Odontogenic Tumors
Dr. Wafaa Khalilجراحة \ خامس اسنان
د. وفاء م(17)
25\ 4\ 2017
Definition of Odontogenic Tumors
• Tumor:- The word tumor means swelling.• Odontogenic tumor:- A group of neoplasm & tumors-like malformations arising from cells of odontogenic apparatus & their remnants.
In other words, odontogenic tumors arise from odontogenic tissues.
Classification of Odontogenic Tumors
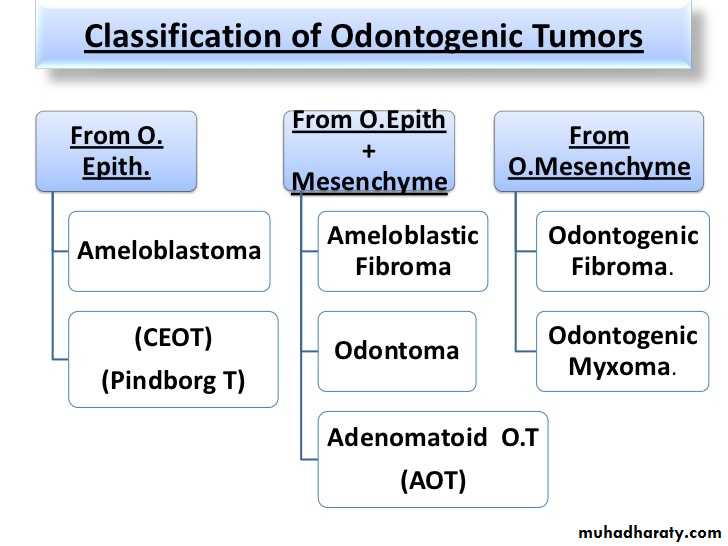
• Tumors of Odontogenic Epithelium
Follicular variant of the conventional solid ⁄ multicystic ameloblastoma.Plexiform variant of a solid ⁄ multicystic ameloblastoma
Ameloblastoma
• It is typically slow-growing, locally invasive and runs a benign course.• H.G.B. Robinson described it as being tumor that is “usually unicentric, non-functional, intermittent in growth, anatomically benign and clinically persistent.”
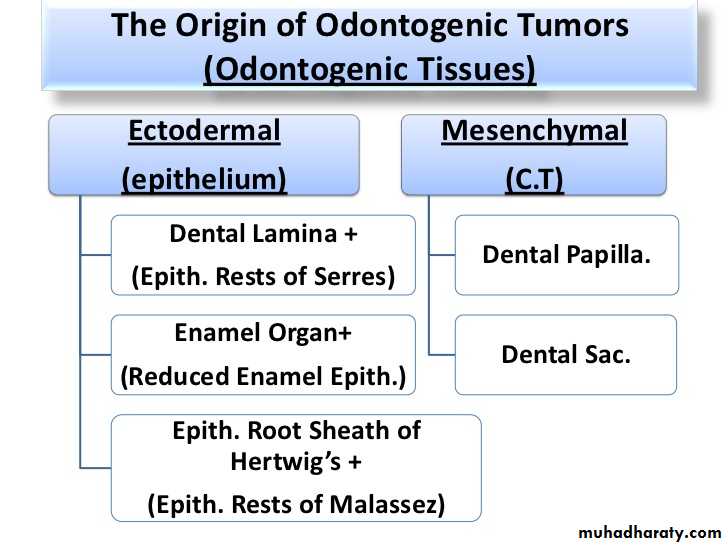
Several origins have been suggested:
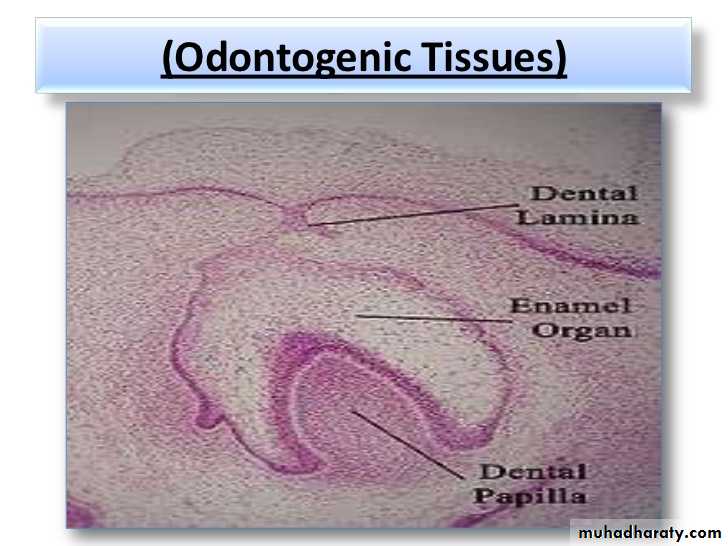
• Dental Lamina + its remnants ( epith. Rests of Serres).• Enamel organ + its remnants ( reduced enamel epith.).
• Epith. Lining of Dentigerous cyst.
• Basal layer of the oral mucosa.
Origin of Ameloblastoma
Types of Ameloblastoma
• 1- Simple, Solid,(Multicystic Ameloblastoma), with its histological variants:-
-Follicular A.
-Plexiform A.
• 2-(Unicystic Ameloblastoma), with its histological variants:
-Luminal Unicystic A
-Intraluminal Unicystic A
-Mural Unicystic A.
• 3- Peripheral (S.T) ameloblastoma.
• 4- Desmoplastic ameloblastoma.
Solid, Multicystic Ameloblastoma
Def. :• - It is a benign but locally invasive neoplasm consisting of epithelium lying in a fibrous stroma.
• - It is one of the few neoplasms that arise from odontogenic epith.
• - It has ↑ recurrence rate than other types of Ameloblastoma.
