



بسم الله الرحمن الرحيم

• Orthognathic surgery

• Introduction
• The term orthognathic originates from the words orthos and gnathos (Gr. orthos = straight; gnathos = jaw). Orthognathic surgery refers to surgical procedures designed to correct jaw deformities. Orthognathic procedures are divided into three categories: maxillary surgery, mandibular surgery, and bimaxillary procedures.• Indications
• In patients with susceptibility to caries and periodontal disease. This may be due to difficulty in maintaining oral hygiene because of severely protruding and irregular teeth.• One indication is also the unaesthetic appearance of a dentofacial deformity resulting in undesirable psychosocial effects.
• Correction of post traumatic facial deformity , post traumatic malocclusion.
• Correction of facial deformity in crainoifacial syndromes with or without distraction osteogenesis.
• As combined work to gain access in certain type of tumor surgery.
• Improve esthetic and phonetic
• contraindications
• Numerous risk factors may alter the treatment plan or preclude surgery, including underlying medical conditions,• bleeding dyscrasias.
• systemic disease .
• local factors that may affect normal wound healing
• compromised vascularity of the surgical region,
• a patient with unrealistic expectations,
• a noncompliant patient, and patients with poor oral hygiene.
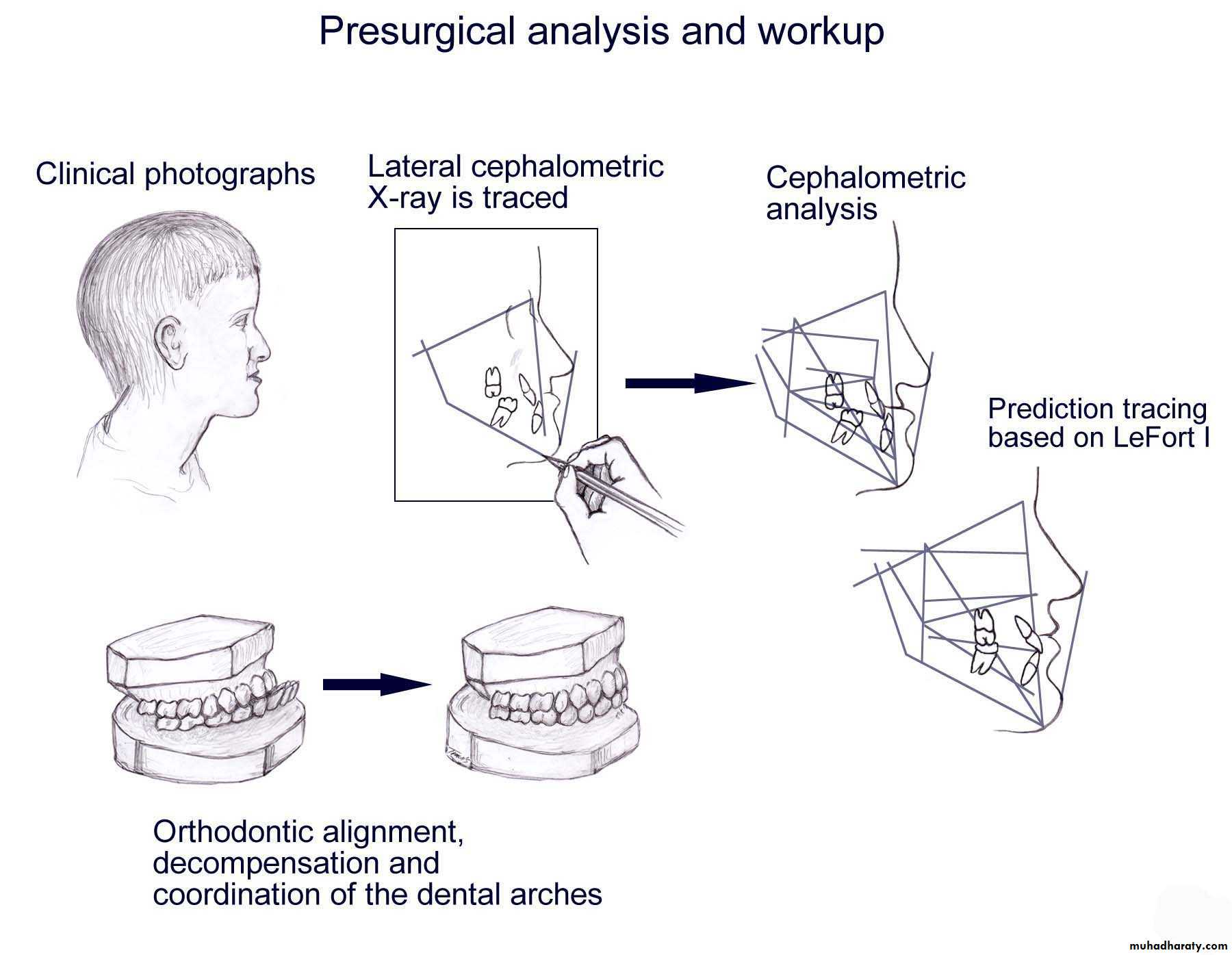
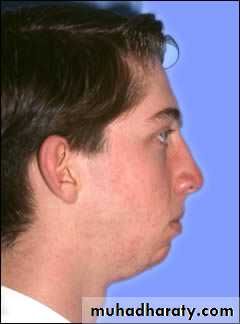
• workup
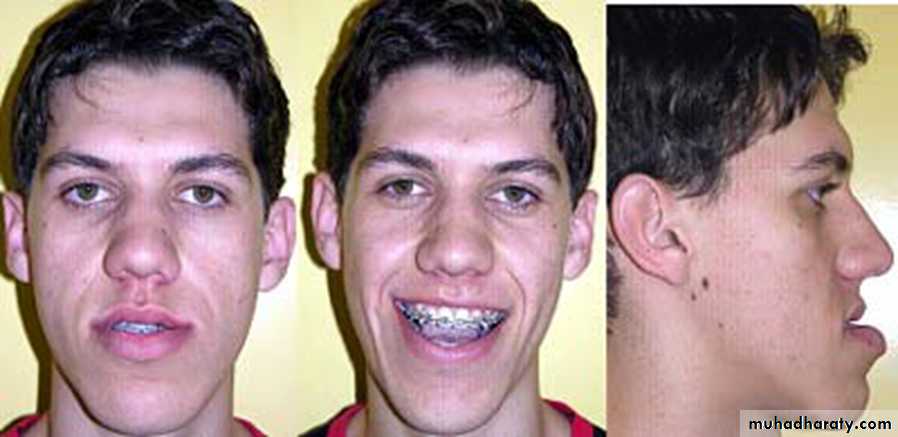
• Clinical examination (dental occlusion. Skeletal relation and evaluation, soft tissue analysis) and this is can be accomplished by• Photograph.
