1
Lec.2
Pediatrics
6
th
stage
2016/8/9
Tutorial
د.دمحم خضر
Acute respiratory infection
CLASSIFICATION
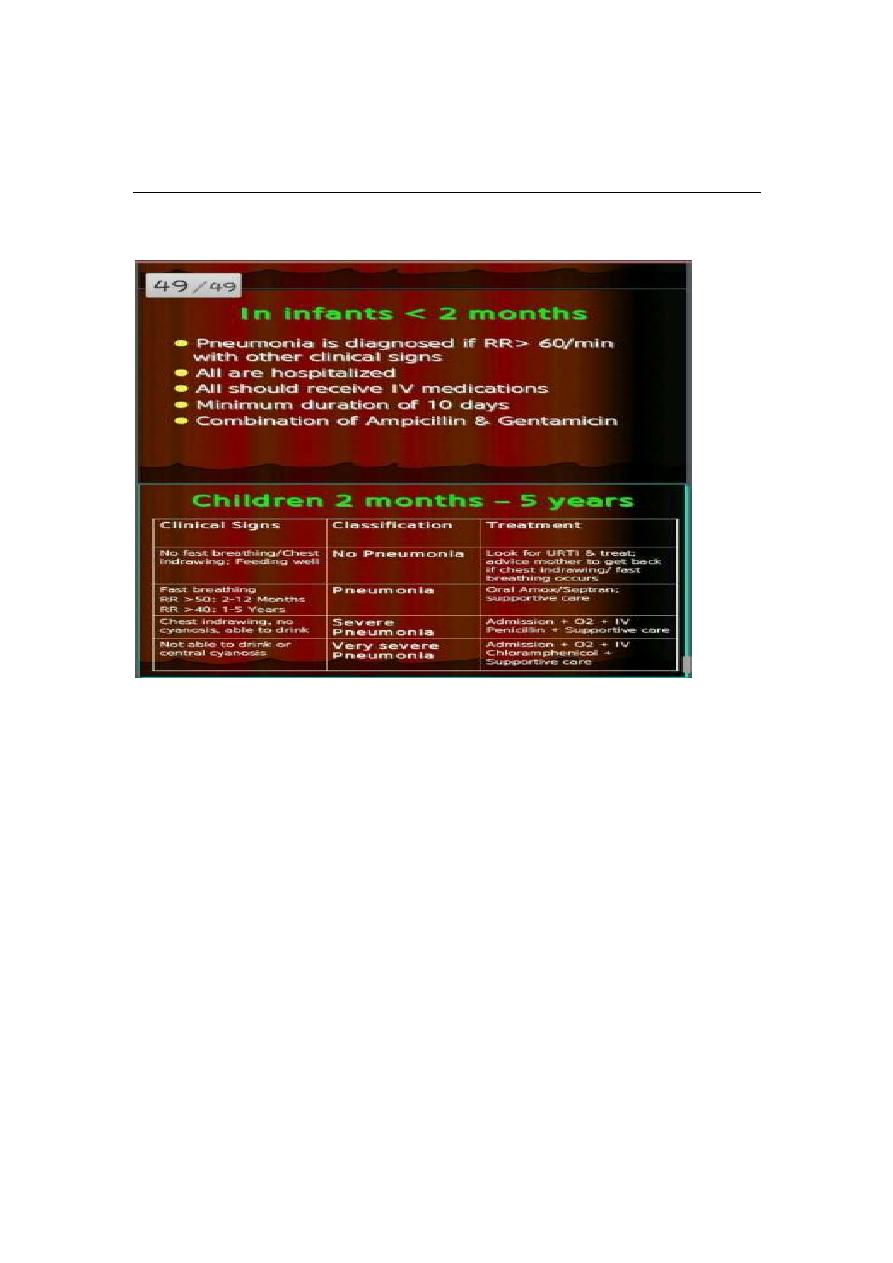
CHILD AGED 2 MONTHS TO 5 YEARS
Classifying the illness means making decisions about the type and
severity of disease. The sick child should be put into one of the four
classifications:
VERY SEVERE DISEASE
SEVERE PNEUMONIA
PNEUMONIA(not severe)
NO PNEUMONIA
VERY SEVERE DISEASE
The danger signs and possible causes are:
2
a) Not able to drink: A child who is not able to drink could have severe
pneumonia or bronchiolotis, septicaemia, throat abscess, meningitis or
cerebral malaria.
b) Convulsions, abnormally sleepy or difficult to wake: A child with these
signs may have severe pneumonia resulting in hypoxia, sepsis, cerebral
malaria or meningitis. Meningitis can develop as a complication of
pneumonia or it can occur on its own.
c) Stridor in calm child: If a child has stridor when calm, the child may
be in danger of life threatening obstruction of the air-way from swelling
of larynx, trachea or epiglottis.
d) Severe malnutrition: A severely malnourished child is at high risk of
developing and dying from pneumonia. In addition, the child may not
show typical signs of the illness.
