Approach to the patient with Diarrhea
Definition of Diarrhea
Three or more stool motion/Day
Loose –watery stool
Stool weight >200 g
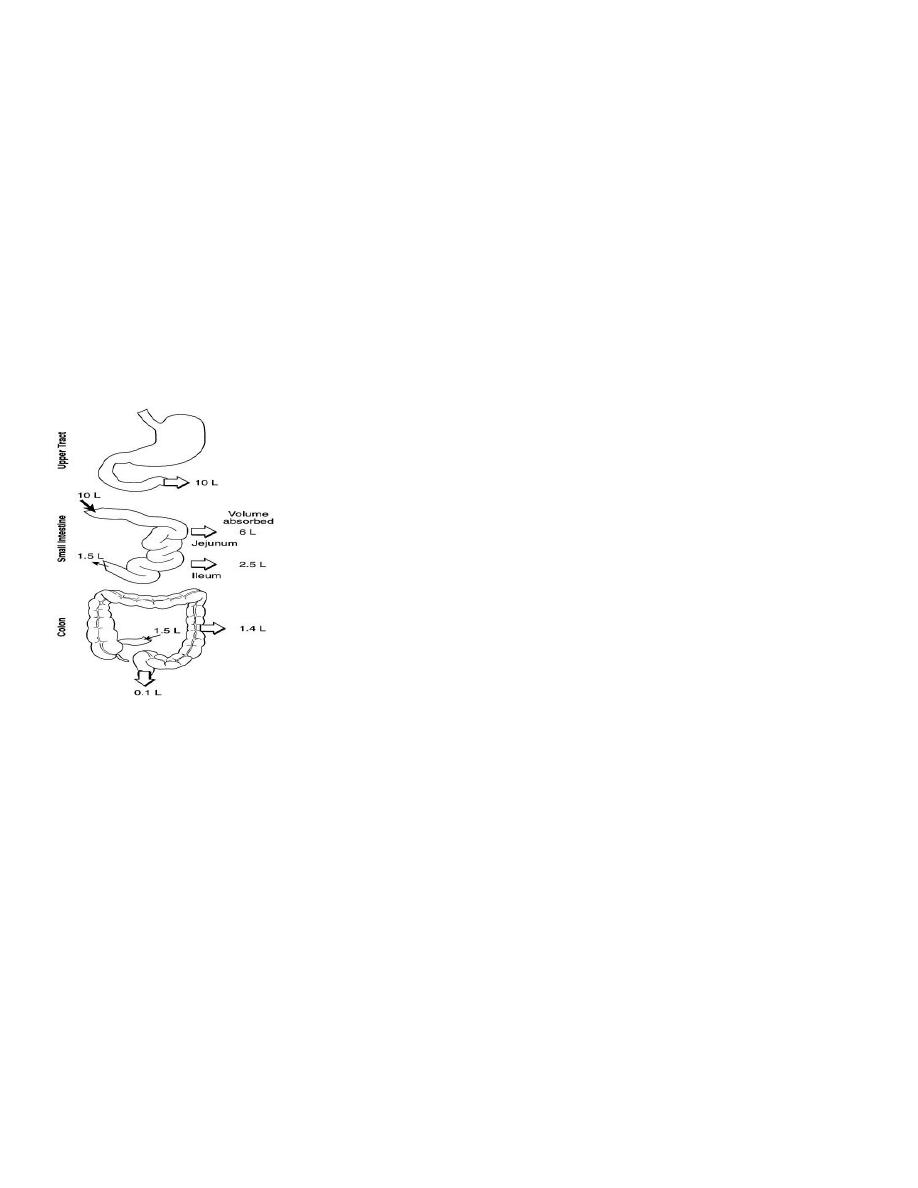
Mechanism of Diarrhea
Clue for diagnosis
▪ Acute versus chronic
▪ Small bowel versus large bowel
▪ Osmotic versus secretary
▪ Inflammatory versus fatty versus secretory
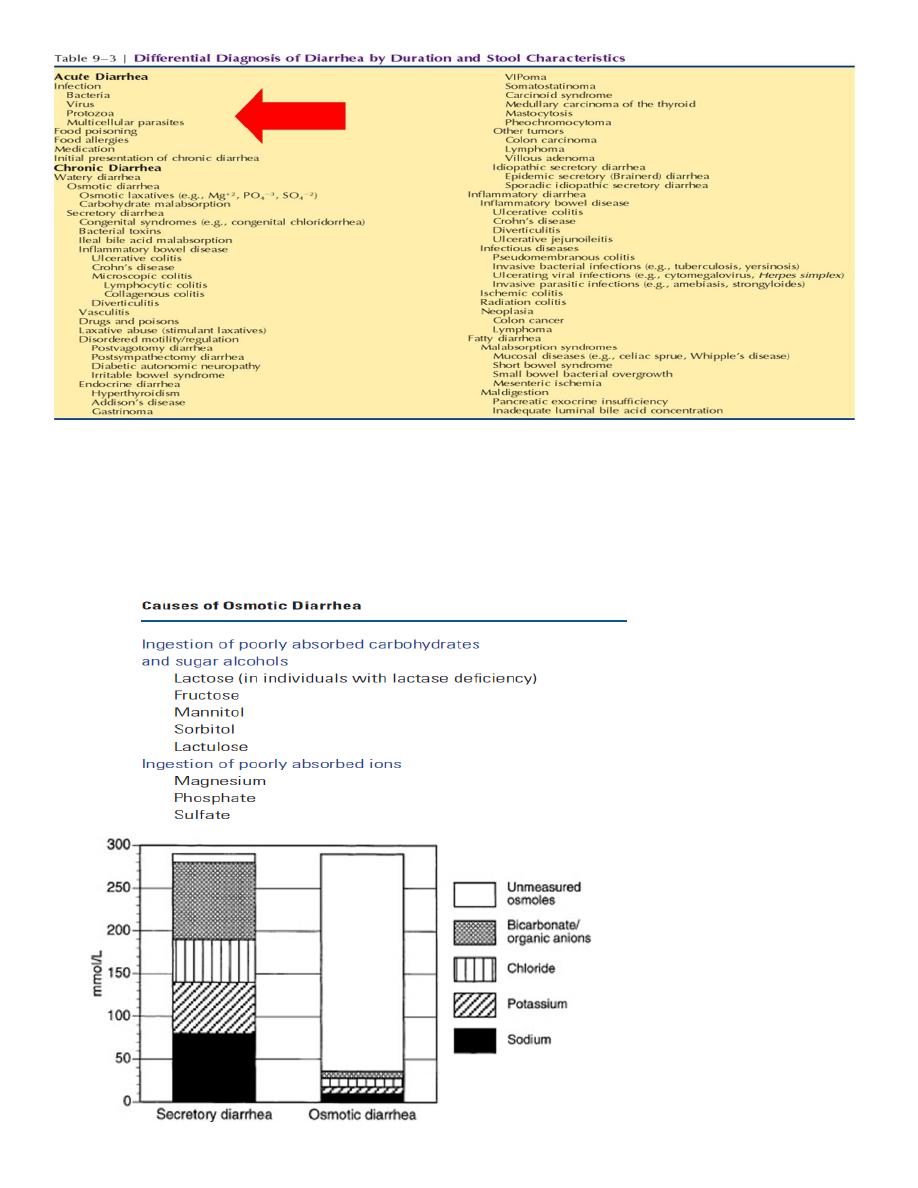
fecal osmotic gap=290-2(Na+k)
A fecal osmotic gap of >50 mosm/kg is suggestive of an osmotic diarrhea and
a gap of >100 mosm/kg is more specific.

Evaluation of Patient with Diarrhea
History
▪ Duration :acute diarrhea (<4 weeks’ duration)
▪ Frequency and volume .
▪ Dehydration or volume depletion.
▪ Stool characteristics.
▪ Relationship of defecation to meals or fasting.
▪ Day versus night.
▪ Fecal urgency or incontinence.