• Standerized radiograph (frontal and lateral cephalometric, panoramic view, periapical and occlusal view, 3D cone beam tomography, digital radiograph and computer analysis and prediction.
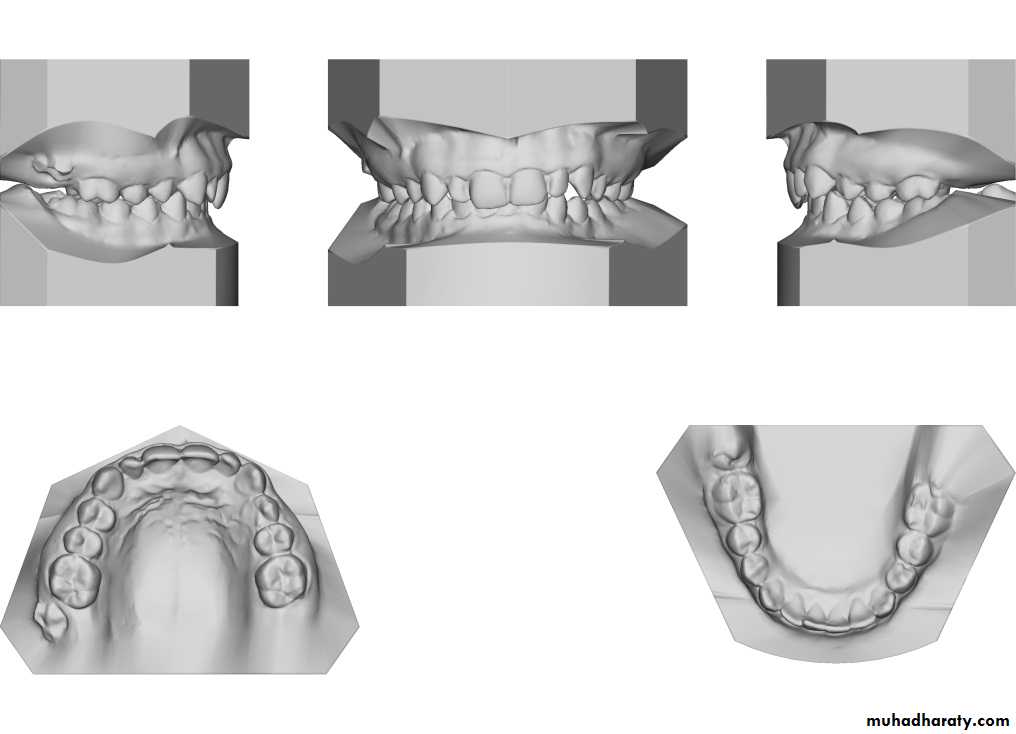
• Study dental cast.
• Team work by orthodontist, restorative and periodontologist and prosthodontist.
High precision 3D surface image registered withCBCT data
Anatomical landmarks on 3D skull model and 3Dcephalometric analysis• workup
• Angle’s classification of the occlusion
• Registration of over bite and over jet
• Recording the centric relation and centric occlusion.
• Imaging study
• Clinical photographs are essential for documentation and to allow for photometric analysis.• Images with the lips at repose and during animation (smiling) are obtained; the degree of dental display is noted for each.
• Cephalometric x-rays provide for standardized skull and/or facial views that allow for comparison over time to assess growth in an individual and for comparison of that individual against standardized population norms. Skeletal views can be obtained in lateral and frontal views.
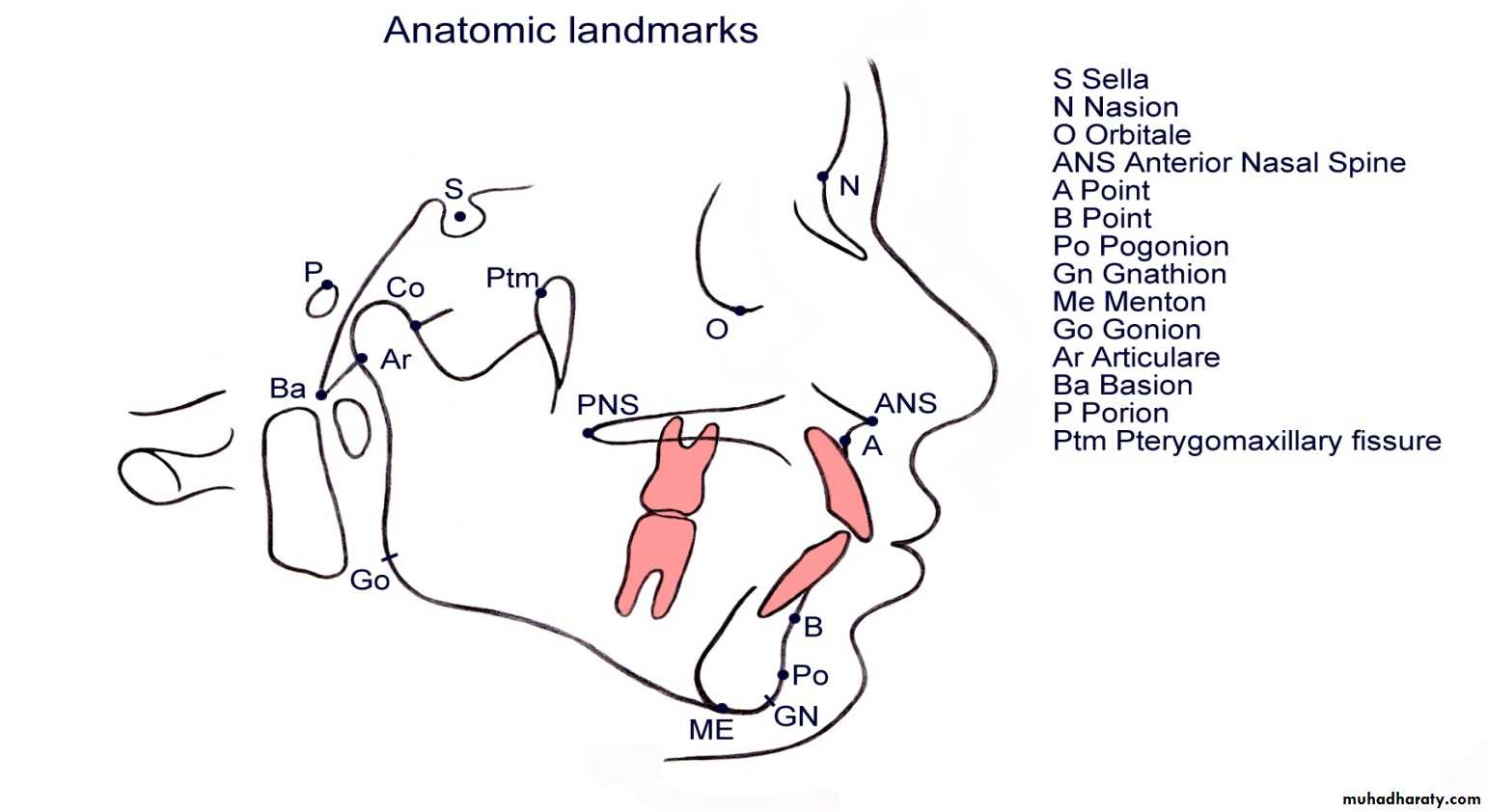
Lateral cephalometric landmarks
Lateral cephalometric x-ray also allows the dentition to be related to each other, and each can be related to its own skeletal base, the maxilla, and the mandible.
