1
2
3
Lec:11
Psychology
Arousal
Arousal:
Is a state of being excited or alarmed or the establishment & maintenance of an awake
state which involve a complex mechanism (mental& physical) ,that prepare the organism to
deal with emergency situation & danger.
The electrophysiological studies showed that both the thalamus & the cortex fire
rhythmical burst of neuronal activities at a rate of 20-40c/s .During sleep the bursts are
slow & not synchronized ,the higher the synchronization the higher the level of
wakefulness.
Stupor or coma indicates absence of arousal.
Intense emotion usually involves physiological arousal caused by the activation of the
sympathetic division of the autonomic nervous system that manifest by:
o Rapid heartbeat & increased blood pressure.
o Rapid breathing.
o pupil dilate
o Dryness of mouth & throat
o Feeling weak & even faint with sinking feeling in the stomach.
o excessive sweating
o trembling
o poor concentration
o blood sugar level increases
As the emergency situation subside the parasympathetic take overall these activities are
triggered in the brain in the Limbic system.
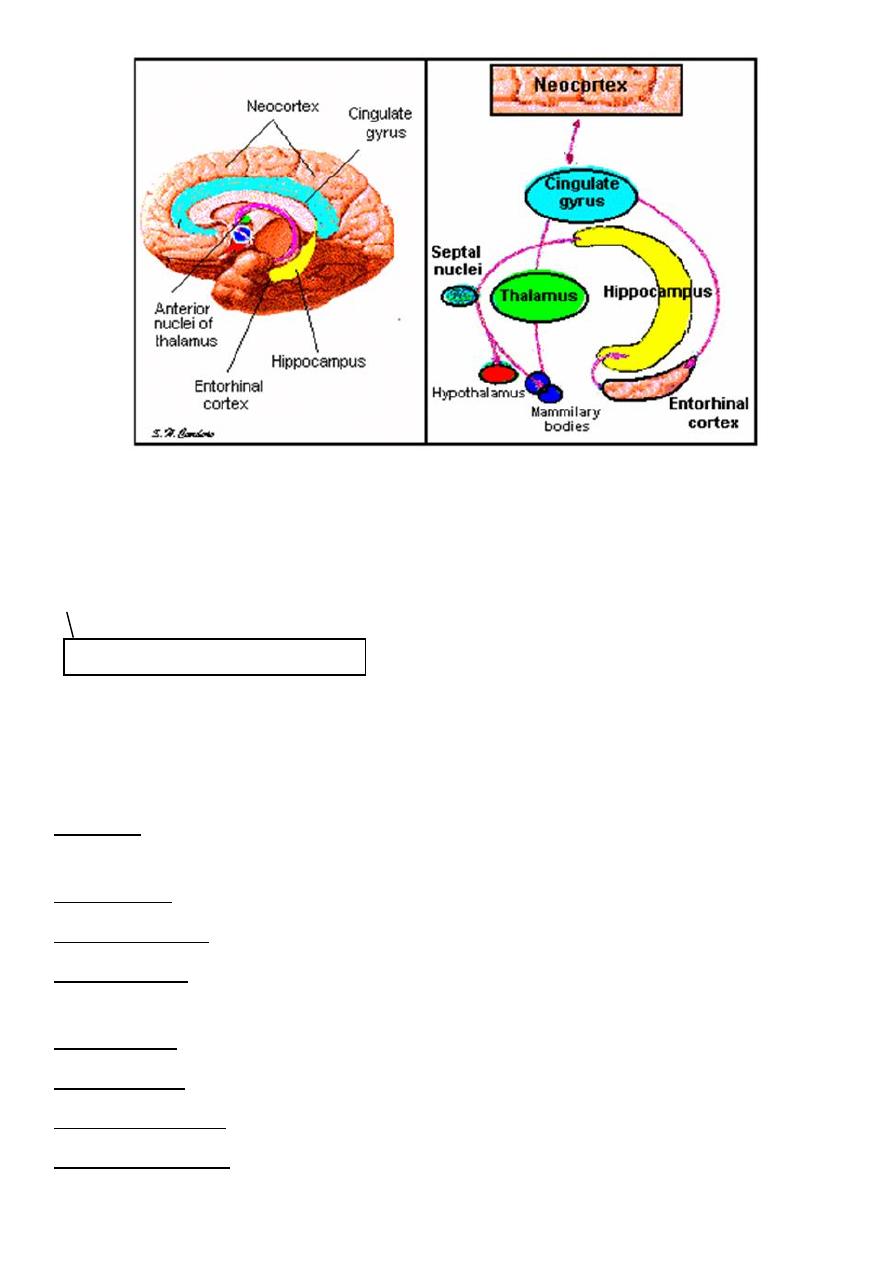
Definition of the limbic system:
Is the neuronal circuit that controls the emotional behavior, drive &motivation.
Important: definition
Important: all
4
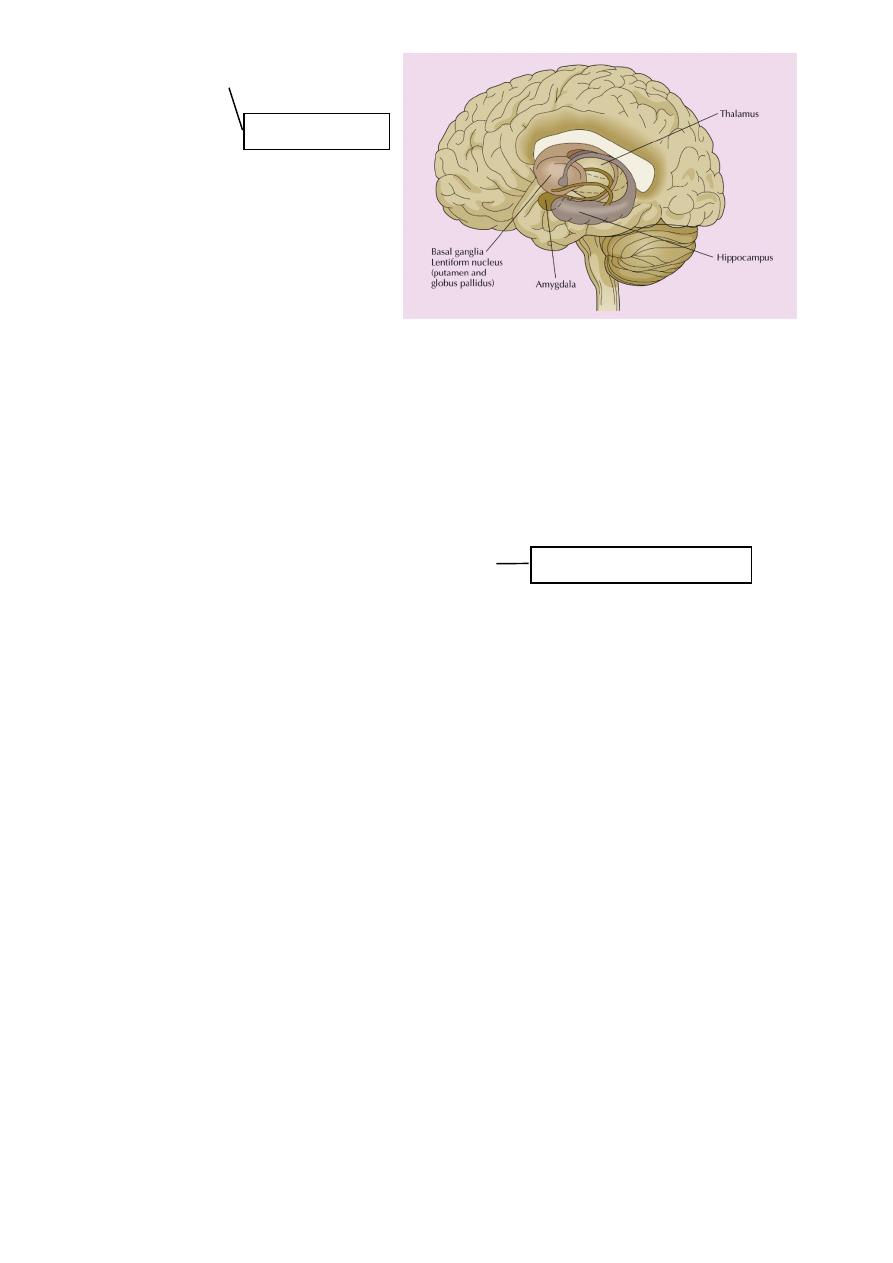
The limbic system: is a set of brain structures including the hippocampus, amygdala,
anterior thalamic nuclei, septum, limbic cortex and fornix, which seemingly support a
variety of functions including emotion, behavior, long term memory, and olfaction
The limbic system is the set of brain structures that forms the inner border of the cortex
Hippocampus and associated structures:
Required for the formation of long-term memories and implicated in maintenance of
cognitive maps.