▪ previous surgery, medications, or radiation therapy.
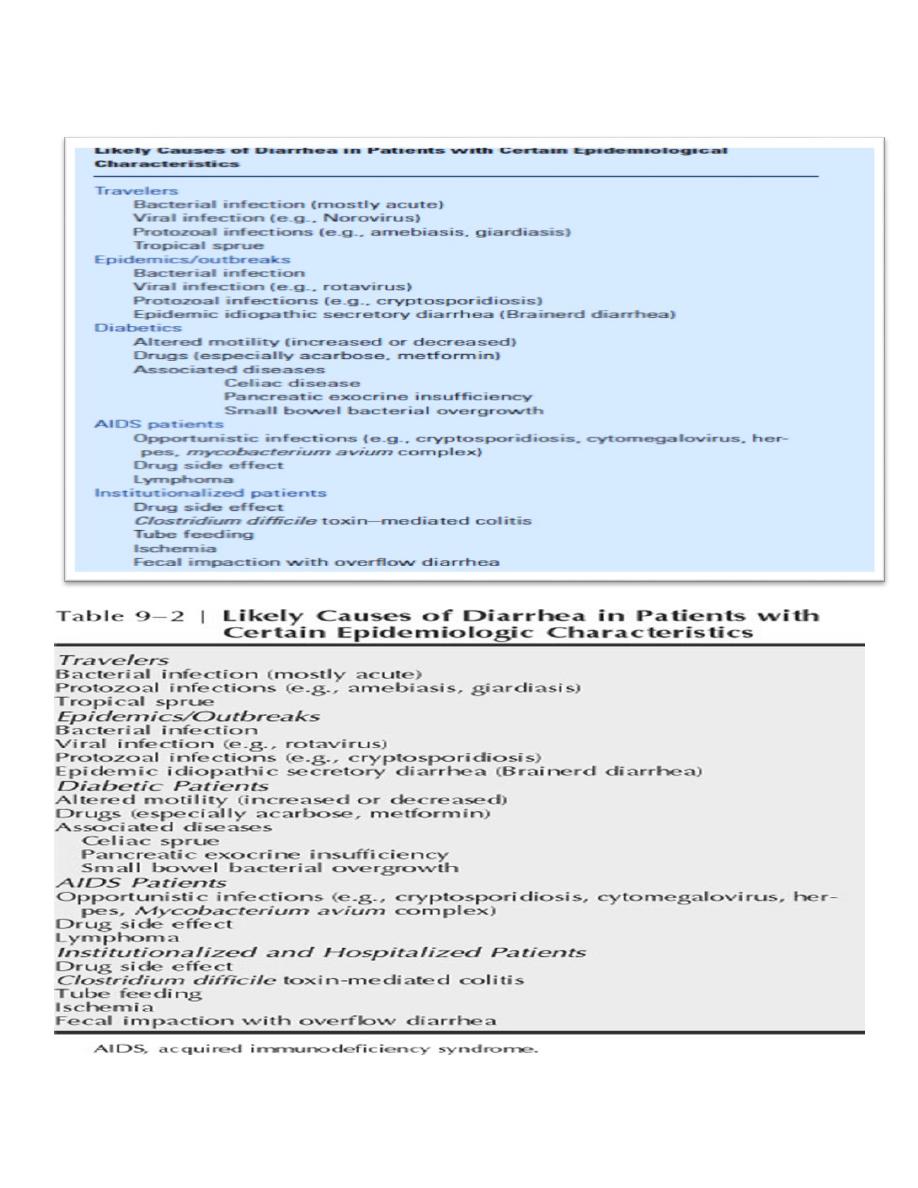
▪ Epidemiological clues.
Physical Examination
▪ severity of diarrhea and its cause.
▪ bowel sounds, abdominal distention and tenderness.
▪ skin changes, Thyroid nodules, right-sided heart murmur, Arthritis
,Lymphadenopathy ….etc.