Frontal cephalometric x-ray allows for assessment of the degree of facial asymmetry.
Periapical films are obtained to determine if sufficient space exists for interdental osteotomies.
For the surgeon, the analysis must be clinically workable, simple to use, and directly relatable to the skeletal elements that can be repositioned.
Additional radiographs include the following
• Three-dimensional computerized tomography (3DCT) is increasingly being used for surgical evaluation and planning .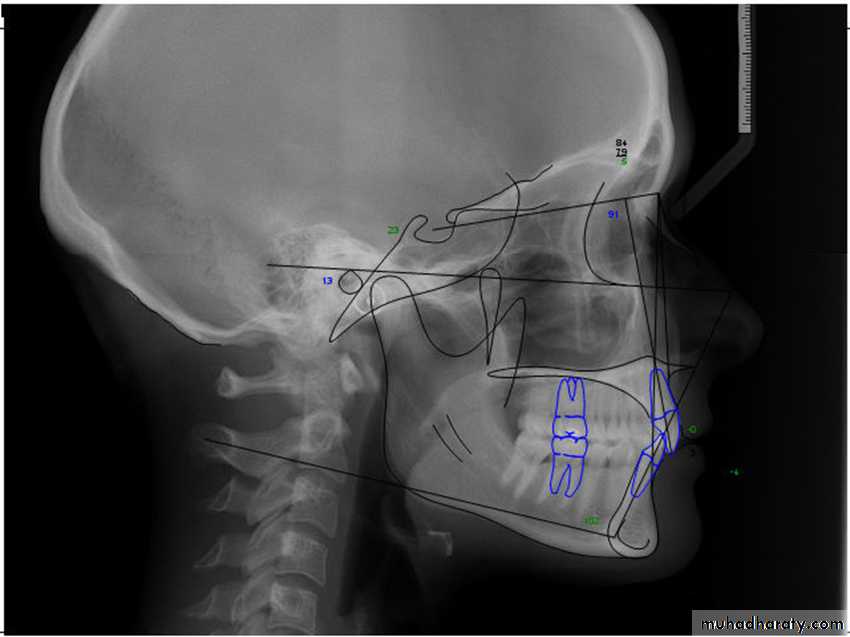

Dental cast
Surgical movement of maxilla and mandible inherently alter the maxillary-mandibular dental occlusion, and as such, careful analysis of the dental models with the orthodontist is essential. The maxillary dental and mandibular dental casts can be studied individually and hand manipulated with each other to assess how the arches are coordinated.Assessment of the models includes space analysis and arch length, transverse width discrepancies, position of the individual tooth within its own arch, and the relationship of the maxillary dentition to the mandibular dentition.
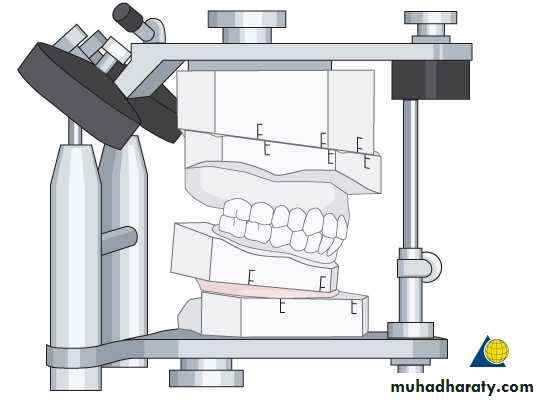


• The surgeon makes osteotomies (ie, incisions) between the teeth in the plaster maxillary cast to create a precise occlusal fit.

• The surgeon then performs the planned surgical procedure on plaster models of the patient’s jaws and teeth and uses these models for reference during the actual surgery.
• The surgeon makes a plastic transitional splint or jig on the model and uses in surgery to position the mandible according to the maxillary position or to position the maxilla based on the position of the mandible
• The jaw may be reshaped on the model until the proper position is obtained.
The management can then be divided into the following 5 phases:
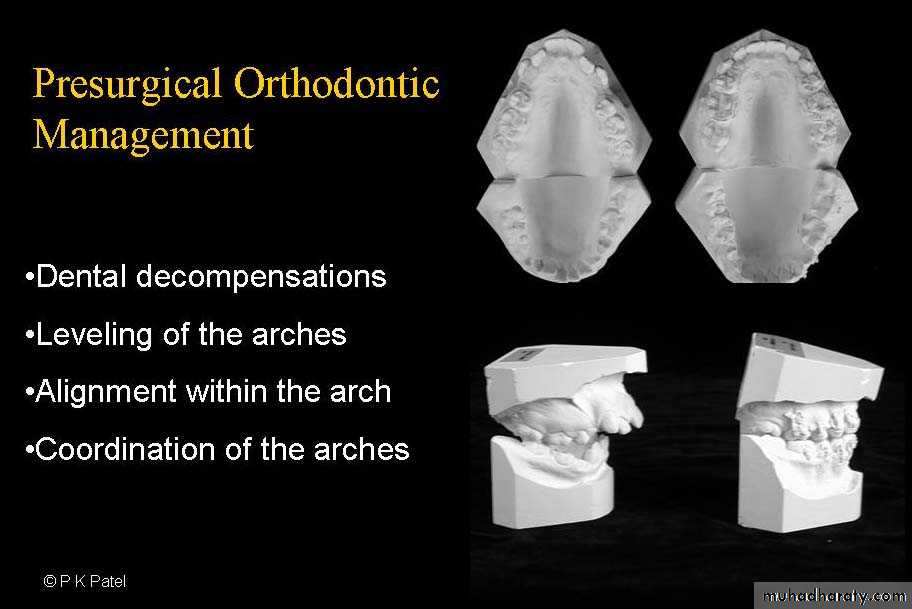
Preorthodontic preparatory phasePresurgical orthodontic treatment phase
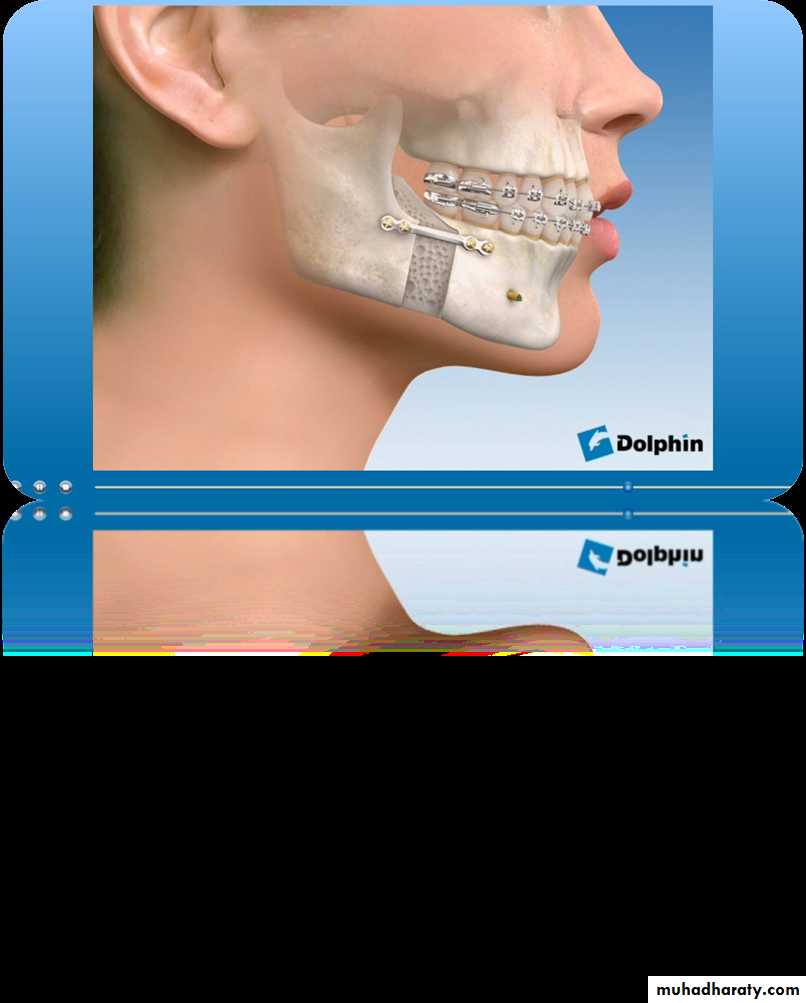
Surgical phase
Postsurgical orthodontic phase
Prosthodontic treatment phase
Principles of surgical treatment
Strict adherence to the surgical principles is inevitable requisites for success of surgery.Psychological evaluation of the patient.
It is essential that the patient and the relatives be informed about the postoperative results as well as the problems involved during postoperative recovery period.