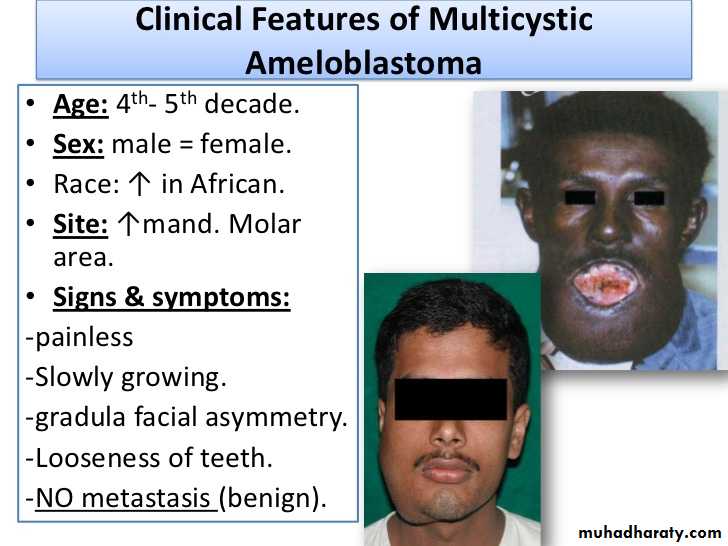
• Age: 4th- 5th decade.
• Sex: male = female.• Race: ↑ in African.
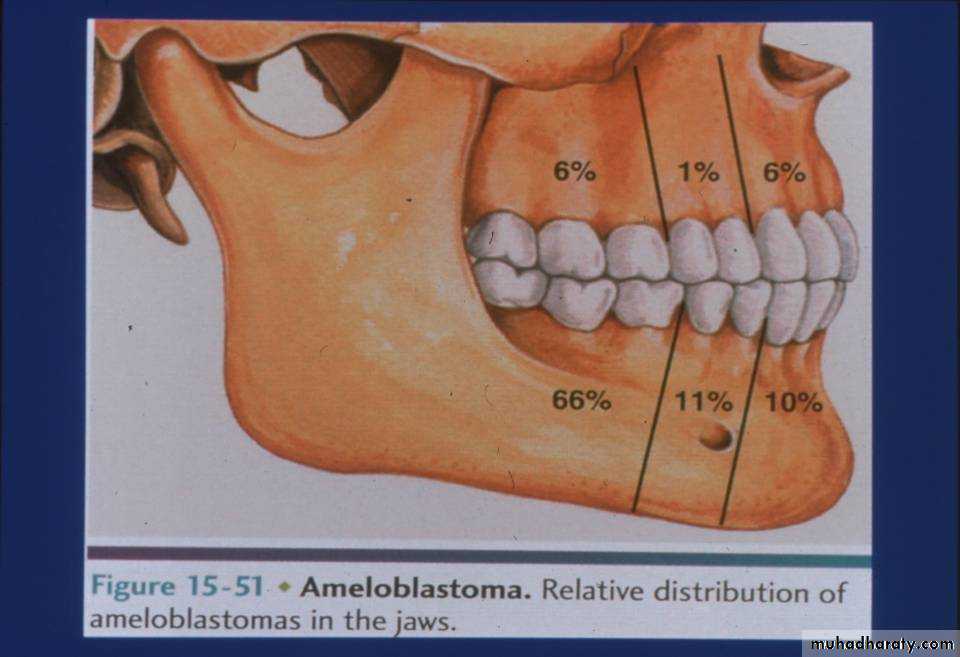
• Site: ↑mand. Molar area.
• Signs & symptoms:
-painless
-Slowly growing.
-gradula facial asymmetry.
-Looseness of teeth.
-NO metastasis (benign).
Solid, Multicystic Ameloblastoma
Clinical features
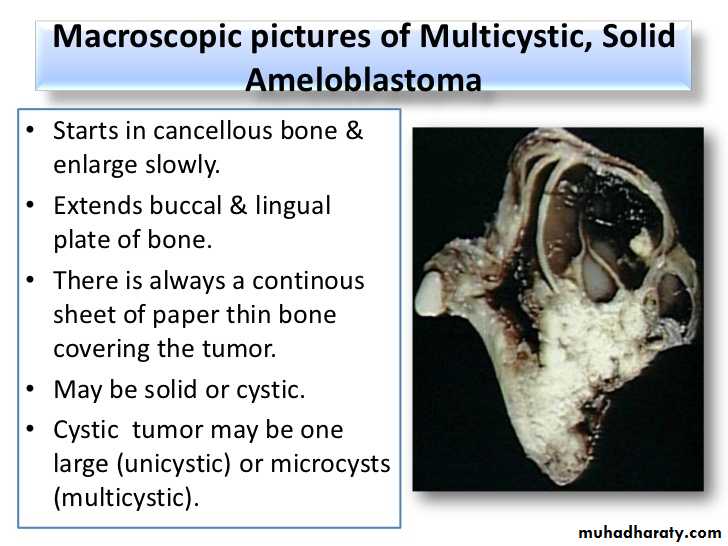
• Starts in cancellous bone & enlarge slowly.
• Extends buccal & lingual plate of bone.• There is always a continous sheet of paper thin bone covering the tumor.