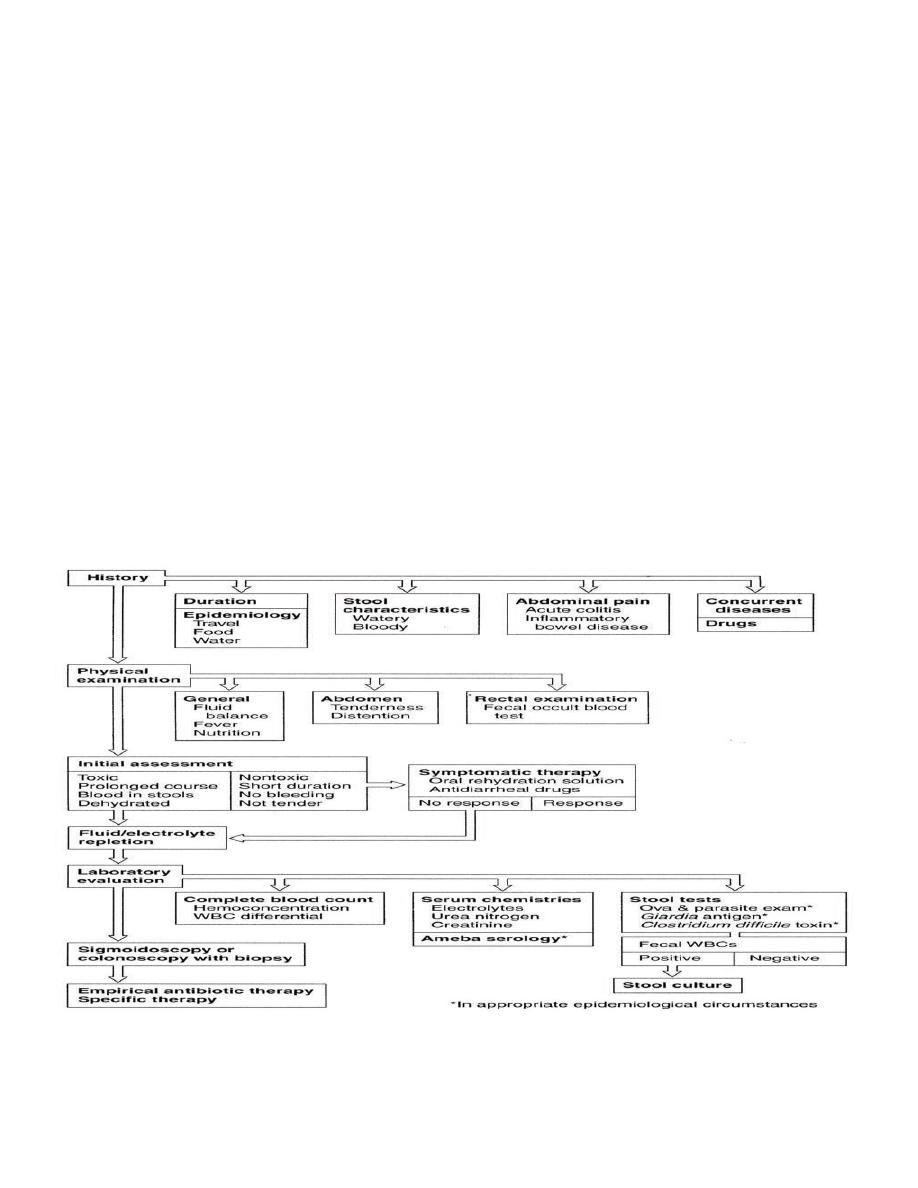
Further Evaluation of Acute Diarrhea
Infectious?
complete blood count
serum electrolyte concentrations, blood urea nitrogen, and serum creatinine
level.
stool sample
fecal lactoferrin or calprotectin levels.
stool cultures .
ELISA testing for giardiasis and serological testing for amebiasis
stool sample for C. difficile toxin.
Proctoscopy , flexible sigmoidoscopy , colonoscopy.