They should be aware of the difficulties in normal activities in the 4-6 weeks postoperatively.
The diet may not be normal( soft liquid diet).
Maintenance of good oral hygiene.
Postoperative swelling and pain should be discussed with the patient.
Occlusal disturbance associated with surgery should be briefed on.
Patient who has been briefed and prepared psychologically turns out to very cooperative patient.
Most patient can resort to their routine activities by the second week of surgery.
Maintenance of blood supply
It is important to maintain of good blood supply to the mobilized segments and this is achieved by maintaining proper soft tissue pedicles to the osteotomized segment.It is not advisable to segment a single jaw in to more than 4 segments because multiple segmentation reduce the blood supply.
Keep minimal stripping of the muscles overlying the bones as blood supply enter through the muscle insertion.
Care of the nerve, vessels, teeth and bones
Facial, inferior alveolar, mental, inferior orbital nerve should be protected during surgery.
Vascular supply of the teeth should be maintained by making the osteotomy at about 3 to 5 mm away from the apices of the teeth.
Alveolar crest and periodontium should be preserved as if this structures violated during surgery may result in deep pocket and tooth ankylosis.
Copious irrigation by saline to minimize thermal damage.
Whenever a bone defect is created, a bone graft is inserted and placed.
Good immobilization and fixation is necessary to prevent fibrous union and mal union or non union of the osteotomized segments.
Post surgical period
Balance of fluids intake and output.Control of infection, pain and edema.
Maintenance good oral hygiene.
Early ambulation is advised and the patient should encouraged to early movement to reduce the chance of pulmonary problems and the patient regain energy faster.
Good nutrition is essential to promote wound healing.
Surgical approaches
Trans oral approaches to the maxillary lefort 1 osteotomy
Trans oral approach to the mandible ramus
(sagittal split osteotomy)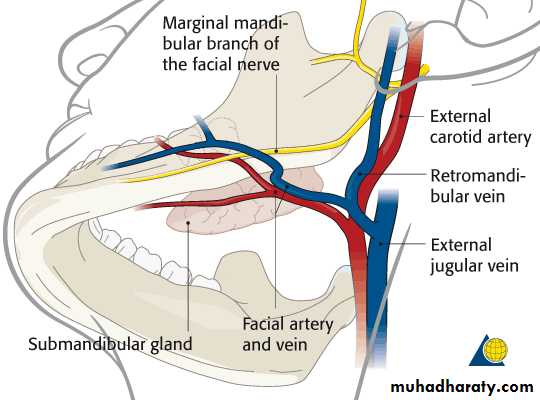
Extra oral submandibular approaches to the mandible
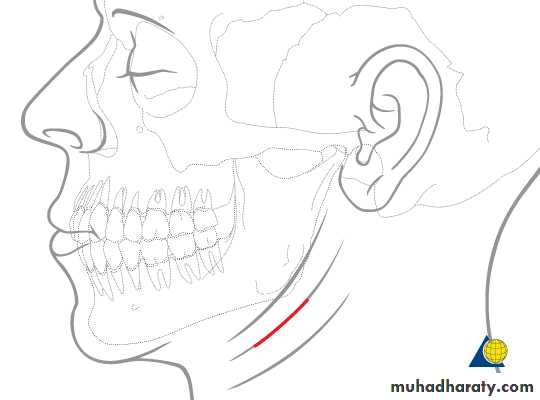
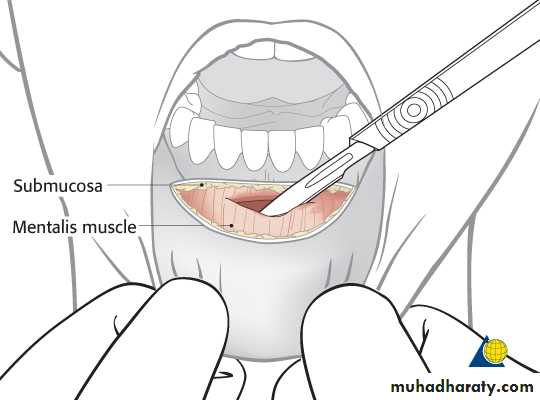
Trans oral approach to the chin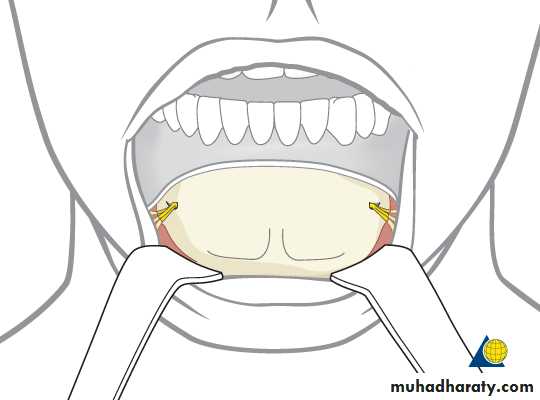
Corrective surgery of the mandible
Ramus osteotomy ( sagittal split osteotomy, vertical subsigmoid osteotomy, c osteotomy, inverted L ostetomy).