Amygdala: Involved in signaling the cortex of motivationally significant stimuli such as those
related to reward and fear in addition to social functions such as mating.
Fornix carries: signals from the hippocampus to the mammillary bodies and septal nuclei.
Mammillary body: Important for the formation of memory;
Cingulate gyrus: Autonomic functions regulating heart rate, blood pressure and cognitive
and attentional processing
Dentate gyrus: thought to contribute to new memories and to regulate happiness.
Piriform cortex: The function of which relates to the olfactory system.
Nucleus accumbens: Involved in reward, pleasure, and addiction
Orbitofrontal cortex: Required for decision making.
Important: definition & content
5
Function of limbic system
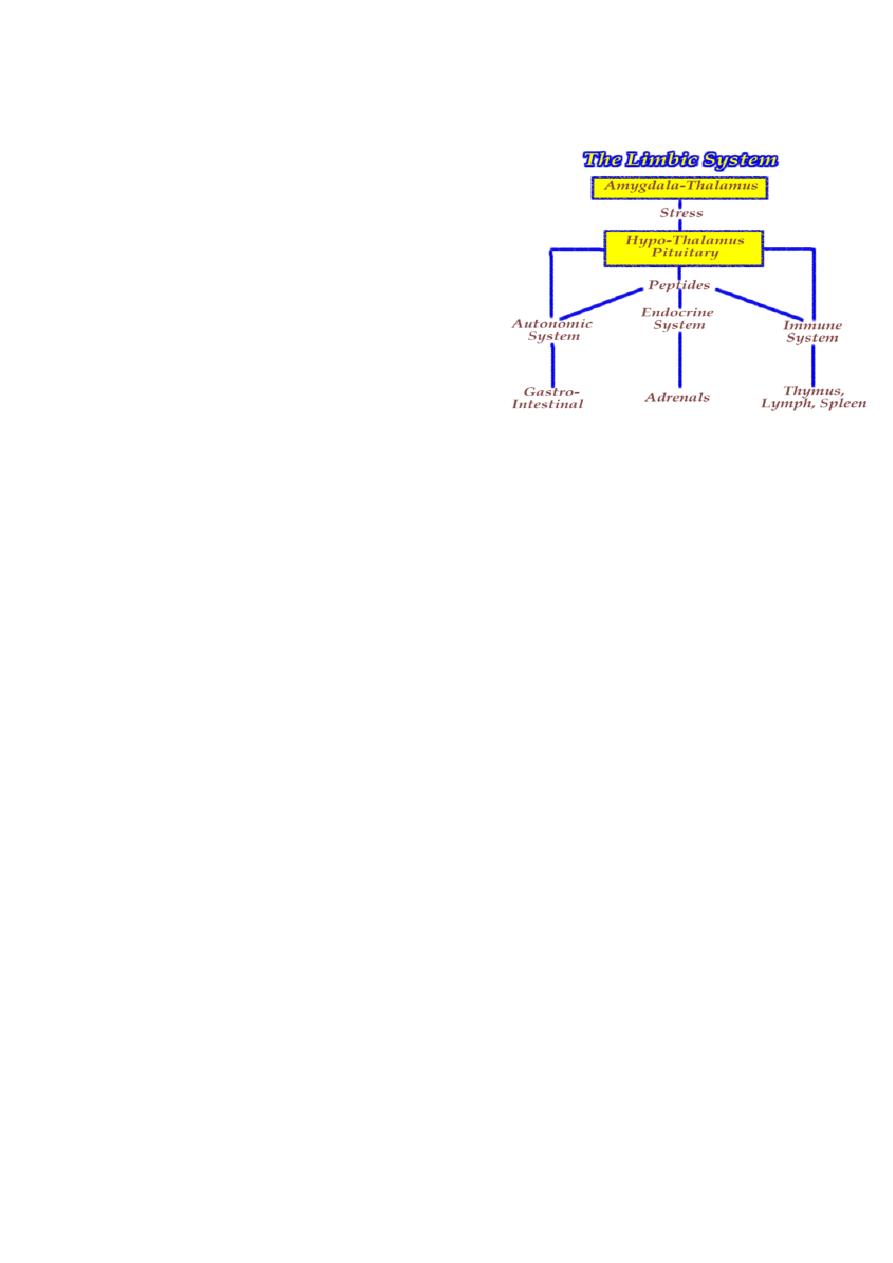
Limbic System: The Center of Emotions
The limbic system operates by influencing the endocrine system and the autonomic
nervous system. It is highly interconnected with the nucleus accumbens, the brain's
pleasure center, which plays a role in sexual arousal and the "high" derived from certain
recreational drugs. These responses are heavily modulated by dopaminergic projections
from the limbic system. The limbic system is also tightly connected to the prefrontal cortex.
Some scientists contend that this connection is related to the pleasure obtained from
solving problems. To cure severe emotional disorders, this connection was sometimes
surgically severed, a procedure of psychosurgery, called a prefrontal lobotomy (this is
actually a misnomer). Patients who underwent this procedure often became passive and
lacked all motivation
Emotion involves the entire nervous system, of course. But there are two parts of the
nervous system that are especially significant: The limbic system and the autonomic
nervous system .
One of its most important effects is causing the adrenal glands (which sit on top of the
kidneys) to release epinephrine (aka adrenalin) into the blood stream. Epinephrine is a
powerful hormone that causes various parts of the body to respond in much the same way
as the sympathetic nervous system. Being in the blood stream, it takes a bit longer to stop
its effects. This is why, when you get upset, it sometimes takes a while before you can calm
yourself down again !
The sympathetic nervous system also takes in information, mostly concerning pain from
internal organs. Because the nerves that carry information about organ pain often travel
along the same paths that carry information about pain from more surface areas of the
body, the information sometimes get confused. This is called referred pain, and the best
known example is the pain some people feel in the left shoulder and arm when they are
having a heart attack.
The other part of the autonomic nervous system is called the parasympathetic nervous
system. It has its roots in the brainstem and in the spinal cord of the lower back. Its
function is to bring the body back from the emergency status that the sympathetic nervous
system puts it into some of the details of parasympathetic arousal include...
o pupil constriction
o activation of the salivary glands
o stimulating the secretions of the stomach
o stimulating the activity of the intestines
o stimulating secretions in the lungs
o constricting the bronchial tubes
Important: only this sentence
6
o decreasing heart rate
The parasympathetic nervous system also has some sensory abilities: It receives
information about blood pressure, levels of carbon dioxide in the blood, and so on.