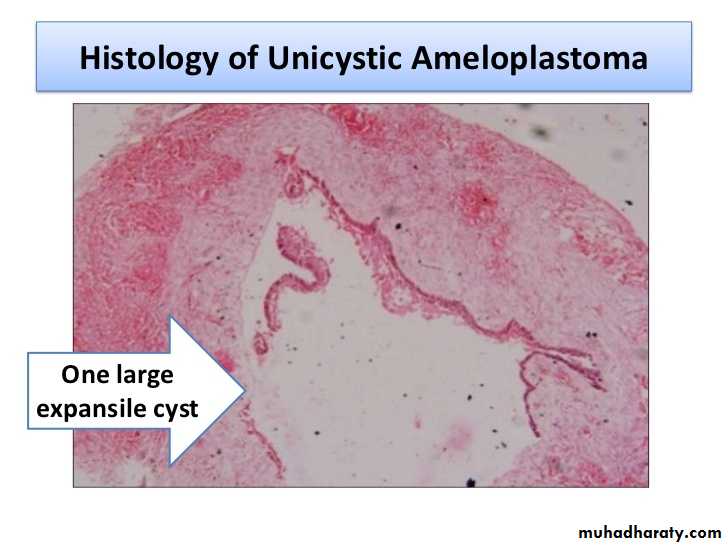
• May be solid or cystic.
• Cystic tumor may be one large (unicystic) or microcysts (multicystic).
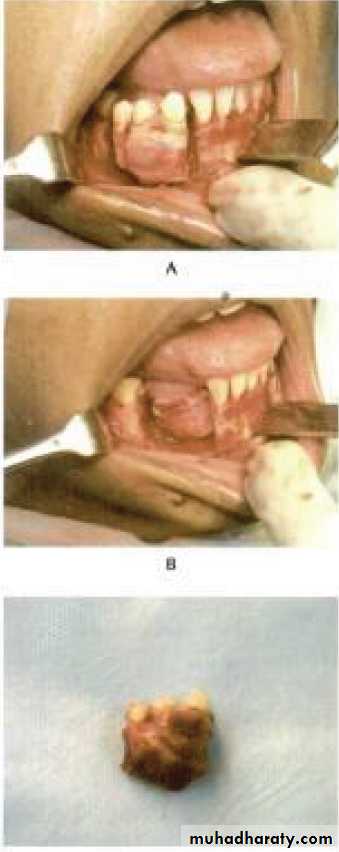
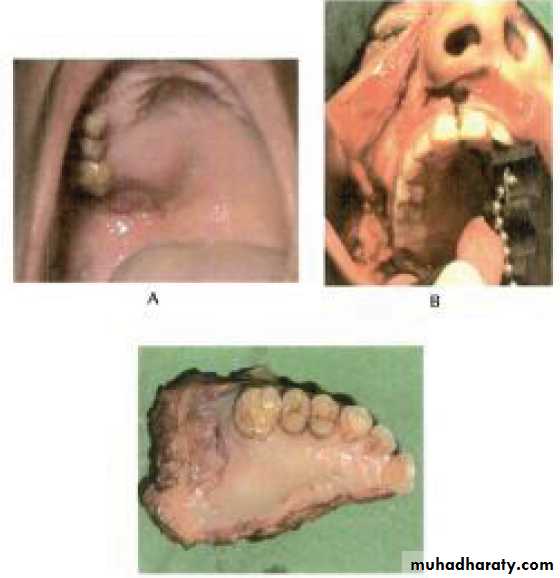
Solid, Multicystic Ameloblastoma Macroscopical pictures
Solid, Multicystic Ameloblastoma
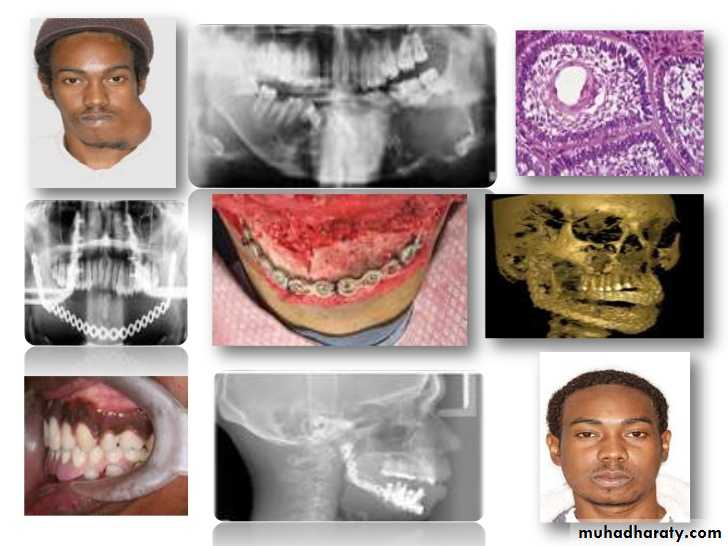
Radiographical appearance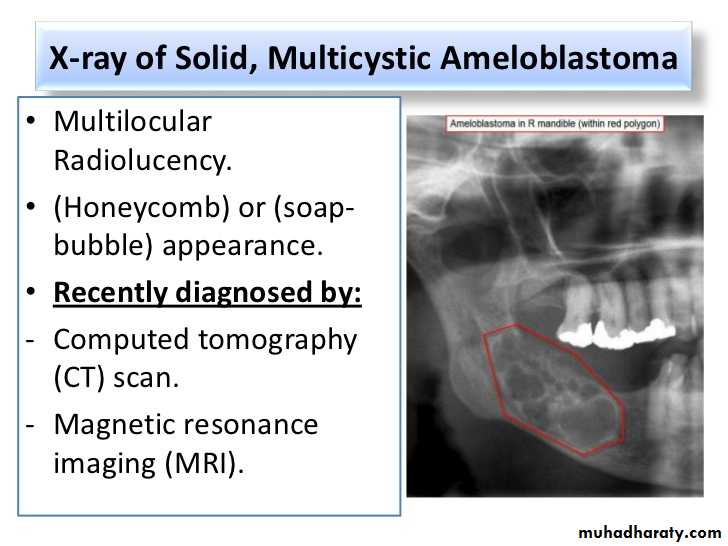
• Usually well-circumscribed;
• Multilocular Radiolucency.• (Honeycomb) or (soap- bubble) appearance.