Body angle osteotomy.
Anterior segmental osteotomy.
Posterior segmental osteotomy.
Genioplasty.
Corrective surgery of the maxilla
Total maxillary osteotomy ( lefort 1 lefort 2, lefort 3).Segmental alveolar osteotomy
• Anterior segmental alveolar osteotomy or ostectomy.
• posterior segmental alveolar osteotomy or ostectomy.
Finally bimaxillary surgery in the upper and lower jaw.
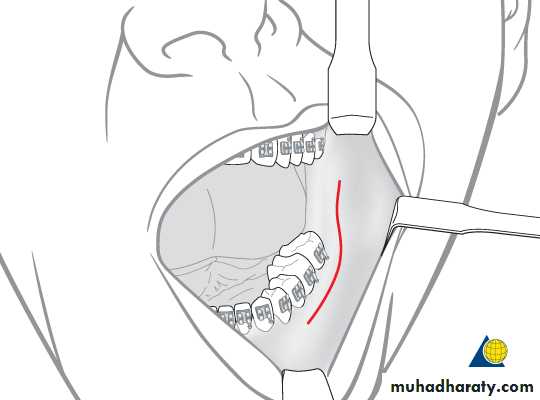
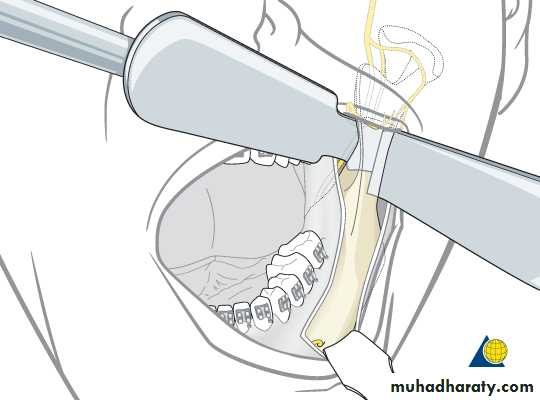
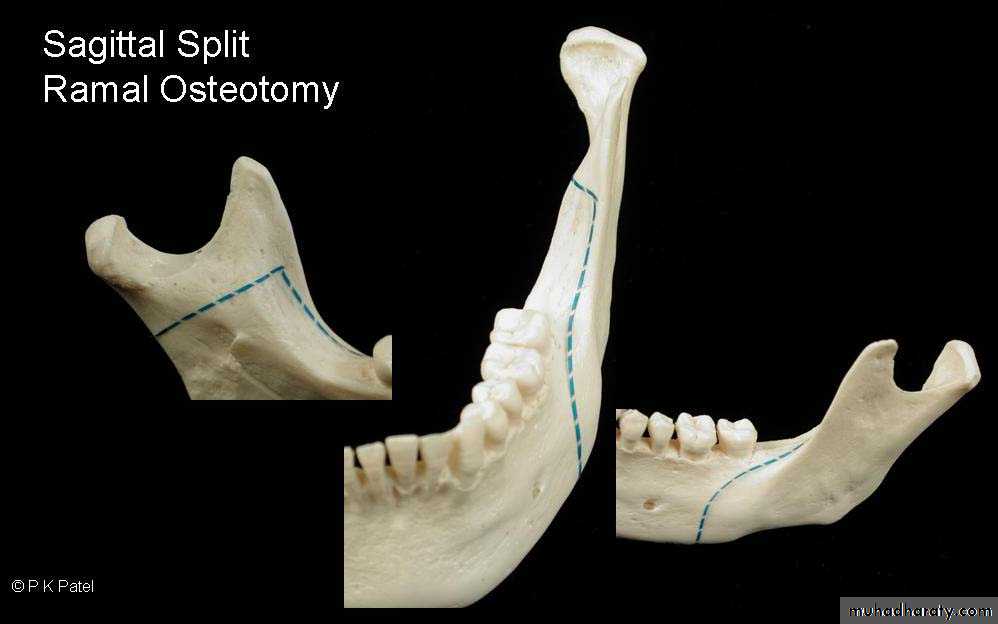
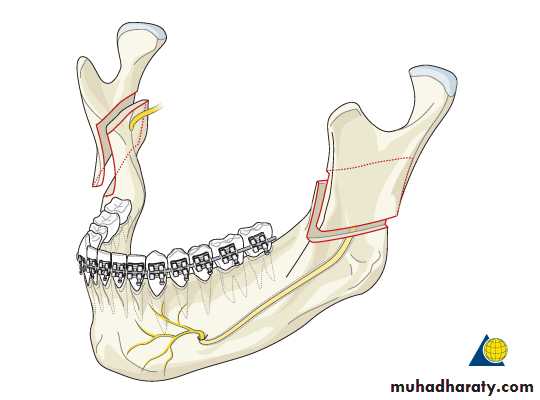
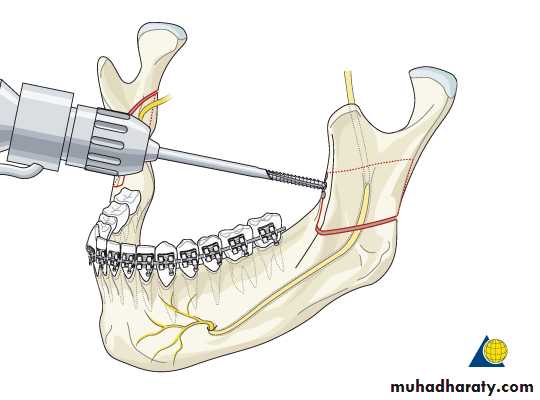
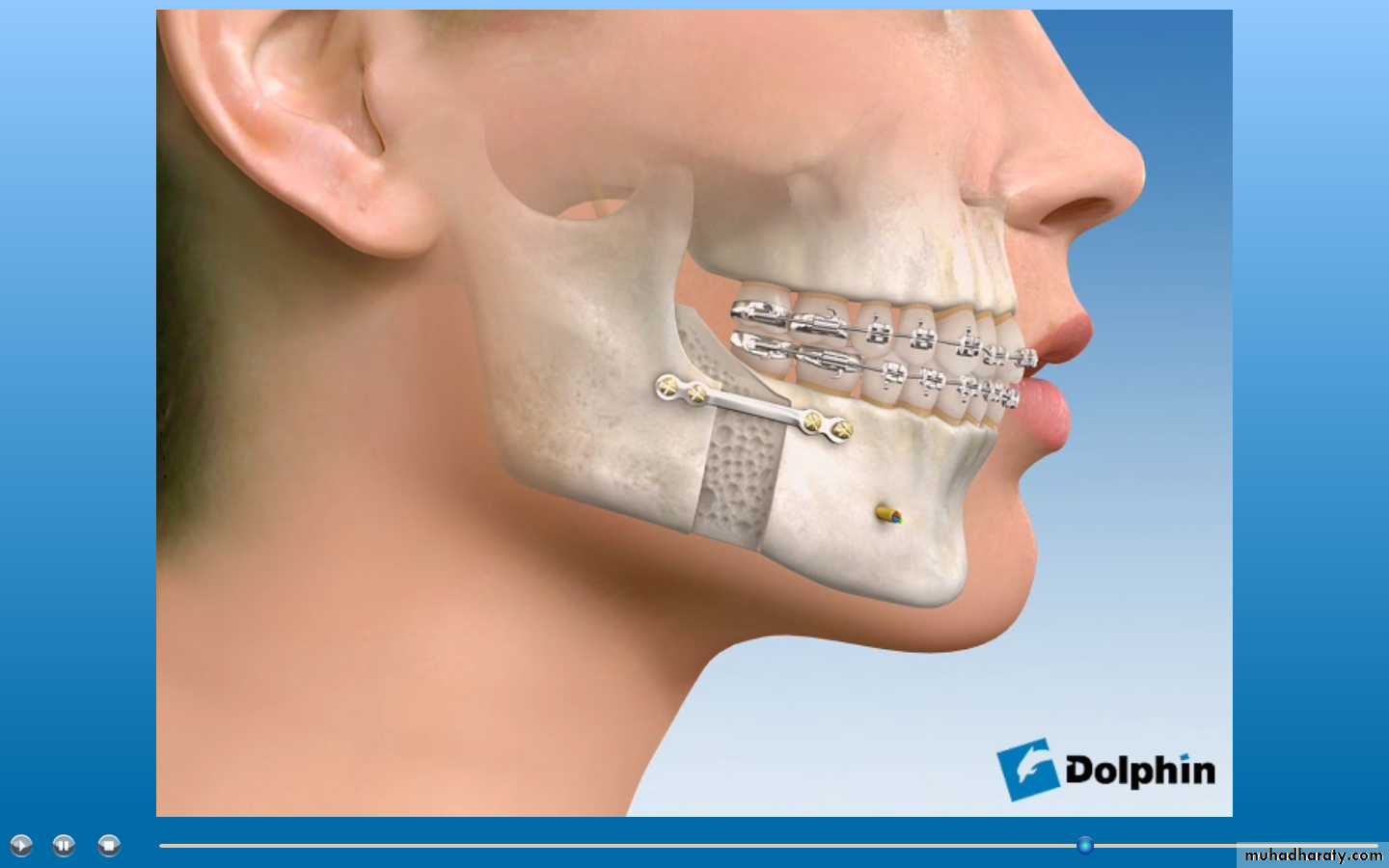
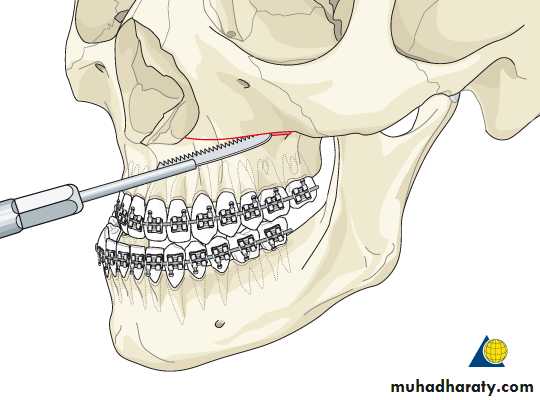
Sagittal split osteotomy
Introduced by Trauner and obwegeser, modified by Dal pont and Hunsuk.The natural plane of cleavage between the buccal and lingual cortical plates of the ramus is used to develop a sagittal splitting separating the proximal (condylar segment) from the distal (dento-alveolar segment).
Sagittal ramus osteotomy
Indications of SSO
Correction of mandibular retrusion. Usually can be combined with genioplasty carried out simultaneously, alternative procedure for mandibular advancement are the inverted L osteotomy and C ramus osteotomy.Correction of mandibular protrusion (prognathism).if the set back movement is graeter than 20 mm bimaxillary surgery should be considerd.
Correction of mandibular asymetry. Usually can be done bilaterally (BSSO) and combined with maxillary osteotomy ( bimaxillary surgery)