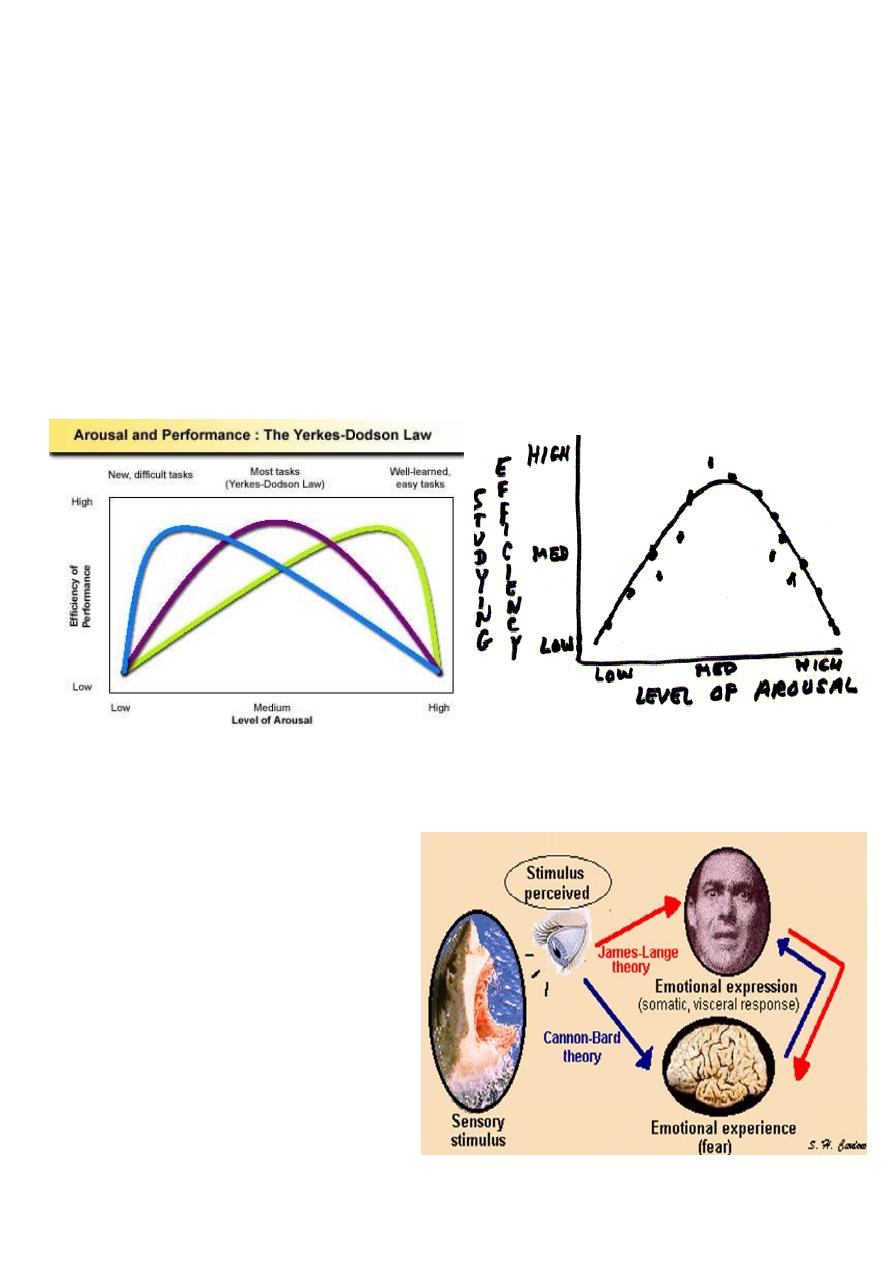
The Inverted-U Theory:
The inverted U theory has been around for as long as the arousal/performance relationship
has been studied. It simply states that the relationship between performance and arousal is
curvilinear as opposed to linear, and takes the form of an inverted-U. It seems relatively
clear that the nature of the relationship between athletic performance and arousal takes
the form of the inverted U, it is not clear why this occurs.
Drive Theory
The great contribution of drive theory is
that it helps to explain the relationships
between learning and arousal, and
between performance and arousal. Many
young athletes are just beginning the
process of becoming skilled performers.
The effect of arousal upon a beginner
may be different from its effect upon a
skilled performer
7
Lec:12
Psychology
Stress and Coping
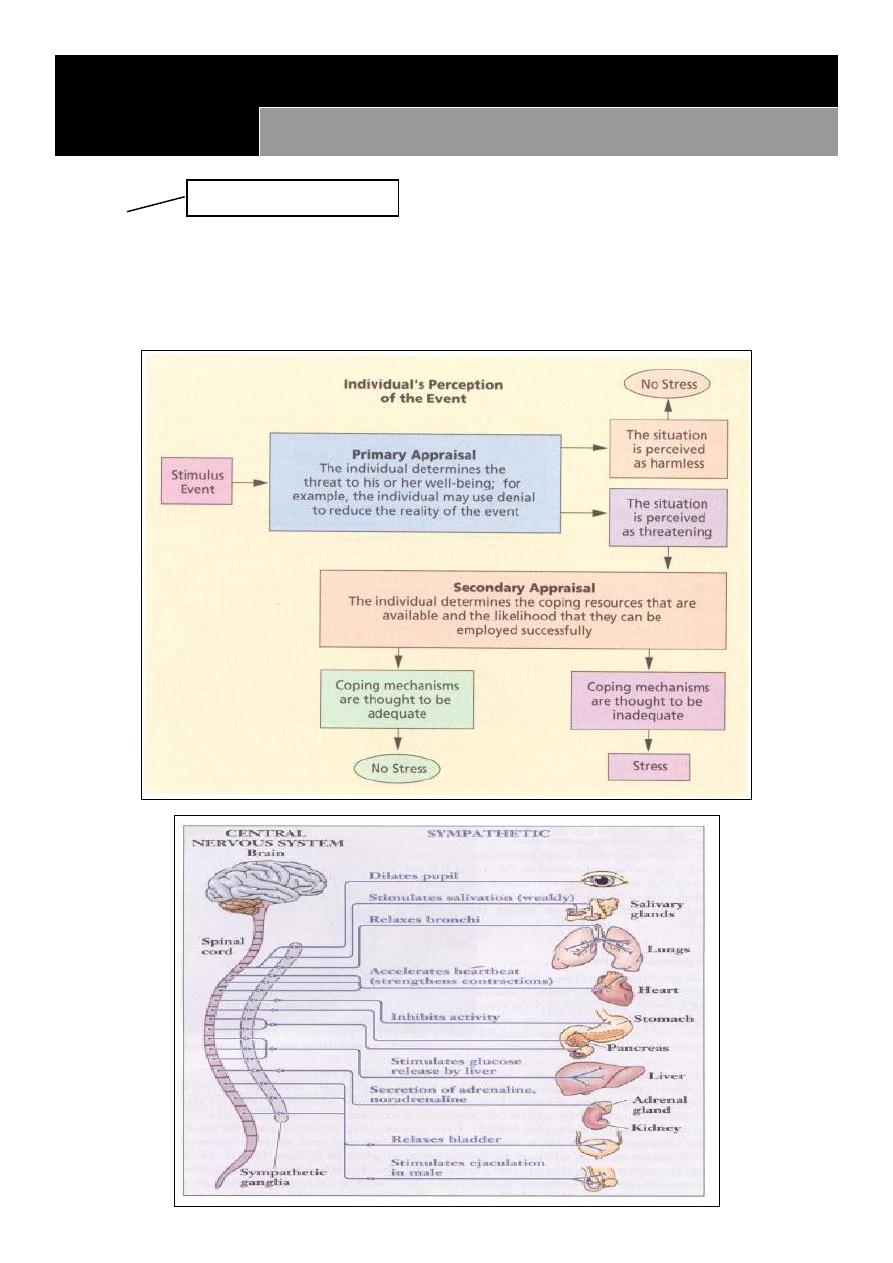
Stress:
A state of physical and/or psychological arousal
Often brought about by a perceived threat or challenge
May be expressed differently by different cultures
Important: definition

8
Stress Reaction Phases:
1. Acute phase Lasts minutes, hours or days
2. Reaction phase Lasts one to six weeks
3. Repair phase Lasts one to six months
4. Reorientation phase Approximately six months after a distressing event & continuing
Acute Phase
Lasts minutes, hours or days
“Fight or flight” response: preparation for physical activity
Narrowing of focus: decreases ability to think properly
Emotional reactions: disbelief/consternation/fear/grief
Rigid behavior: irritability, anger, etc. affects communication
Panic is rare but if present, requires immediate attention
Reaction Phase
Lasts one to six weeks
Delayed reactions: previously repressed or denied feelings will surface
May be overwhelming, bringing feelings of powerlessness
Reaction Phase: Characteristic reactions:
Fear of returning to the site of the event
Dreams or nightmares
Anxiety, restlessness, insomnia
Muscular tension, tremors and exaggerated startle response
Increased irritability and isolation, depression
Disturbing thoughts about survival, relief, guilt and grief
Perceived images of how others suffered in the disaster, i.e. how they died, how they
injured
Repair Phase
Lasts one to six months
Reactions are less intense, and not so overwhelming
o Feelings of hurt continue, but are more manageable
Important: enumerate and time
9
o Renewed interest in everyday life
o Makes plans for the future
Reorientation Phase
Approximately six months after a distressing event and continuing
Heightened stress reactions are substantially reduced
o Grief reaction may not be resolved but is accepted
o Most reactions will diminish gradually
Assessing ongoing needs is important
Coping with Stress
Coping is a way to prevent, delay, avoid, or manage stress
Coping mechanism categories:
o Changing the source of stress
o Changing the view of the situation
o Tolerating the stressor until it passes or becomes less troublesome
Loss and Grief
Loss is a common theme in most disaster settings
Common reactions to loss:
o Denial, numbness or shock
o Bargaining
o Depression
o Anger
o Acceptance
o Reorientation
Loss and Grief – Signs of Trouble
Avoiding or minimizing emotions
Using alcohol or drugs to self-medicate
Using work or other distractions to avoid feelings
Hostility and aggression toward others
Important: all
11
Emotional Numbness or Extreme Agitation
Immediate attention is needed
Possible referral for professional care
When referring:
o Inform the person of your intention
o Recognize that the referral may cause a negative reaction
Guiding Principles in Providing Psychological Support
First protect from danger
Focus on physical and material care
Be direct, active and remain calm
Focus on the “here and now” situation
Provide accurate information about the situation
Assist with mobilization of resources
Do not give false assurances
Recognize the importance of taking action
Reunite with family members
Provide and ensure emotional support
Focus on strengths and resilience
Encourage self-reliance
Respect feelings and cultures of others
Crisis Intervention
Observe safe practices by showing concern for your own safety
Remain calm and appear relaxed, confident and non-threatening
Crisis Intervention Steps
1. Assess the situation
2. Establish rapport
3. Identify the main problem (s)
4. Deal with feelings and emotions
5. Generate and explore alternative coping strategies
6. Formulate an action plan
7. Follow up
Important: definition
11
Lec:13
Psychology
Illness behavior
Illness behavior (sick role)
Illness behaviour refers to those behaviours that individuals engage in once they believe
that they are ill.