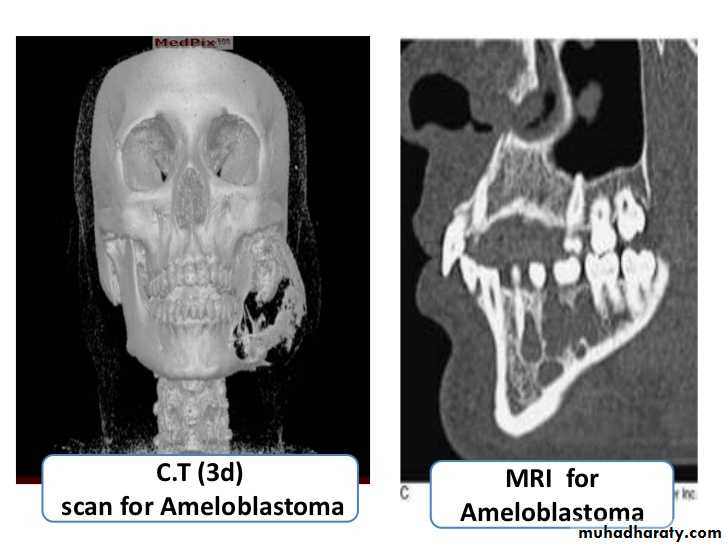
• Recently diagnosed by:
• Computed tomography (CT) scan.
• Magnetic resonance imaging (MRI).
Solid, Multicystic Ameloblastoma
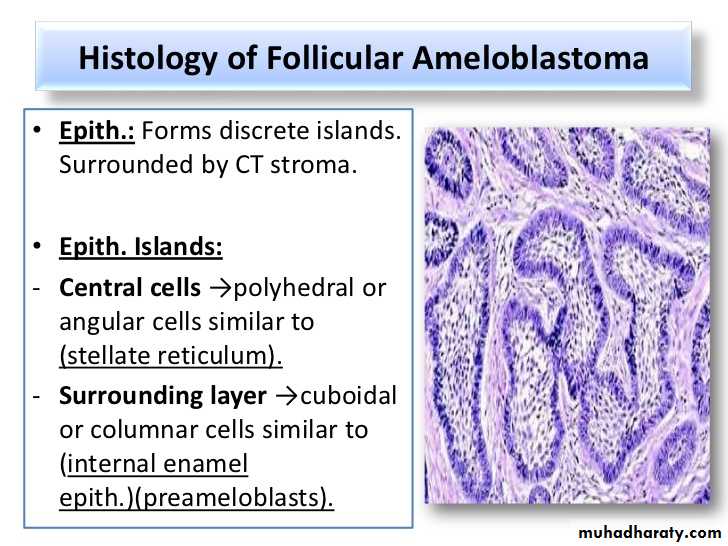
Histological feature• There are several microscopic subtypes but these generally have little bearing on the behavior of the tumor.
• The follicular and plexiform types are the most common.
• The follicular type is composed of islands of epithelium which resemble the enamel organ in a mature fibrous connective tissue stoma.
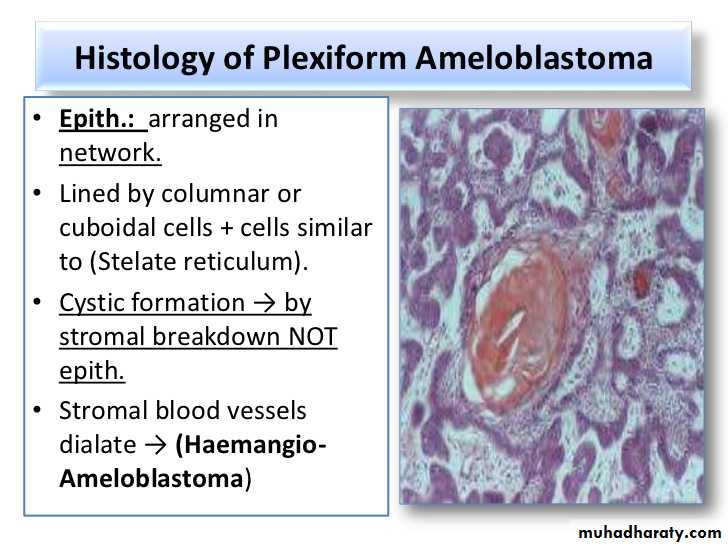
• The plexiform type is composed of long, anastomosing cords or larger sheets of odontogenic epithelium. Its stroma tends to be loose and more vascular.
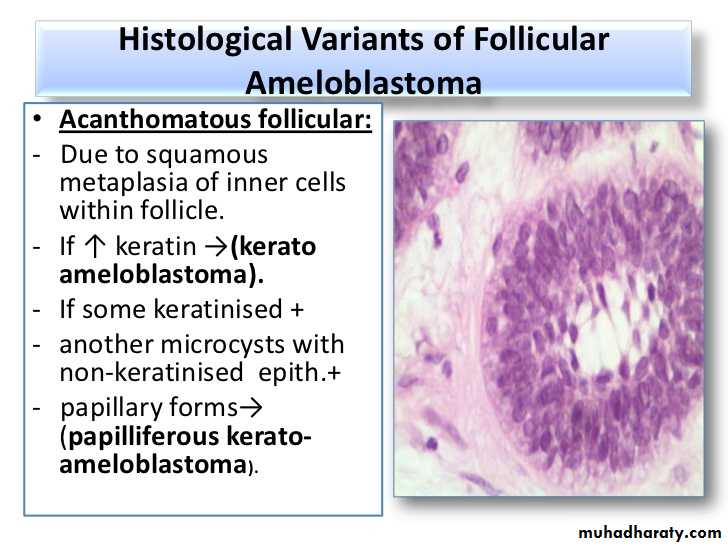
• The acanthomatous type shows evidence of extensive squamous metaplasia with keratin formation in the island of odontogenic epithelium.