Compensatory repositioning of the occlusal plane.to allow other osteotomy to be done especially with the operation used for vertical adjustment of the mid face ( bimaxillary surgery).
Vertical subsigmoid osteotomyvso or ivso
One of the sipmlest mandibular osteotomy.Can be done intra orally(IVSO) or extra orally.
In this procedure we move the distal segment ( body and dentoalveolar) backwards with the proximal segment (condylar) overlap the distal segment laterally.
It is indicated for set back cases( mandibular prognathism).
Although interpositional bone graft can be used to increase ramus length ( correction of mandibular retrusion) and advance the distal segment.
The inverted L osteotomy is preferred for advancement cases (correction of mandibular retrusion).
sso
Vertical subsigmoid osteotomyVSO
Comparison
VSOSuitable for mandibular set back more than advancement.
Less danger of damage to inferior dental nerve but more danger to damage facial nerve branch(extra oral approach).
Extra oral scar.
Simple technique.
Less bone to bone contact.
SSO
Suitable for mandibular set back and advancement.
Slightly greater danger to damage inferior dental nerve and less danger to facial nerve.
No extra oral scar.
Technique require more learning.
More bone to bone contact.
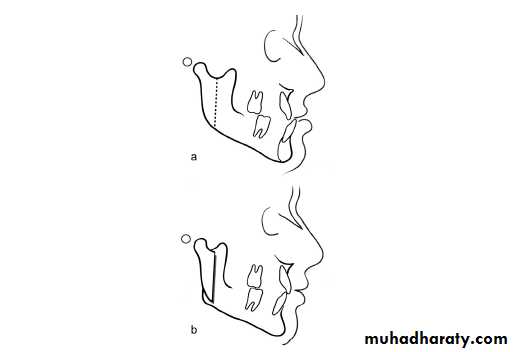
Anterior segmental osteotomy.KӦLE procedure
Osteotomy performed on the anterior mandible with separation of the labial segment of the alveolar bone form canine to canine or from first premolar to first premolar.