“It is not the symptoms themselves that are significant in comprehending illness behaviour,
but the way in which they are defined.”
Sick Role:
A form of behaviour deemed appropriate to those perceived as being encumbered by
illness
Comprises regulatory features that control the “deviant behaviour” of illness thereby
preventing disruption of societal stability & cohesiveness (i.e. “The Social Order”).
The social community determines whether we can legitimately consider ourselves as ill.
We influence the social community’s decision by how we present and behave.
In sociology, the “sick role” is a term used to describe the social behaviors exhibited
both by people who are sick and the people around them.
The term “sick role” was coined by researcher Talcott Parsons in the early 1950s. Since
then, a number of people have built on Parsons' work to explore the role played in
society by people who are ill as well as the experiences of people who are sick.
Benefits of sick role:
Ability to gain exemption from normal roles e.g. employment, domestic work
Societal relinquishment of perspective that individuals concerned are responsible for
their illness and predicament
Obligations under the sick role theory:
People who are sick are expected to get better,
work on getting better by going to the doctor,
complying with medication regimens, and cooperating with treatment plans
Being sick can,
Come with loaded social responsibilities and burdens.
Important: all

12
The sick role can also be involved in social perceptions of disability and disabled persons.
For example, many people believe that people with mental illness should adhere to
prescribed medications in order to be functional members of society or to be entitled to
receive benefits,
Illness perception might reflect cultural beliefs, psychological needs, or something else that
may have little to do with measurable disease.
Factors influencing individual response to illness
Symptom visibility & perceived importance of this
Assessment of symptom’s significance
Potential for symptoms to disrupt community
Symptom denial for fear of confirmation of serious illness
Deferring response to symptoms because of competing social demands
Assessment of social & economic costs of responding to symptoms versus potential
health-related benefits
Available information knowledge & cultural assumptions & understandings
Symptom frequency & persistence
Competing interpretations of symptoms
An understanding of a patient’s illness perception is necessary to help in a diagnosis. This
can be difficult because perception is highly subjective, and there's no absolute method of
measuring it, either from individual to individual, or even within one person’s perspective
through time. Researchers have determined that reducing illness perception to its most
basic elements can help patients describe what it is they are feeling. By organizing these
components into a structure, patients can reconstruct the architecture of their beliefs
about their illnesses
The first area of focus is identity. This component contains what the patient believes is true
of the disease, including cause and symptoms. A patient who lists a number of experiences
such as confusion, nausea, and anxiety as symptomatic of a particular disease may be more
likely to experience those symptoms while simultaneously failing to recognize others that
are just as likely to be part of the cluster.
The patient’s sense of timeline describes the third component. This area is concerned with
the perceived illness’s initial appearance, its trajectory, and its conclusion. Patients with the
illness perception that a sickness is or will become chronic are less likely to recover from it
quickly than those who believe it is temporary.
Those scoring highest on Optimism Scale tend to be:
More successful
Healthier

13
Improve under pressure
Endure stress better
Live longer
Importance of habitual patterns of subjective beliefs about the causes of events
(“explanatory style”)
The fourth area of concern is consequences. Patients whose illness perception leads them
to believe that it will have a profound and negative effect on the quality of life are more
likely to become discouraged or depressed than those who don’t have this particular
perception. Patients who, in fact, do have a serious disorder but lack a strong sense of
consequences might be better able to fight it or less equipped to handle the effects.
The final category is cure-control. This element of illness perception is concerned with the
degree to which the patient believes a cure is possible. This can range from a fully negative
position in which there is no hope of a cure to a fully positive one, in which the patient
firmly believes a cure will be found.
The general idea is that the individual who has fallen ill is not only physically sick, but now
adheres to the specifically patterned social role of being sick. ‘Being Sick’ is not simply a
‘state of fact’ or ‘condition’, it contains within itself customary rights and obligations based
on the social norms that surround it. The theory outlined two rights of a sick person and
two obligations:
Rights:
o The sick person is exempt from normal social roles
o The sick person is not responsible for their condition
Obligations:
o The sick person should try to get well
o The sick person should seek technically competent help and cooperate with the
medical professional
There are three versions of sick role: 1. Conditional 2. Unconditionally legitimate 3.
Illegitimate role:
condition that is stigmatized by others
Rejecting the sick role.
o This model assumes that the individual voluntarily accepts the sick role.
o Individual may not comply with expectations of the sick role, may not give up social
obligations, may resist dependency, may avoid public sick role if their illness is
stigmatised.
o Individual may not accept ‘passive patient’ role.
Doctor Patient relationship
o Going to see doctor may be the end of a process of help seeking behavior

14
o , importance of 'lay referral system'- lay person consults significant lay groups first.
o This model assumes 'ideal' patient and 'ideal' doctor roles).
o Differential treatment of patient, and differential doctor patient relationship-
variations depend on social class, gender and ethnicity.
Blaming the sick.
Blaming the sick.
o ‘Rights’ do not always apply.
o Sometimes individuals are held responsible for their illness, i.e. illness associated
with sufferers lifestyle. (Alcoholism).
o In stigmatised illness sufferer is often not accepted as legitimately sick.
Chronic Illness.
o Model fits acute illness (measles, appendicitis, relatively short term conditions).
o Does not fit Chronic/ long-term/permanent illness as easily, getting well not an
expectation with chronic conditions such as blindness, diabetes.
o In chronic illness acting the sick role is less appropriate and less functional for both
individual and social system.
o Chronically ill patients are often encouraged to be independent.
Factors that determine the type of illness behavior expressed in the individual.
o age and gender in illness behavior
o Far greater in women .
o variation to ethnicity s
o education,
o family structure, and social networks
o Health care coverage and insurance.
o Socioeconomic status.
o Lower-class individuals (lower in socioeconomic status) most likely to delay seeking
professional health care even when presented with severe symptoms.