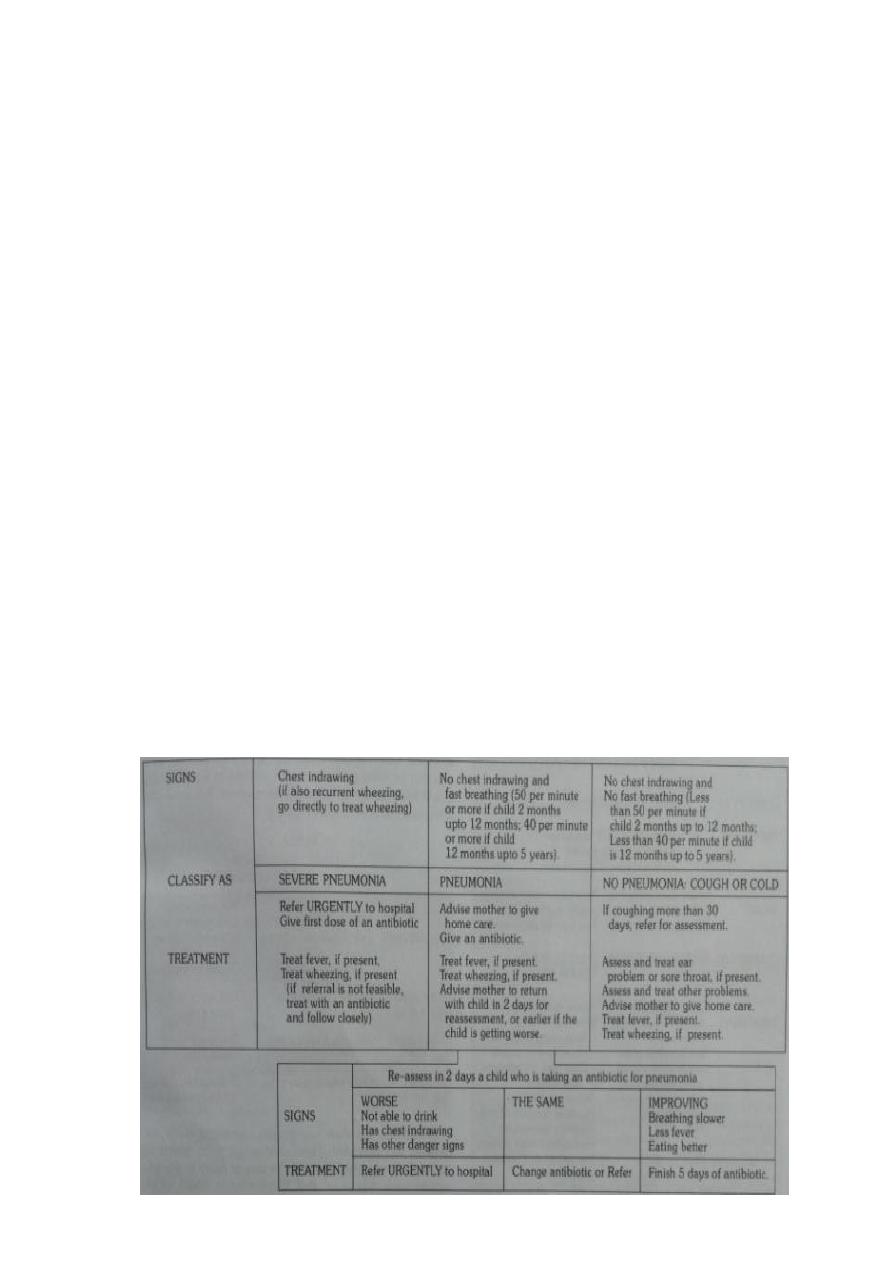
. SEVERE PNEUMONIA
2
The most important signs to consider when deciding if the child has
pneumonia are the child’s respiratory rate, and whether or not there is
chest indrawing may not have fast breathing if the child becomes
exhausted, and if the efforts needed to expand the lungs is too great.
In such cases , chest indrawing maybe the only sign in a child with
severe pneumonia. A child with chest indrawing is at higher risk of
pneumonia than a child with fast breathing alone.