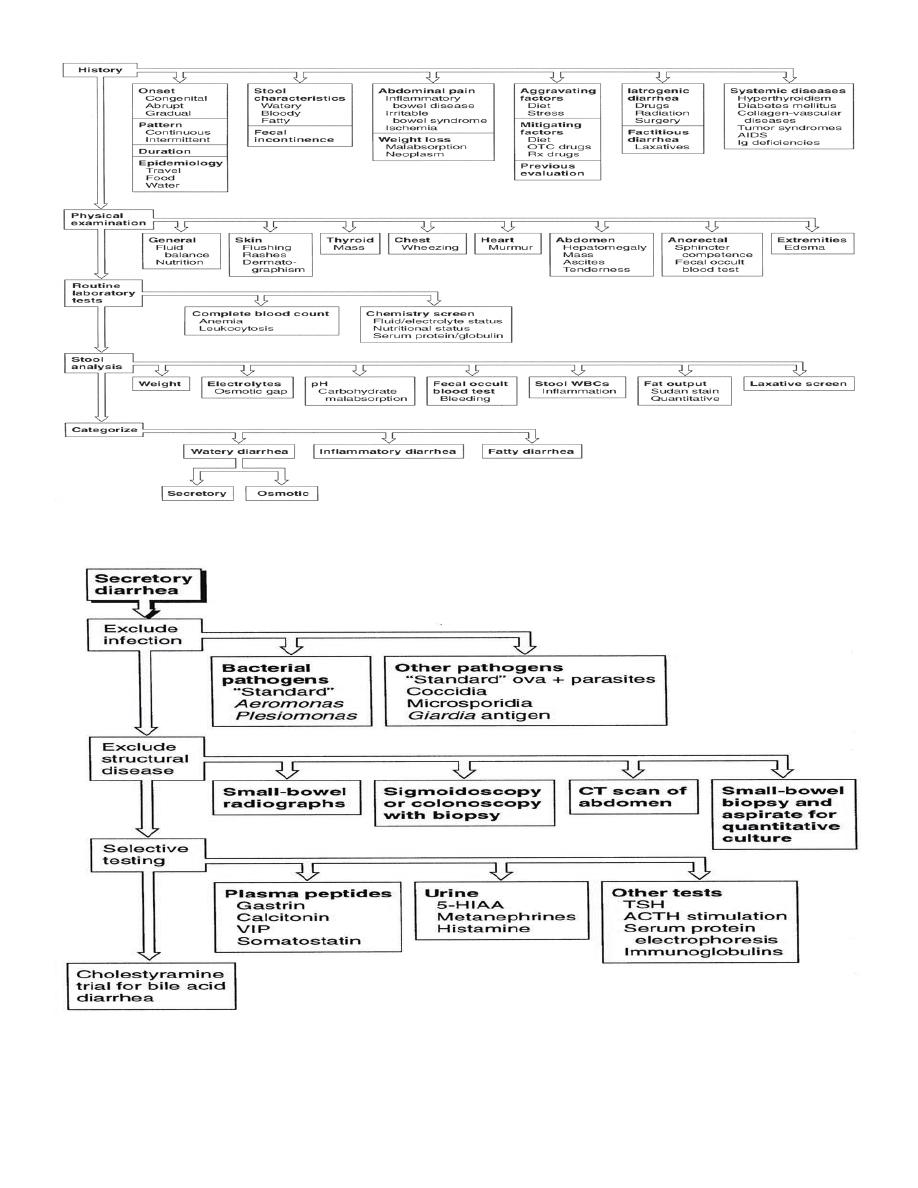
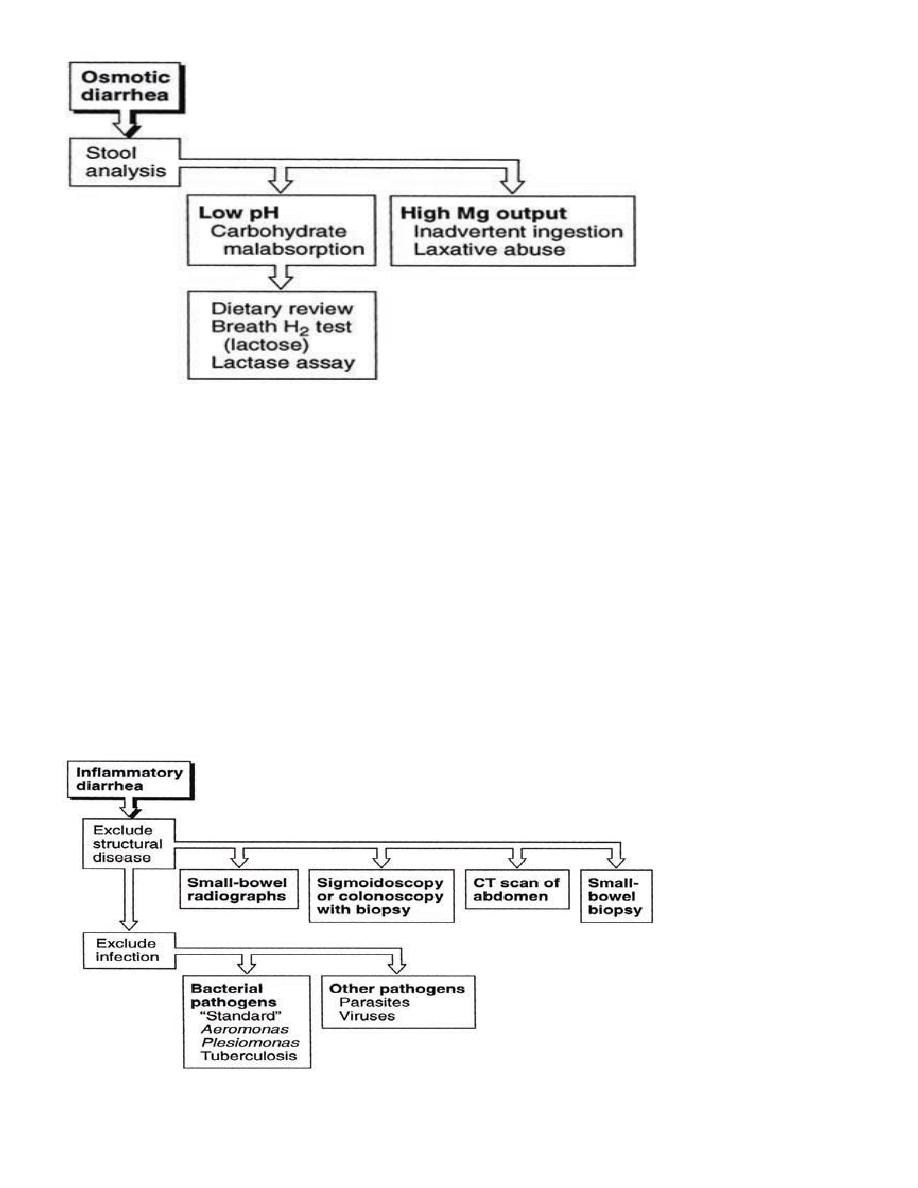
Evaluation of Chronic Inflammatory Diarrhea
Mucosal disruption and inflammation (white blood cells or blood in stools)
are classified as having inflammatory diarrhea.
Diagnostic considerations include IBD, infections, ischemia, radiation
enteritis, and neoplasia.
Colonoscopy ( with T.ileum intubation)should be considered.
Infection needs to be considered as C. difficile, cytomegalovirus, amebiasis,
and tuberculosis.