Treatment & Management Beliefs
o Do less
o Avoid exercise
o Rest
o Avoid academic work
o Exercise more & do more
o “The exploration of a patient’s biography is an important strategy in establishing a
successful working relationship.”
15
Lec:14
Psychology
Patient doctor relationship
Physician’s Responsibilities:
Freedom of choice
Responsibility to improve community
Responsibility to patient is paramount
Must support access to medical care for all people
Human dignity
Honesty
Responsibility to society
Confidentiality
Continued study
Patient's rights:
Right to give informed consent
Right to privacy
Right to be informed of advantages and potential risks of treatment
Right to refuse treatment
Right to confidentiality
Privileged communication
Expectations:
Patient expects from doctor:
o A cure
o Medication
o To be listened to
o Sympathy
o Advice- he understands
o The ‘answer’
o A sick note
o What they want (agenda)
o Comfort
o A chat
o No harm
Important: all
Important: all
Important: all

16
o Professionalism & Respect
o To be told what to do
o To feel better
o The truth
Why a patient goes to doctor:
o They feel ill physically
o They feel ill mentally
o They are lonely
o They want time off work
o Need advice
o Don’t know who to turn to
o Marital/family problems
o Legal reasons
Doctor expects from patient:
Trust
Compliance to treatment
Agreement
The truth
Respect
They want to get better
To be listened to
To obey the ‘Rules’!
Doctor Patient Contacts
The nature of the relationship determines the success or otherwise of the contact
Communication and Diagnosis
Patients who feel at ease and who are encouraged to talk freely are more likely to
disclose the real reason for consultion
Communication and Treatment
Advice, reassurance and support from the doctor can have a significant effect on recovery
(The placebo effect)

17
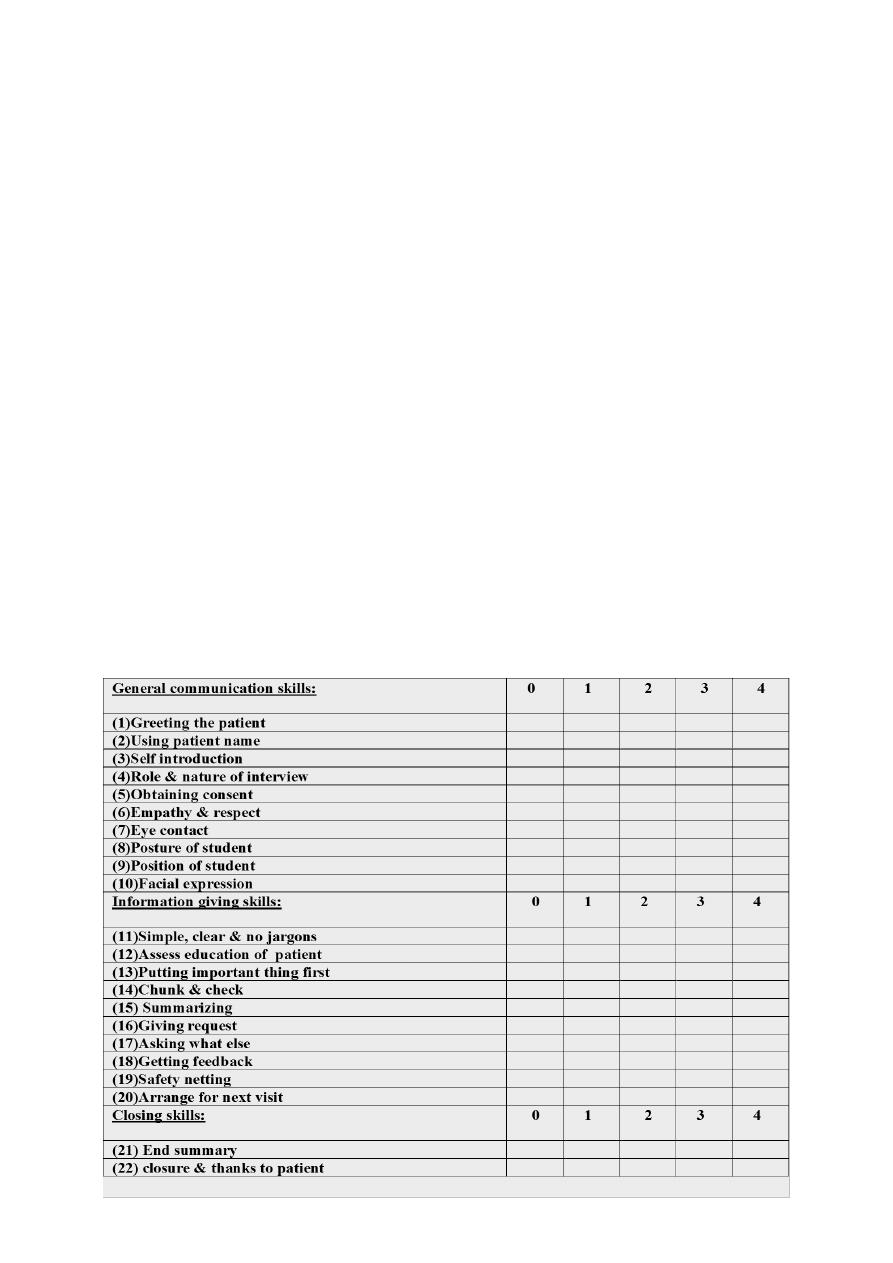
Clinical competence used to include the medical technical knowledge, physical
examination, and medical problem solving.
While the Communication was missing from the list.
It is clear from the literature that better physician communication skills improve patient
satisfaction and clinical outcomes and that good communication skill can be taught and
learned
Patient controlled consultation
“You’re paid to do what I tell you!!”
The Paternalistic Approach
“If I’ve told you once I told you 1,000 times, stop smoking!!”
Paternalism
The traditional D-P relationship
Doctor Takes on role of “parent”
Patient submissive
Doctor centred consultation style:
Paternalistic - doctor is the expert and patient expected to cooperate
Tightly controlled interviewing style aimed at reaching an organic diagnosis.
Patient Centred consultation style
Less authoritarian - encourages patient to their own feelings and concerns
Open questioning, interested in psycho-social aspect of illness
Consultation Styles
It’s serious isn’t it doctor?
Patient centred clinical interview
Doctor –
History examination investigation
Results in a differential diagnosis
Patient –
Ideas, expectations, feelings,
18
Results in an understanding of patient's beliefs
Length of Consultation
Average 8 minutes
Makes patient centred consultation styles more difficult.
Goals of Communication Teaching and Learning
o Doctors with good communication skills identify patients' problems more accurately
o patients are more satisfied with their care and can better understand their problems,
investigations, and treatment options
o patients are more likely to adhere to treatment and to follow advice on behaviour
change
In Conclusion
o Communication techniques are a learned skill. Unfortunately, many health care
providers discover this after an adverse event occurs. If this is the case in your facility,
turn that negative experience into a positive teaching tool by asking these questions:
o What can we learn from this?
o How can we prevent a recurrence?
o Is there anything we can do now to alleviate the situation?
19
Lec:15
Psychology
Thinking
Thinking
Thinking represent many most complex form of behavior, the highest of mental activity
The important of thinking is the use of symbol theses symbol may be a word, images,
movement, mathematical symbol or others.
The use of language i.e. verbal symbols.
Mans ability to use symbol is only characteristic of his thinking, he organize the information
into pattern this is called Concept formation.
-
Generalization.
-
Abstract.
The whole process of generalization and abstract is called Concept formation and this is the
mechanic of thinking.
Problem solving behavior:
We use thinking in problem solving behavior the classical is reported by Dunker ex.
The Effect of previous Experience
:
The extend to which previous experience could affect thinking done by many reserches,
one of these done by Main, he set groups of subject, the 1
st
group had no previous
experience he gave them an apparatus to construct from many component find difficulty to
Important: definition of abstract
Important: definition of concept
21
solve the problem while the 2
nd
group who had previous experience find no any difficulty to
construct the apparatus.
