeth.
•



First premolar:
Long axis is parallel to the vertical axis when viewed from the front or the side.Its palatal cusp is about 1mm short of, and its buccal cusp in contact with, the occlusal plane.
Second premolar:
Its long axis is parallel with the vertical axis when viewed from the front or the side.Both buccal and palatal cusps are in contact with the
occlusal plane.
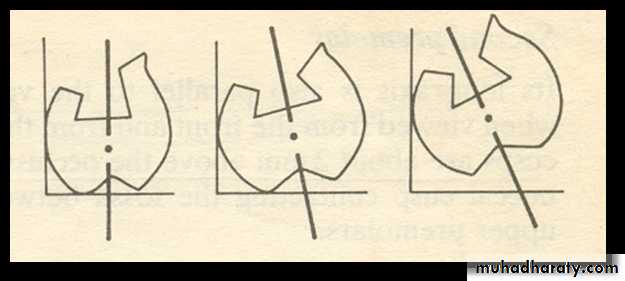
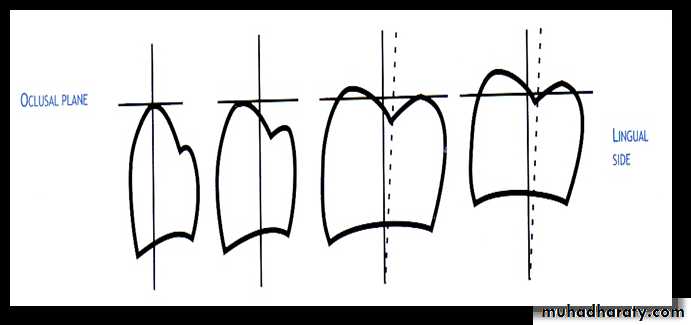
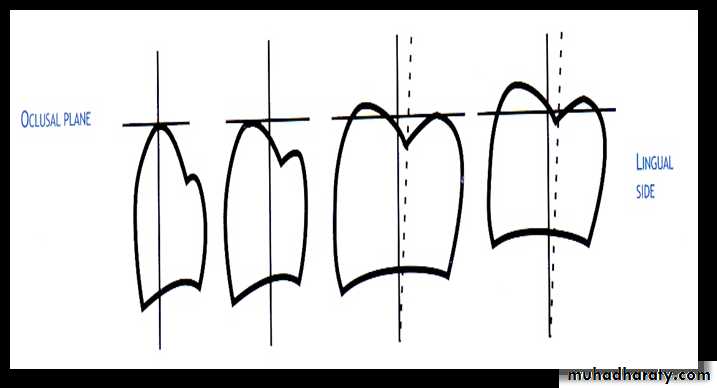
First molar:
Long axis slopes buccally when viewed from the front, and distally when viewed from the side.
Only mesiopalatal cusp is in contact with the occlusal plane.
Second molar:
Long axis slopes buccally more steeply than the first molar when viewed from the front, and distally more steeply when viewed from the side.
All four cusps are clear of the occlusal plane, but the mesiopalatal cusp is nearest to it.
Orientation and arrangement of mandibular teeth
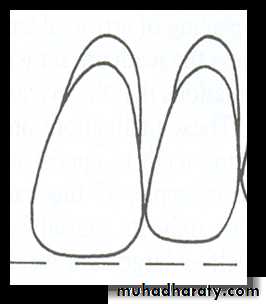
Mandibular central incisor:Mesio-distal inclination:
The long axis is perpendicular to the occlusal plane (vertically upright).
Labio-lingual inclination:
The central incisor is placed with its neck depressed and the tooth will show that it’s labially inclined when viewed from one side.
The incisal edge:
Are 1-2 mm above the occlusal plane.
Position of the mandibular lateral incisor:
Mesio-distal inclination:
The mandibular lateral incisor is placed with its long axis showing a slight distal inclination.
Labio-lingual inclination:
The labial surface is perpendicular to the occlusal plane.
The incisal edge:
Are 1-2 mm above the occlusal plane.
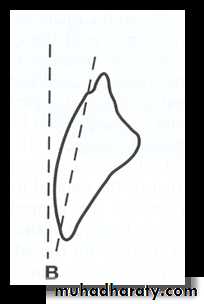
Position of the mandibular canine:
Mesio-distal inclination:The mandibular canines are placed with a more distal inclination (neck distally placed) than the mandibular lateral incisors.
Labio-lingual inclination:
The neck of the tooth is placed prominently. The tooth shows a slight lingual inclination (at the incisal edge) when viewed from the side
The incisal tip:
Lies 1-2 mm above the occlusal plane
Horizontal overlap (over jet):
This the horizontal distance between the incisal edge of the maxillary central incisor and the labial surface of the mandibular central incisor.
Vertical overlap (over bite):
The maxillary anterior teeth overlap the mandibular anterior teeth and this overlap on the vertical axis is called the vertical overlap.