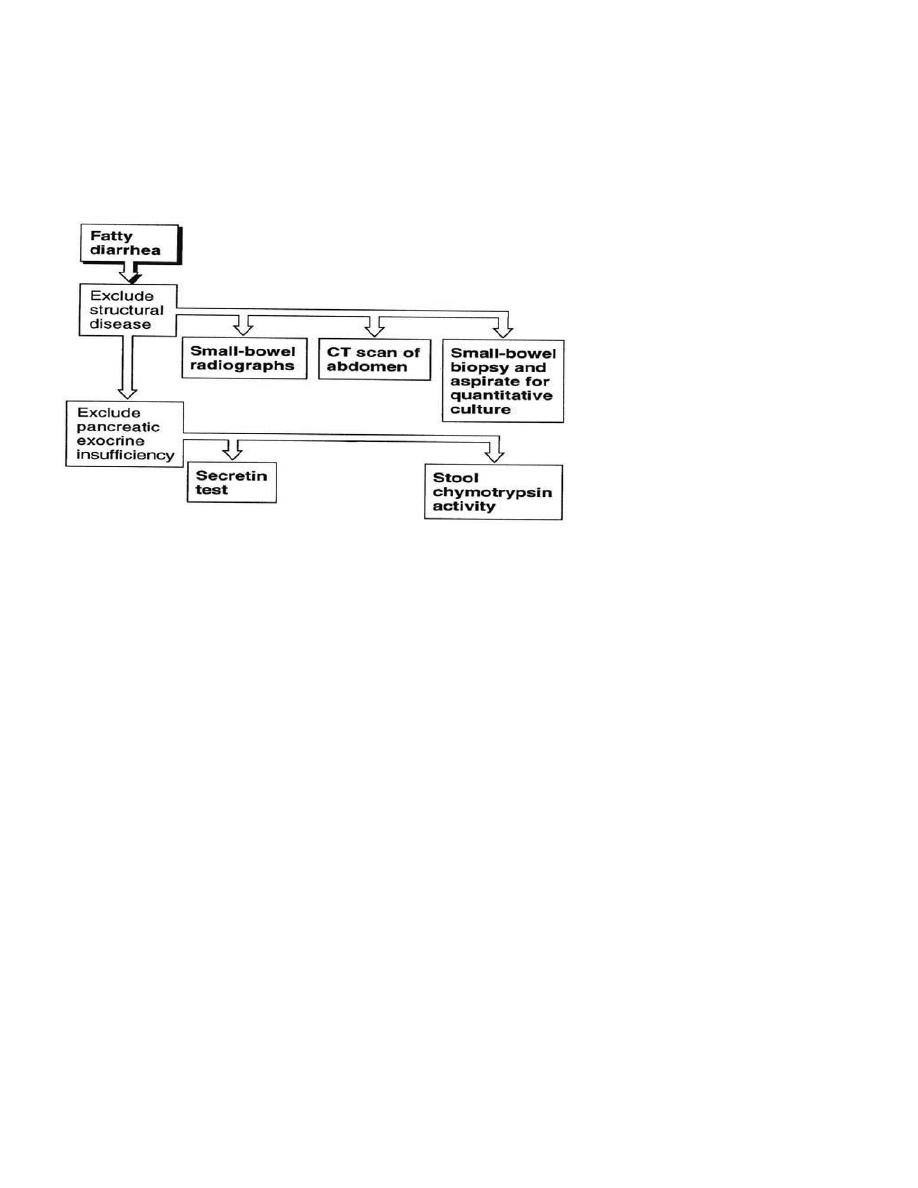
Evaluation of Chronic Fatty Diarrhea
▪ 24 hrs. fecal fat of 7–14 g provided that daily fat intake of 100g is consider
abnormal.
▪ Sudan stain of a fecal smear.
Treatment of Diarrhea
The most important therapy is replacement of any fluid and electrolyte
deficits.
Empirical Therapy of Acute Diarrhea:
▪ Antidiarrheal agents Opiates such as loperamide or diphenoxylate with
atropine.
▪ Antibiotics or antiprotozoal
Empirical Therapy of Chronic Diarrhea
▪ Empirical antibiotic therapy generally is less useful than in acute diarrhea.
▪ Potent antidiarrheal opiates, such as codeine, opium, or morphine.
▪ Therapeutic trials of bile acid-binding resins in idiopathic secretory diarrhea .
▪ Pancreatic enzyme replacement in unexplained steatorrhea have been
discussed previously.
▪ Octreotide, a somatostatin analog, is of proven value in the treatment of
some forms of diarrhea