Solid, Multicystic Ameloblastoma
Histological featureSolid, Multicystic Ameloblastoma
Additional feature
• In some studies solid/multicystic ameloblastomas are reported to be more common in Blacks.
• While lesions are generally asymptomatic, ameloblastomas may cause paresthesia, pain particularly if infected and they can erode the cortical palates.
Solid, Multicystic Ameloblastoma
Treatment• Treatments have ranged from simple enucleation and curettage to en bloc resection.
• Marginal resection is the most widely used method of treatment with the least recurrences reported (up to 15 %).
• Most surgeons advocate a margin of at least 1.0 cm beyond the radiographic limits of the tumor as the tumor often extends beyond the apparent radiologic/clinical margins.
• Treatment with curettage has resulted in recurrence rates ranging from 55-90 %.
• Treatment with marginal resection has resulted in approximately a 15 % recurrence rate.• Ameloblastomas of this type arising in the maxilla are particularly dangerous as it is often difficult in getting adequate margins.
• Rarely is an ameloblastoma life threatening.
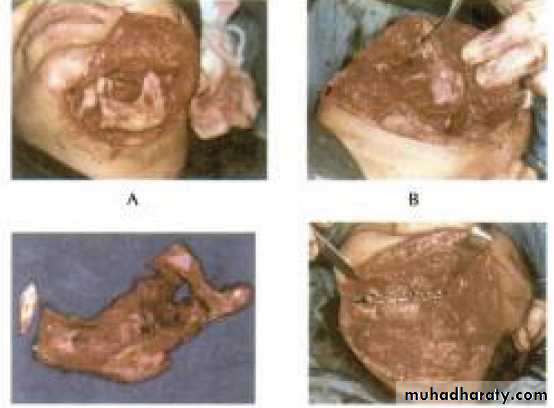
Solid, Multicystic Ameloblastoma
prognosis

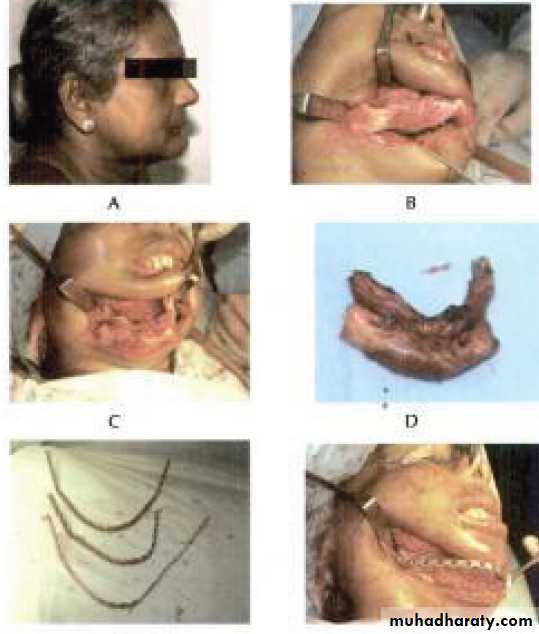
• En block resection
Segmental resection of the mandible
Hemi-Maxillectomy
Hemi-mandibulectomy
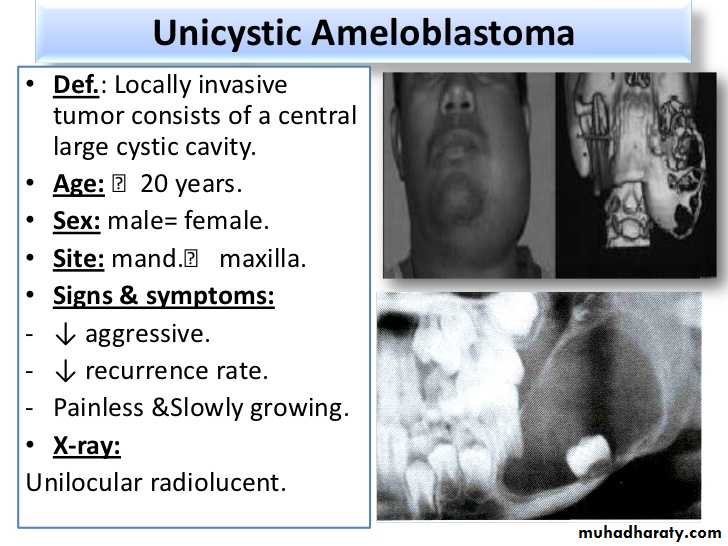
Unicystic Ameloblastoma
Clinical feature• Def.: Locally invasive tumor consists of a central large cystic cavity.
• Age: ˂20 years.
• Sex: male= female.
• Site: mand.˂ maxilla.
• Signs & symptoms:
• ↓ aggressive.
• ↓ recurrence rate.
• Painless &Slowly growing.
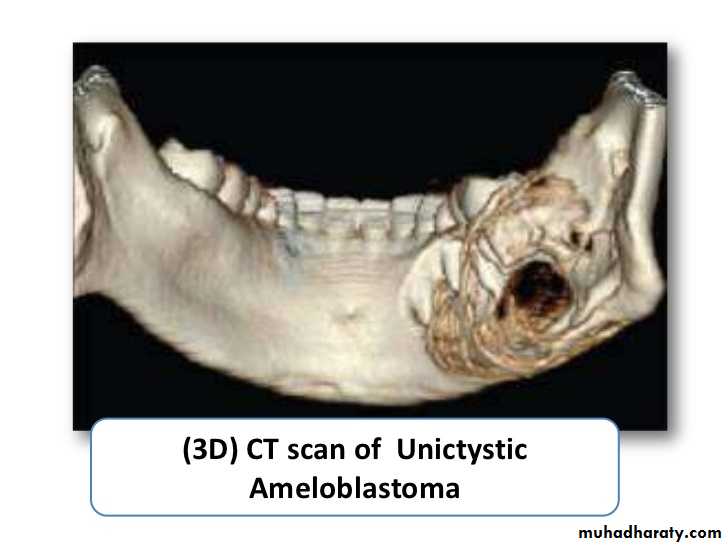
• X-ray:
• Unilocular radiolucent.