Bodily process in thinking:
We are completely inactive physically is thinking out problem, but it has shown certain
bodily processes accompany thinking, there is muscular movement are involved in mental
process
During thinking certain recordable nervous and muscular changes occur even although they
are not apparent either to the thinker or to the observer and this can be recorded by EMG
and EEG.
Autistic thinking: it is a fantasy thinking, this may be adjustment to intorable situation
excessive fantasy thinking occur in schizophrenia and in normal people.
Primary and Secondary process in thinking:
-Primary process are these which dominate in infancy and children ch. By immature,
primitive tendency to immediate gratification of basic instinctual drive or needs.
- Secondary process are more mature and directed way of thinking, here the instinctual
impulses can be controlled or delayed or substituted by another form of gratification.
Thought Disorder
1. Disorder of the stream of thought:
o Inhibition of thought. {Depression}
o Pressure of thought. {mania or schizophrenia}
o Flight of Ideas. {mania}
o Thought Blocking. {schizophrenia}
o Incoherence of Thought {schizophrenia}
o Circumstantial pressure of talk. {mania or schizophrenia}
o Preservation- speech disorder. {dementia}
2. Disorder of the Content of Thought:
o Delusion – A fixed false unchable belief is out of keeping with person educational and
cultural background, not shared by others.
o An over – valued idea- an idea that because of its feeding tone takes precedence
overall other ideas, it may be true or false.
Important: all
Important: all
21
Types of delusion according to content
1. Paranoid Delusion.
2. Hypochondriacal delusion.
3. Delusion of guilt
4. Delusion of poverty
5. Nihlistic delusion
6. Grandiose delusion.
7. Persecutory delusion.
8. Ideas of self-reference.
9. Primary and secondary delusion.
3. Disorder of the form of thought:
o Negative formal thought.
o Positive formal thought Disorder (No abstract thinking).
o Neologisms.
o Self –reference of thinking.
o Talking past the point ( here the pt. gives a worong answer
4. Disorder of possession of thought
o Here the individual is compelled to think his own thought against his will.
1. Obsessional thought cun be classified into:-
a. Obsessional ideas or mental images.
b. Obsessional impulses.
c. Obsessional phobias.
d. Obsessional Ruminations.
Obsessions may occur in obsessional neurosis, in depression, in schizophrenias, and
organic states.
2. Alienation of thought –this takes three forms:-
a. Thought withdrawal
b. Though insertion.
c. Thought broadcasting
Important: all
Important: all
Important: all

22
23
Lec:16
Psychology
Memory
Three-Stage Model of Memory
Forgetting and Memory
Problems with Memory
Memory Improvement
Memory is the ability to code, store and retrieve information
Memory involves coding the input of the senses (visual, auditory)
Memory is rarely perfect
Forgetting refers to memory failure
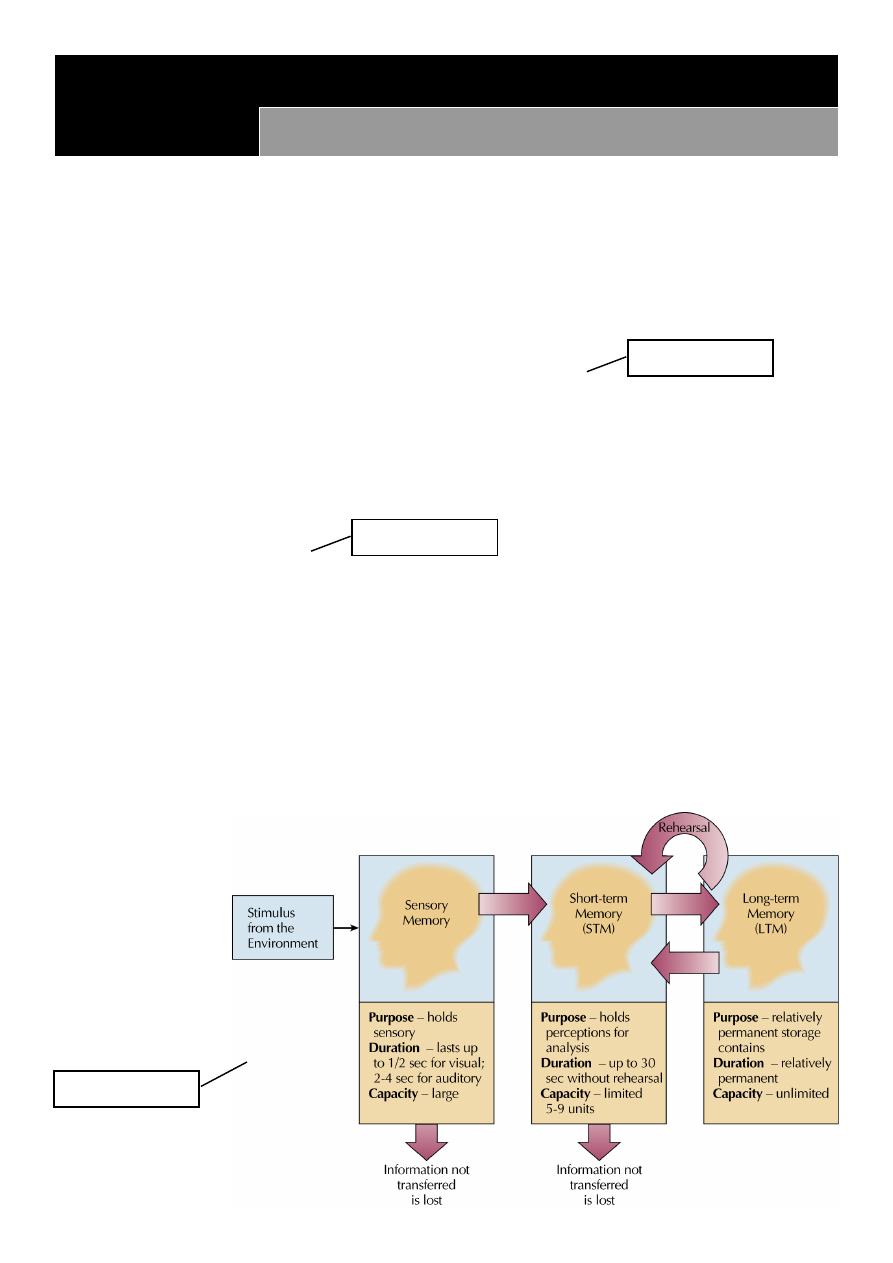
Three Stages of Memory:
Sensory Memory is a brief representation of a stimulus while being processed in the
sensory system
Short-Term Memory (STM) is working memory
o Limited capacity (7 items)
o Duration is about 30 seconds
Long-Term Memory (LTM) is large capacity and long duration
Overview of
Memory Model:
Important: all
Important: all
Important: all
24
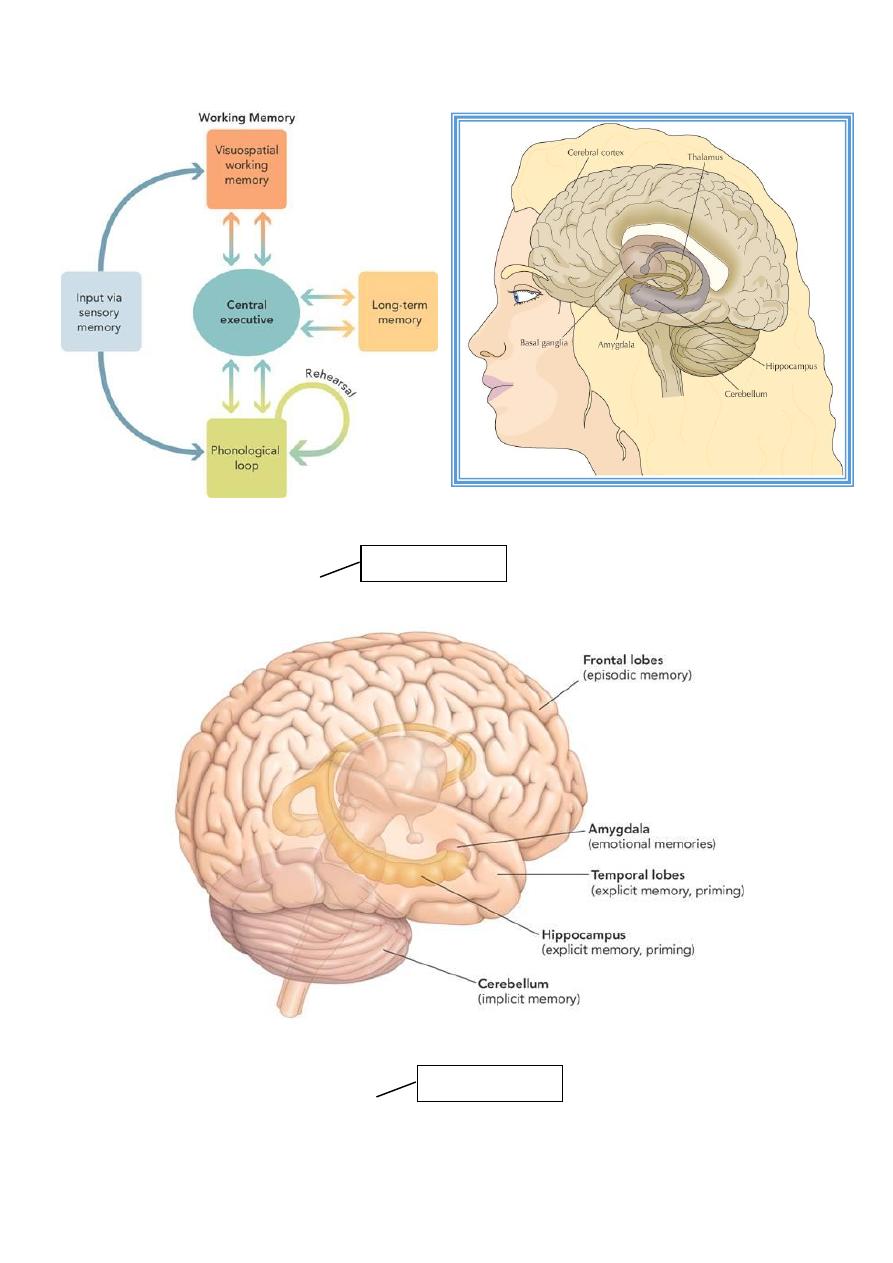
Working Memory Model:
Memory: Brain Structures
Where Are Memories Located?