The osteotomized segment derived the blood supply from the soft tissue attached to the lingual aspect and it is important that this soft tissue attachment remain during the surgery.
Anterior subapical osteotomyKӦLE procedure
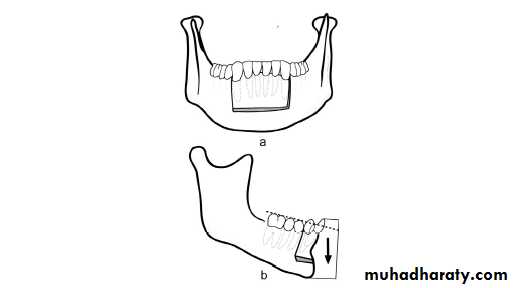
Anterior segmental osteotomy.KӦLE procedure / indications
The lower labial segment can be repositioned:-superiorly to correct anterior open bite. inferiorly ( after sub apical ostectomy). postreiorly ( after alveolar ostectomy).
or combination movement.
Can be combined with anterior maxillary osteotomy in cases with bimaxillary alveolar protrusion
Genioplasty / the management of the chin
From the front the chin may be asymmetric with deviation to the right or left .may be receded or protruded in profile view.
Method for correction include
• Simple reduction Genioplasty.
• Re contouring Genioplasty.
• Augmentation Genioplasty by bone graft or alloplastic material.
• Sliding Genioplasty.
Most often the Genioplasty procedure can be combined with other osteotomy procedure in the mandible like SSO or with other maxillary surgery as in bimaxillary osteotomy.
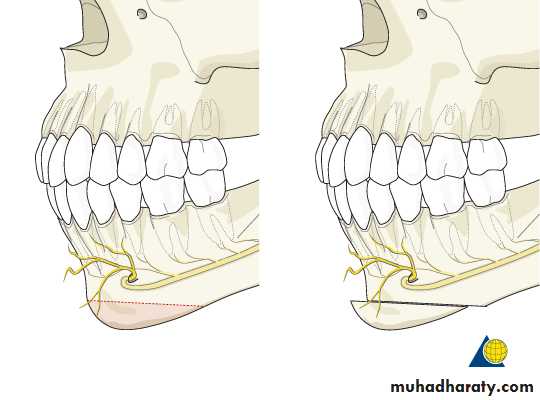
Genioplasty
For transverse genial deformities, vertical osteotomies/ostectomies can also be performed.This allows widening or narrowing of the chin. In case of widening, additional bone grafts or alloplastic implants (eg, ceramic blocks) are needed.

Genioplasty
Before
After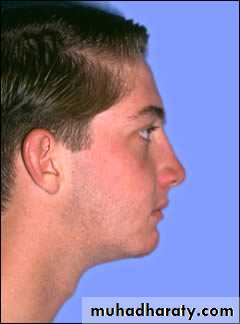
Maxillary osteotomy
The most common osteotomy performed in the maxilla are theLefort 1 osteotomy.
Anterior subapical (segmental) osteotomy, (WASSMUND PROCEDURE).
Posterior segmental osteotomy.
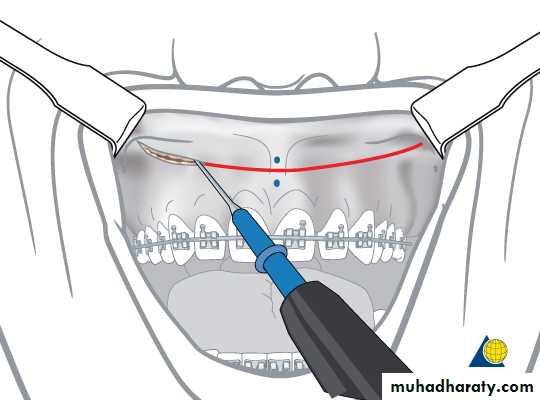
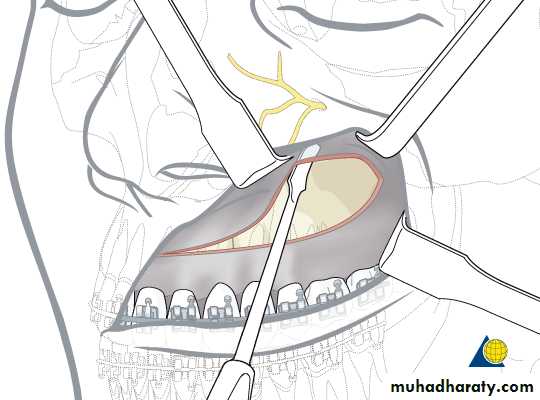
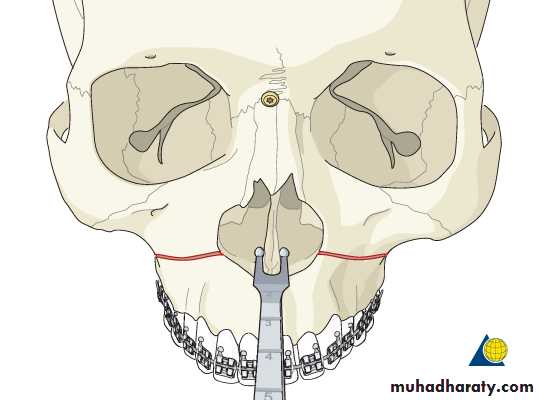
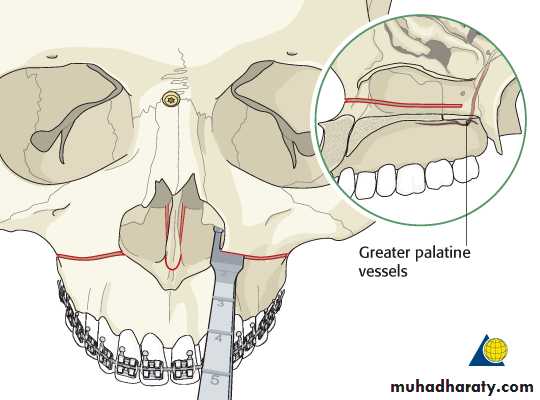
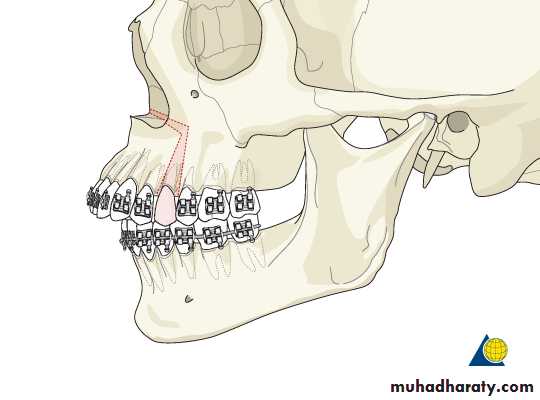
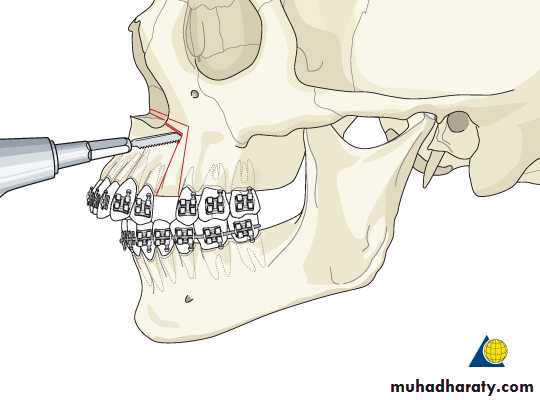
Lefort 1 osteotomy
Used to advance the maxilla and this is accomplished by carrying the osteotomy line posteriorly on the lateral wall of the maxilla to the point just above the pterygomaxillary suture.