A child classified as having severe pneumonia also has other signs such
as;
. Nasal flaring, when the nose widens as the child breaths in
. Grunting, the short sounds made with the voice when the child has
difficulty in breathing and
. Cyanosis, a dark bluish or purplish coloration of the skin caused by
hypoxia
3
Children who have chest indrawing and a first episode of wheezing often
have severe pneumonia, however with recurrent wheezing do not have
severe pnuemonia.
3. Pneumonia (not severe)
A child who has fast breathing and no chest indrawing is classified as
having pneumonia(not severe). Most children are classified in this
category if they are brought early for treatment. Fever , cough,
tachpnoea, crackles , signs of consolidation , and constitutional
symptoms are the general clinical features seen in a patient suffering
with pneumonia.
4. No pneumonia: cough or cold
Most children with a cough or difficult breathing do not have any danger
signs or signs of pneumonia ( chest indrawing or fast breathing). These
children have a simple cough or cold. They are classified as having ‘no
pneumonia: cough or cold’. They do not need any antibiotic. Majority of
such cases are viral infections where antibiotics are not effective.
Normally a child with cold will get better within 1-2 weeks.
MANAGEMENT OF PNEUMONIA IN A CHILD AGED 2 MONTHS UPTO 5
YEARS

4
Classifying illness of young infant
Infants less than 2 months of age are referred to as young infants. They
have special characteristics that must be considered when their illness is
classified. They can become sick and die very quickly from bacterial
infections, are much less likely to cough with pneumonia, and frequently
have only non specific signs such as poor feeding, fever or hypothermia.
1) Further mild chest indrawing is normal in young infants because their
chest wall bones are soft. The presence of these characteristics means
that they will be classified and treated differently from older children.
2) Many of the cases may have added risk factor of low birth weight.
Such children are very susceptible to temperature changes and even in
tropical climates, death due to cold stress or hypothermia are common.
3) In young infants the cut off point for fast breathing is 60 breaths per
minute. Any pneumonia in young infants is considered to be severe.

5
CLASSIFICATION AND MANAGEMENT OF ILLNESS IN YOUNG INFANTS
Treatment
A. TREATMENT FOR CHILDREN AGED 2 MONTHS UPTO 5 YEARS
.PNEUMONIA (child with cough and fast breathing)
cotrimoxazole is the drug of choice for the treatment of pneumonia.
Cure rates are 95%. It is less expensive with few side effects and can be
used safely by health workers at the peripheral health facilities and at
home by the mothers.

6
The condition of the child should be assessed after 48 hours.
Cotrimoxazole should be continued for another 3 days in children
who show improvement in clinical condition.
If there is no improvement in the condition then it should be
continued for 48 hours and then reassesed.
If at 48 hours or earlier the condition worsens, the child should be
hospitalised immediately.
Severe pneumonia (chest indrawing)
Children with severe pneumonia should be treated as inpatients with
intramuscular injections of benzylpenicilline(after test dose) ampicillin or
chloramphenicol.
The condition of the child must be monitored everyday and reviewed
after 48hrs for antibiotic therapy.
Antibiotic therapy must be given for a minimum of 5 days and continued
for atleast 3 days after the child gets well.
Very severe disease
-Children with signs of very severe disease are in imminent danger of
death and should be treated in a health facility, with provision of oxygen
therapy and intensive monitoring.

7
-Chloramphenicol IM is the doc in all such cases. Treat for 48 hrs ,if
conditons improve switch over to oral chloramphenicol. It should be
given for a total of 10 days.
-If condition worsens or does not improve after 48hrs switch to IM
injections of cloxacillin and gentamicin.
B. PNEUMONIA IN YOUNG INFANTS UNDER 2 MONTHS OF AGE
The treatment in these condition is basically the same.
1.The child must be hospitaised.
2.Treatment with cotrimoxazole maybe started by the health worker
before referring the child.
3. If pneumonia is suspected in the child should be treated with IM
injection of bezylpenicilline or ampicillin, along with injection
gentamycin.
Besides antibiotics, therapy for the associated conditions if any,
must be instituted immediately. The child must be kept warm and
dry. Breast feeding must be promoted strongly as the child who is
not breast fed is at a much higher risk of diarrhoea.
Management of AURI (no pneumonia)
-> Many children with presenting symptoms of cough, cold and fever do
not have pnenumonia and do not require treatment with antibiotics.
->They are not recommended as majority of cases are caused by viruses
and antibiotics are not effective, they increase resistant strains and
cause side effects while providing no clinical benefit, and are wasteful
expenditure.
->Symptomatic treatment and care at home is generally enough for such
cases.