Unicystic Ameloblastoma
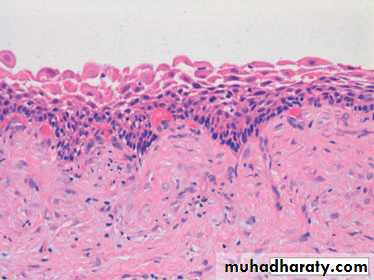
Histological featurePart of the wall of a unicystic ameloblastoma showing detail of the lining epithelium. Although more subtle than in solid ⁄ multicystic ameloblastomas, there is some basal palisading. The spiky rete processes and loosely attached suprabasal cells are further diagnostic aids in the appropriate clinical context. This is the luminal variant as neither intraluminal nor intramural ameloblastoma was present.
Unicystic Ameloblastoma
Treatment and prognosis• Enucleation of the cyst is probably adequate for the luminal and intraluminal/plexiform types.
• Treatment of the mural type is controversial with some surgeons believing that local resection is best.
• 10-20 % recurrence after enucleation and curettage with all unicystic ameloblastomas.

• Peripheral Ameloblastoma
• These tumors are extraosseous and therefore occupy the lamina propria underneath the surface epithelium but outside of the bone.• Histologically, these lesions have the same features as the intraosseous forms of the tumor.
• Malignant Ameloblastoma and Ameloblastic Carcinoma
• Less than 1 % of the ameloblastomas show malignant behavior with the development of metastases.• Malignant ameloblastoma is a tumor that shows histologic features of the typical (benign) ameloblastoma in both the primary and secondary deposits.
• Ameloblastic carcinoma is a tumor that shows cytologic features of malignancy in the primary tumor, in recurrence and any metastases.
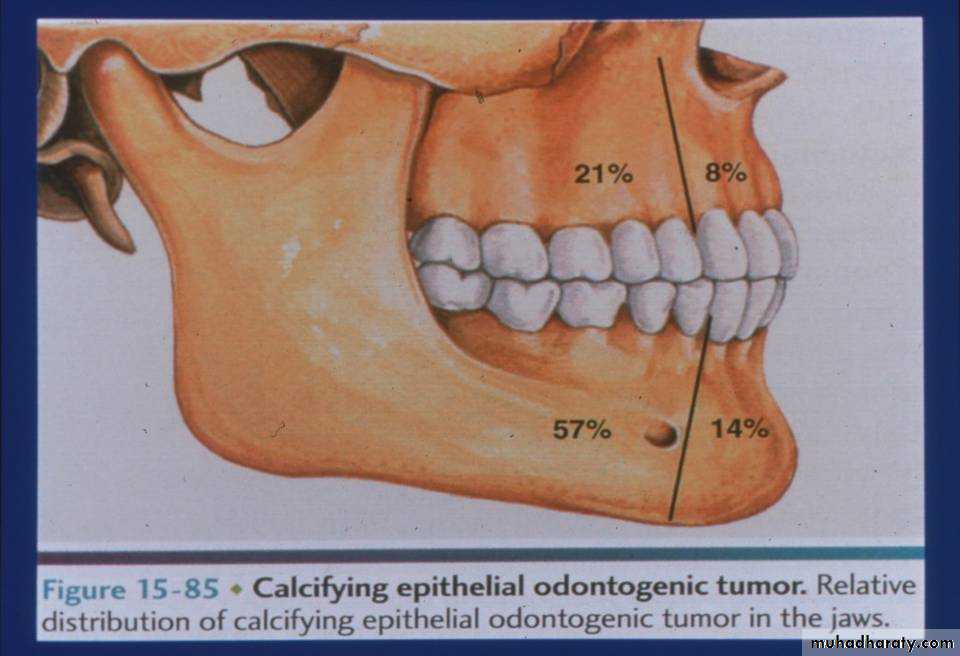
Calcifying Epith. Odontogenic Tumor (CEOT) (Pindborg’s Tumor)
Def.:• It is a locally invasive epith. Neoplasm characterized by the development of intra- epith. Structure probably of an amyloid-like nature.
• This amyloid-like structure may become calcified & liberated into the surrounding stroma.
• Origin (Histogenesis):
• (Reduced E.E) of associated unerupted tooth.
Calcifying Epith. Odontogenic Tumor Clinical features
• Age: between 20-60 years.• Sex: M=F
• Site:
- Intraosseous →mand˂max (post.).
- Extraosseous→anterior.
• Signs & symptoms:
• painless.
• Slowly growing.
• Associated with impacted tooth.