Memory tends to be localized and distributed throughout the brain--not just the cortex.
Important: all
Important: all
25
Why Do We Forget? Five Key Theories
Decay
Interference
Motivated Forgetting
Encoding Failure
Retrieval Failure
Five Theories of Forgetting:
1. Decay Theory: memory degrades with time
2. Interference Theory: one memory competes (interferes) with another
– Retroactive Interference (new information interferes with old)
– Proactive Interference (old information interferes with new)
3. Motivated Forgetting: motivation to forget unpleasant, painful, threatening, or
embarrassing memories
4. Encoding Failure: information in STM is not encoded in LTM
5. Retrieval Failure: memories stored in LTM are momentarily inaccessible (tip-of-the-
tongue phenomenon)
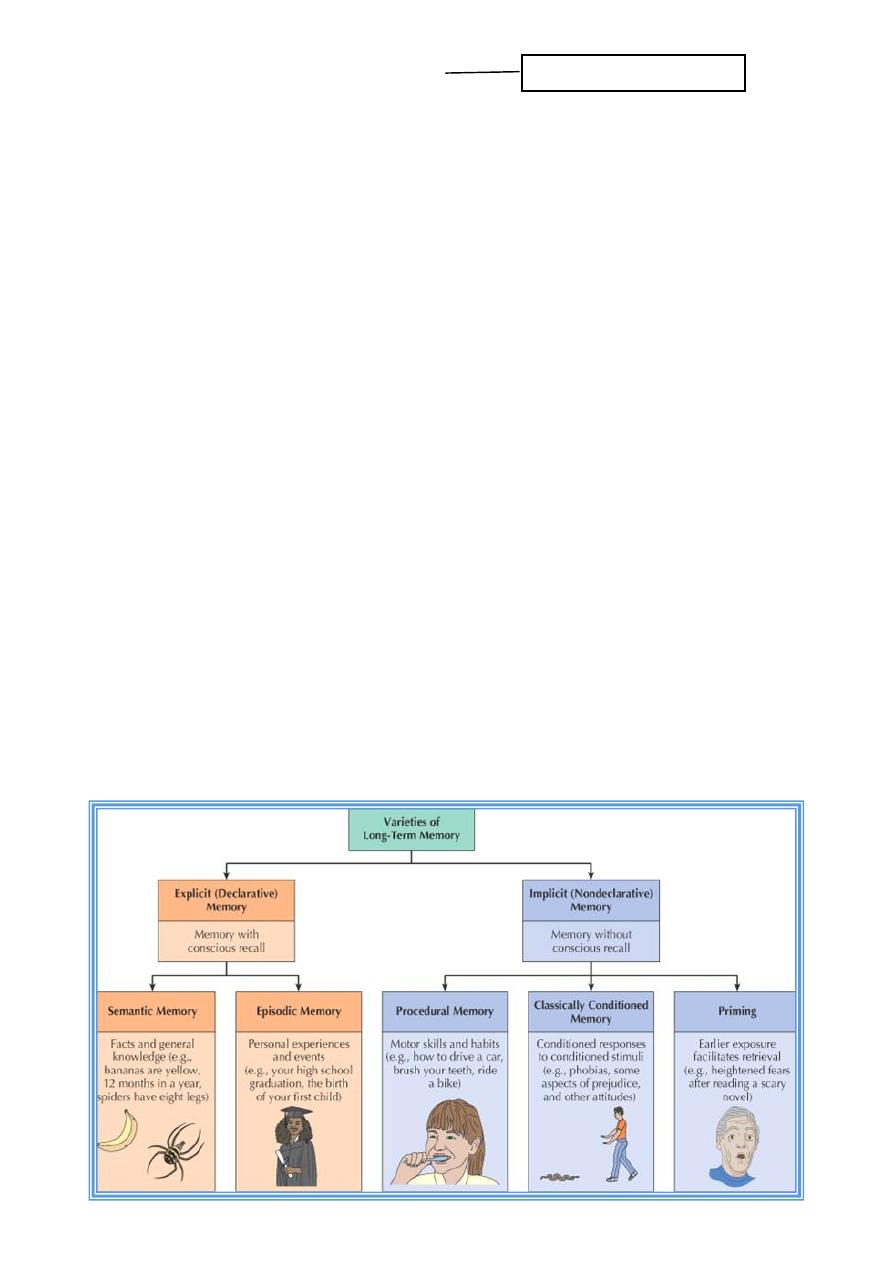
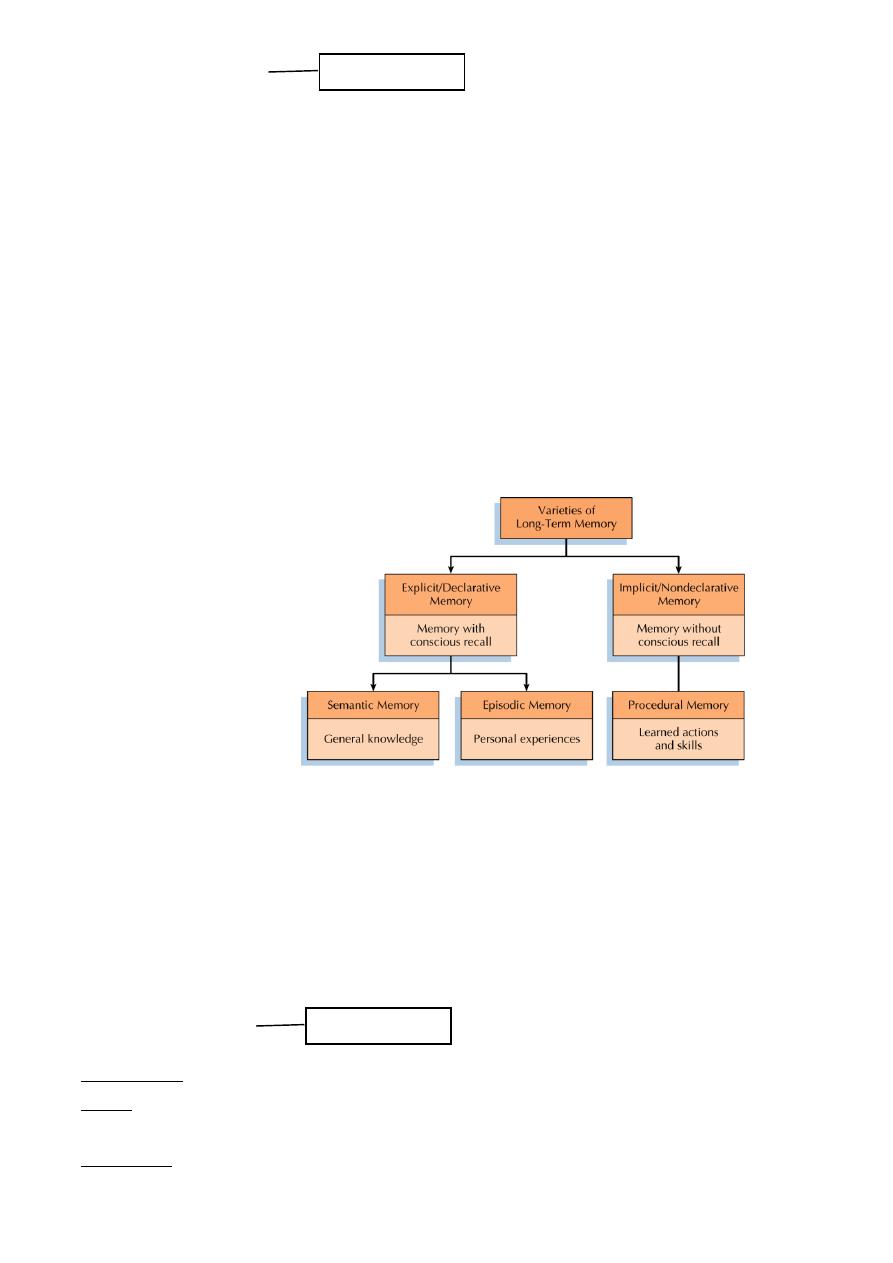
Types of Long-Term Memories:
Important: enumerate
26
Long-Term Memory:
Information transferred from STM to LTM is coded into categories and stored in terms of
meaning
REM sleep may play a key role in categorizing new items within LTM
Memories retrieved from LTM are not an exact replica of the original event
Memories are reconstructed and can be altered during the retrieval process
Varieties of LTM:
Psychologists distinguish between two types of LTM
Semantic memory refers to factual information (What is the capital of Georgia?)
Episodic memory refers to autobiographical information as to where and when an event
happened
“I remember visiting the capital of of Georgia”
Overview of LTM:
Organization of LTM:
Items in LTM are organized in categories that form a hierarchy with multiple paths (direct
and indirect) to each item
Sometimes the cues required to recall an item are not sufficient
Tip-of the tongue phenomenon: person can’t easily recall the item, but shows some