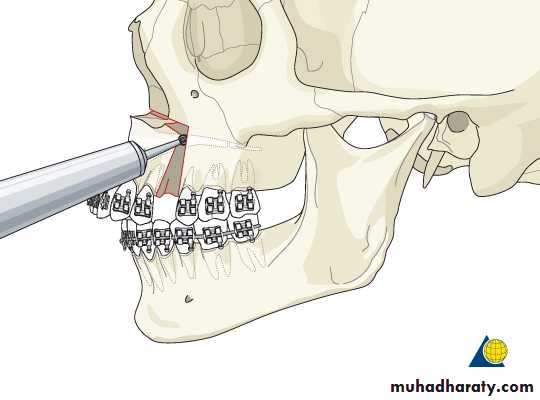
Curved osteotome used to separate the maxillary bloc anteriorly from the pterygoid plates ( pterygomaxillary dysjunction).
The osteotomy line run above the apices of the maxillary teeth.
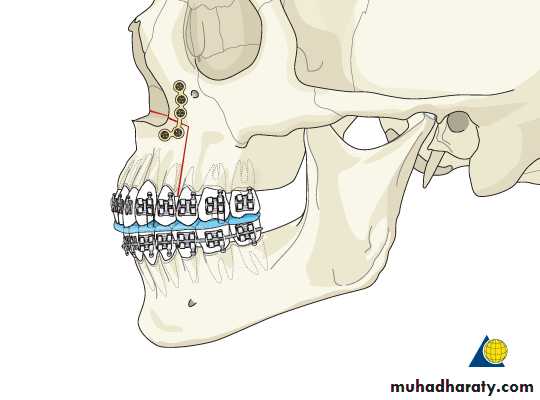
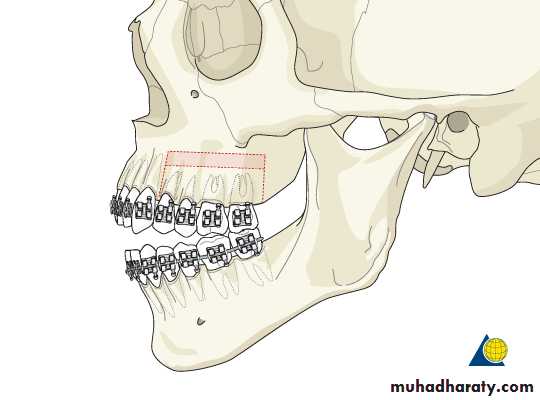
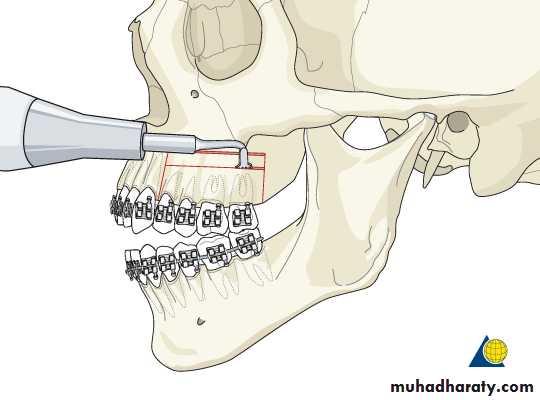
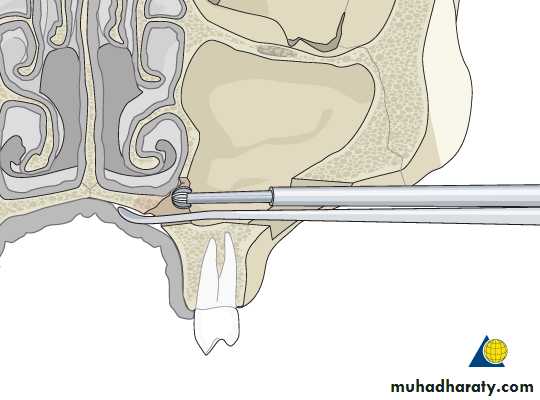
Anterior maxillary osteotomy.Anterior sub apical osteotomy.Anterior segmental osteotomy.Wassmund or Wunder osteotomy.
Used to mobilize the anterior segment of the maxilla allow repositioning in upward, downward or rotational manner by (osteotomy alone) or in posterior direction ( if ostectomy used).
The premolar tooth in each side( usually the first premolar) is extracted to gain space for mobilization.
Mainly used to correct maxillary protrusion and can be used in conjunction with anterior sub apical osteotomy of the mandible in cases of bimaxillary protrusion.
Anterior segmental osteotomy
Posterior maxillary osteotomy
Indicated inUnilateral posterior cross bite especially in older patients.
Excessive transverse width of the posterior maxilla.
For closure of posterior open bite by inferior repositioning of the posterior segment with post operative orthodontic retention for at least 18 months due to relapse.
Posterior maxillary osteotomy
Advantages of bimaxillary surgery
The patient undergo one surgical procedure, one hospitalization period, one anesthetic session and one inter maxillary fixation period.
The danger that the patient refusing further surgery is avoided during un acceptable stage of occlusion.
More stable results as the soft tissue tension will be distributed on both arches.
Complications and adverse effects of orthognathic surgery
Nerve injuriesNerve injuries in orthognathic surgery can be caused by indirect trauma, such as compression by surgical edema, or direct trauma, such as compression, tear or cut with surgical instruments or stretching during manipulation of the osteotomized bone segments
Complications
TMJ complication, fibrous ankylosis, hypomobility, condyle displacementVascular complication ( bleeding).
Relapse( skeletal and dental)
Infection.
Others ( fracture of the osteotomized segment, bad split, periodontal problems, teeth damage,