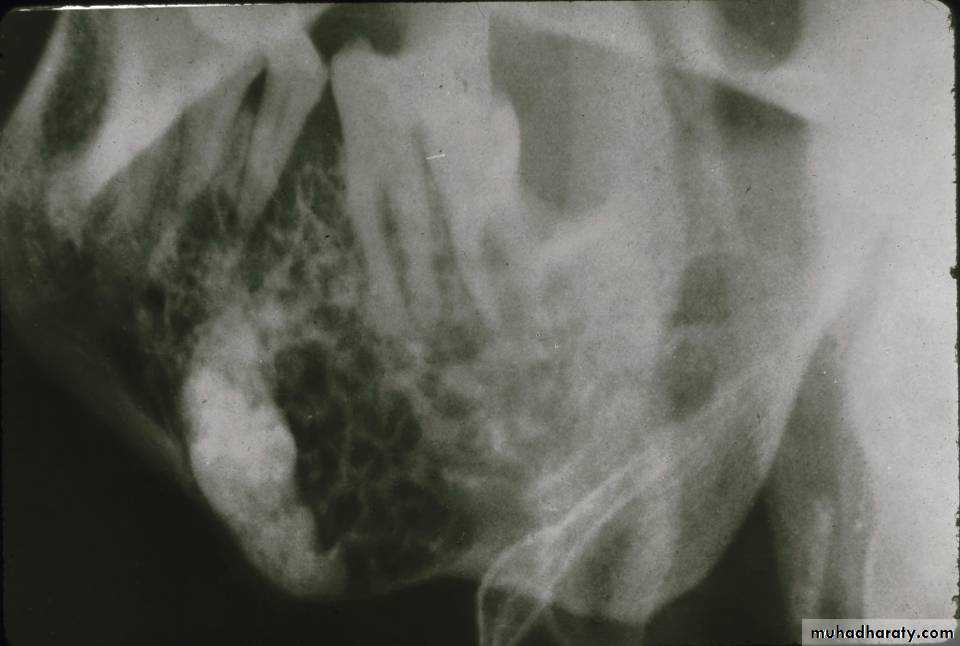
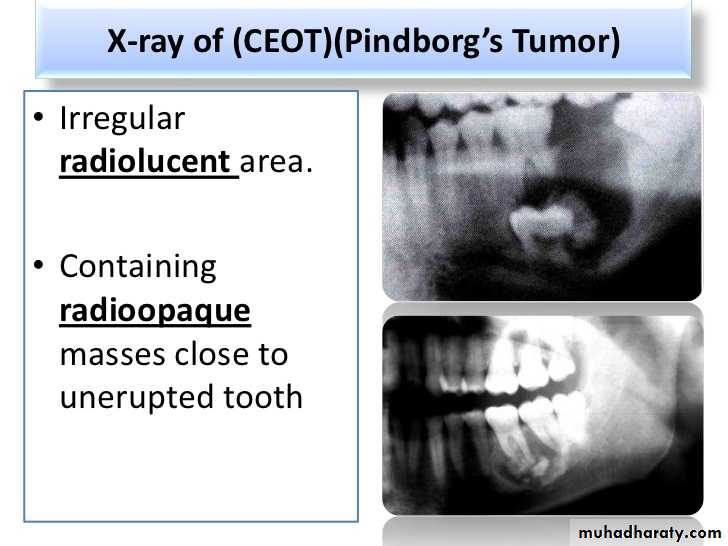
• CEOTs occur as radiolucent lesions with/without opaque foci.
• They are usually well-circumscribed and may be unilocular or multilocular.• Slightly over 50 % of the CEOTs are associated with an unerupted tooth.
Calcifying Epith. Odontogenic TumorRadiographical features
CEOT: Additional Features, Treatment and Prognosis
• Bony lesions most commonly present as painless, slow-growing swellings.• Peripheral lesions typically appear as non-specific sessile gingival masses.
• Conservative local resection is the treatment of choice as these lesions are typically less aggressive than the ameloblastoma.
• With this treatment the recurrence rate is approximately 15 % and the overall prognosis is good.
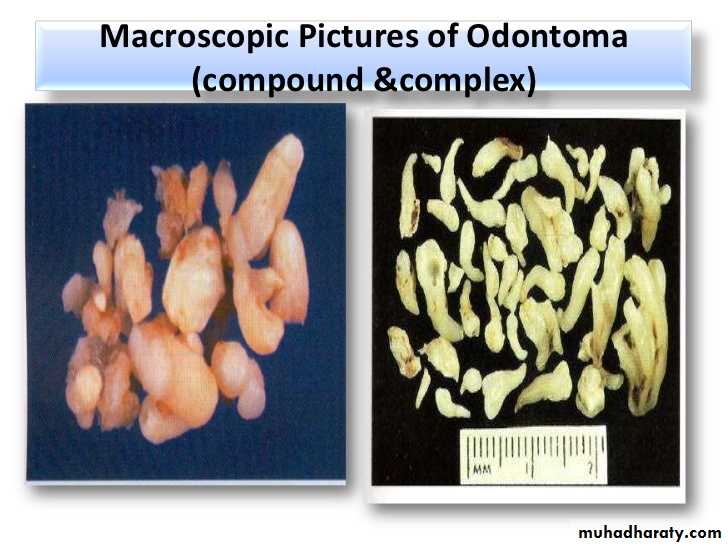
Odontoma
• The odontoma is the most common odontogenic tumor.• It is not a true neoplasm but rather is considered to be a developmental anomaly (hamartoma).
• Two types of odontomas are recognized:
• Compound
• Complex
Odontoma
Compound OdontomaComplex Odontoma
• Def.: a malformation in
which all dental tissues
are represented in more
orderly pattern than
complex.
• Contains many many tooth-like structures.
• Don’t resemble the
normal tooth morphologically.
• Def.: a malfrmation in
which all dental tissues
are represented in more
disorderly pattern.
• Contains many
disordered tooth-like structures.
• Don’t resemble normal tooth morphologically.
• Patient Age: Most cases are recognized during the second decade of life with a mean of 14 years.
• Gender Predilection: Approximately equal.
• Location: Somewhat more common in the maxilla. The compound type is more often in the anterior maxilla while the complex type occurs more often in the posterior regions of either jaw.
Odontoma
Clinical features
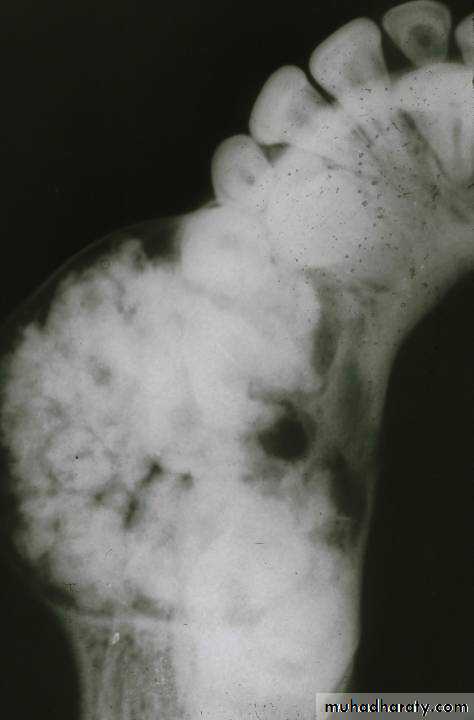
• Early lesions are radiolucent with smooth, well-defined contours.