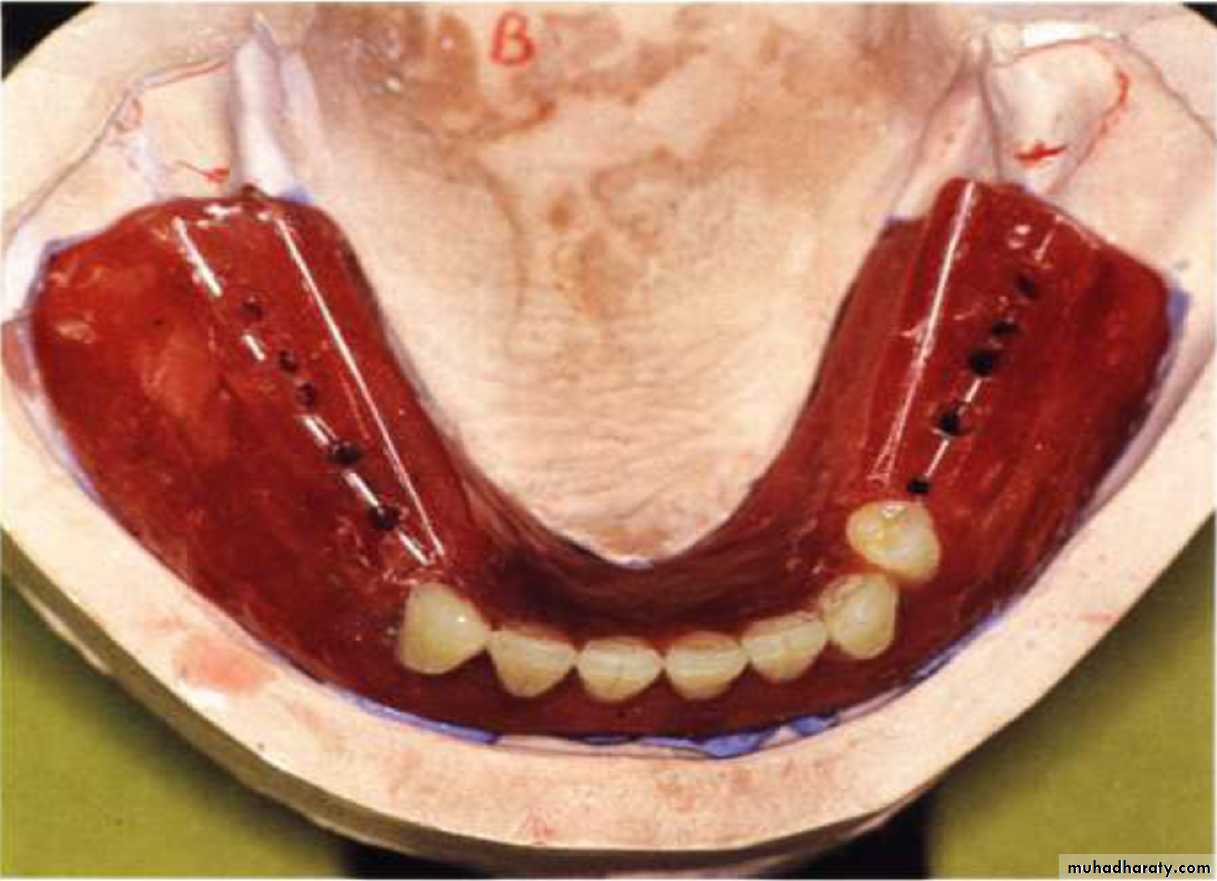
The retromolar pad is exposed and points are marked on pounds lines
joining the cannine to retromolar pad.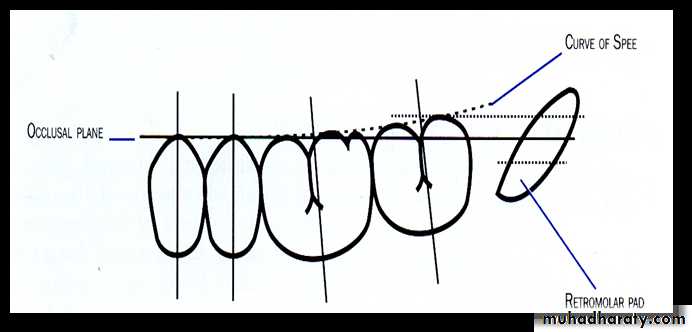
Mandibular 1st Molar
Facial: Long axis rests mesially, when viewed from side.Proximal : Long axis inclines Lingually, when viewed from front.
Occlusal: Buccal cusps are higher than Lingual cusps. Distal cusps are higher than Mesial cusps.
Second premolar:
Long axis is parallel to the vertical plane when viewed from both the front and the side.
Both cusps are about 2mm above the occlusal plane.
The buccal cusp contacts the fossa between the two upper premolars.Mandibular 2ed Premolar
Facial & Proximal : Long axis is vertical from both views.
Occlusal : Both cusps are about 1-2mm above Occlusal plane
Mandibular Ist Premolar
Facial : Long axis is parallel to vertical plane.Proximal : Long axis is parallel to vertical plane.
Occlusal : Bu cusp is above the occlusal plane, whereas Li cusp is below occlusal plane.
Mandibular 2nd Molar
Facial : Mesial inclination is more than 1st molar.Proximal : Lingual inclination is slightly more than 1st molar.
Occlusal : Buccal cusps are higher than Lingual. Distal cusps are higher than Mesial.