• Later a well-defined radiopaque appearance develops.• The compound type shows apparent tooth shapes while the complex type appears as a uniform opaque mass with no apparent tooth shapes present.
Odontoma
Radiographical features
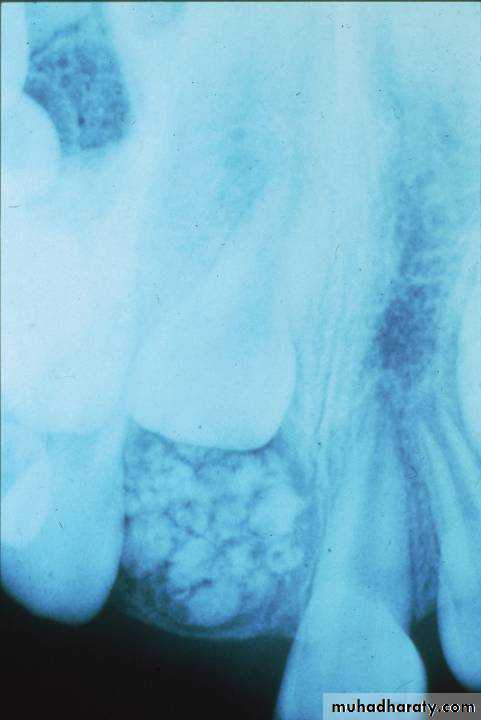

• Most odontomas are small and do not exceed the size of a normal tooth in the region.
• However, large ones do occur and these may cause expansion of the jaw.• Most odontomas are asymptomatic and as a result are discovered upon routine radiographic examination.
• Odontomas may block the eruption of a permanent tooth and in these cases are often discovered when “searching for” the “missing” tooth radiographically.
Odontoma
Additional features
Odontoma
Treatment and prognosis• Odontomas are treated by simple local excision and the prognosis is excellent.
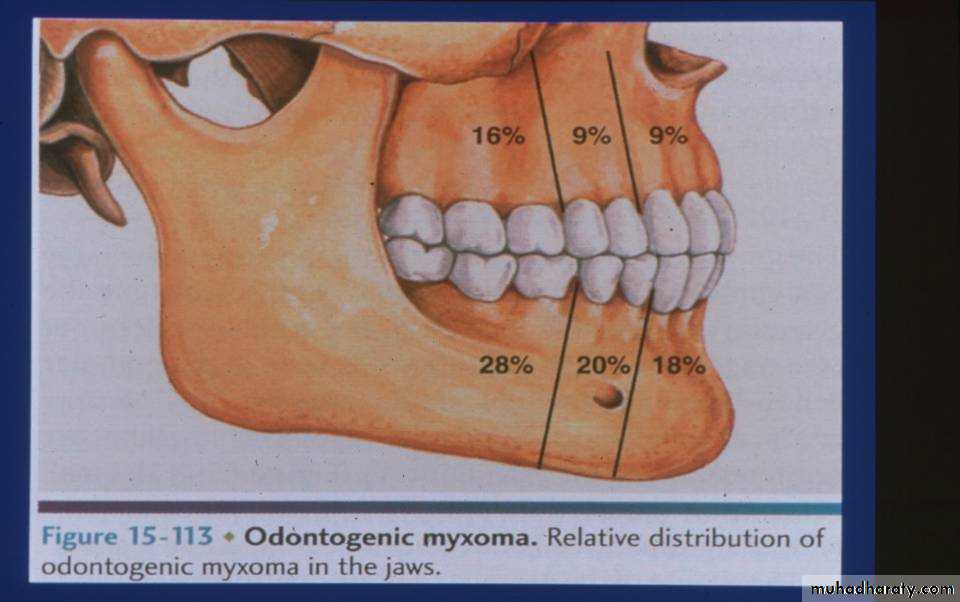
• Odontogenic Myxoma: Clinical and Radiographic Features
• Patient Age: 10-50 years with a mean around 30 years.• Gender Predilection: Reported to be about equal.
• Location: May occur in any area of the jaws but more common in the mandible.
• Radiographic Appearance: Radiolucent lesion often with a multilocular appearance. The borders may be indistinct.
• Odontogenic Myxoma: Histologic Features
• The tumor is composed of loosely arranged stellate, spindle-shaped and round cells in an abundant, loose myxoid stroma with few collagen bundles.• Epithelial cells are not required for diagnosis.
• The odontogenic myxoma may be confused with a chrondromyxoid fibroma or with myxoid change in an enlarged dental follicle or papilla.
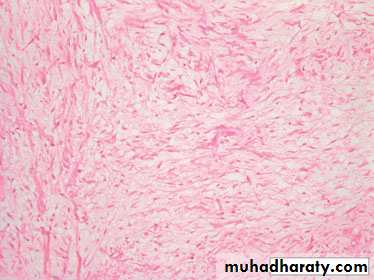
The odontogenic myxoma contains more delicate, dispersed collagen fibers, between which is glycosaminoglycan, which gives the tumor its mucinous consistency. Epithelial cells may not be present, as in this example.
• Odontogenic Myxoma: Treatment and Prognosis
• Small odontogenic myxomas are treated by curettage, while larger lesions may require surgical resection.• Odontogenic myxomas are not encapsulated and tend to infiltrate adjacent tissues.
• Recurrence rates of up to 25 % are reported.
• Overall, the prognosis is good for most odontogenic myxomas.