recall for its characteristics (“…it begins with the letter ….”)
Memory Measures:
Recognition is when a specific cue (face or name) is matched against LTM
Recall is when a general cue is used to search memory
E.g. define the term “statistical significance”
Relearning refers to a situation in which a person learns material a second time.
Memory is evident in savings of time to relearn the second time versus the first
Important: all
Important: all
27
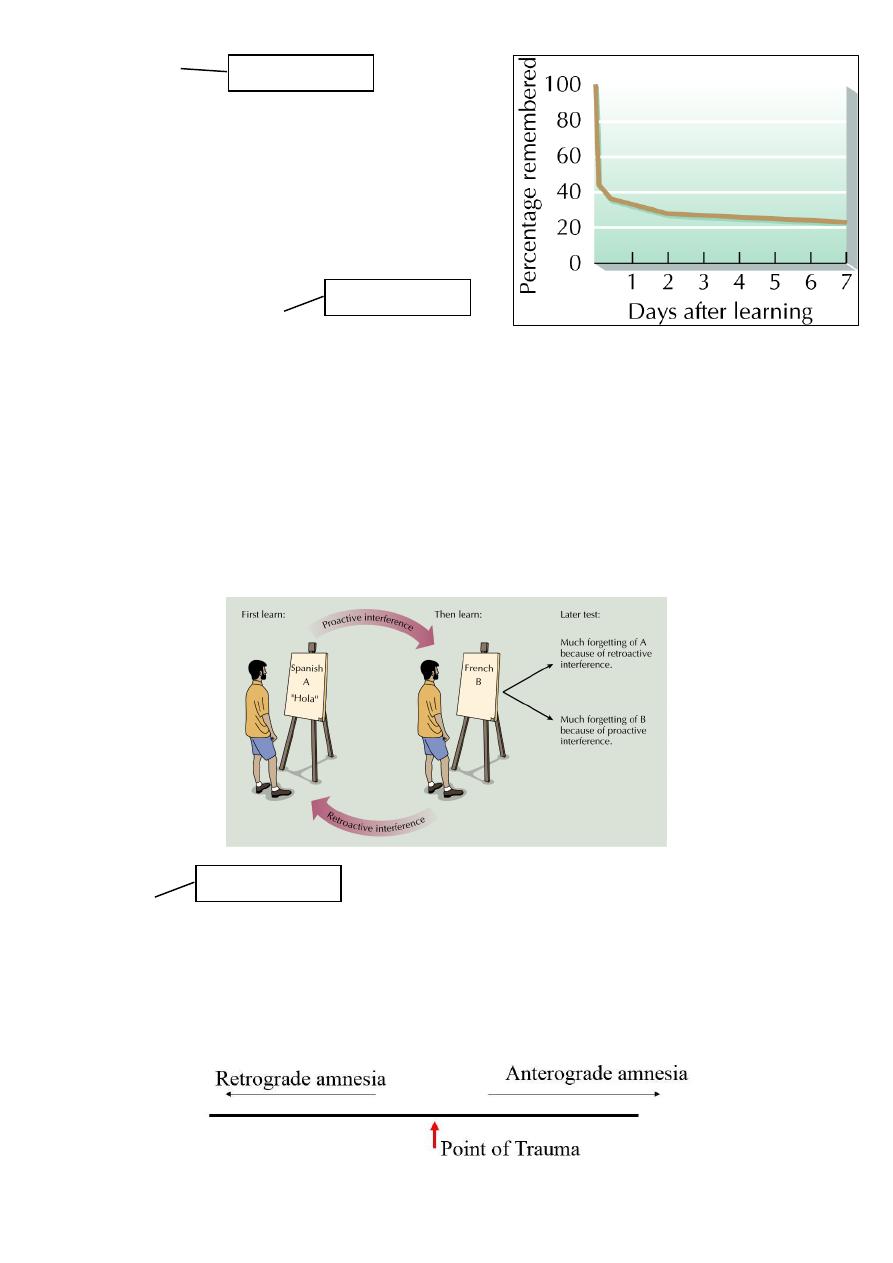
Forgetting:
Forgetting is the inability to recall previously
learned information
Forgetting rate is steep just after learning and
then becomes a gradual loss of recall
Theories of Forgetting:
Interference theory argues that information competes for retrieval
o Proactive interference: old information interferes with recall of new information
o Retroactive interference: new information interferes with recall of old information
Decay theory: memory trace fades with time
Motivated forgetting: involves the loss of painful memories (protective memory loss)
Retrieval failure: the information is still within LTM, but cannot be recalled because the
retrieval cue is absent
Interference and Memory:
Amnesia:
Amnesia is forgetting produced by brain injury or by trauma
Retrograde amnesia refers to problems with recall of information prior to a trauma
Anterograde amnesia refers to problems with recall of information after a trauma
Important: all
Important: all
Important: all
28
Anatomy of Memory:
Bilateral damage to
the hippocampus
results in anterograde
amnesia (Patient H.M.)
Issues in Memory:
Memory recall may involve reconstruction and thus may not be accurate
Reasons for inaccuracy of memory:
o Source amnesia: attribution of a memory to the wrong source (e.g. a dream is recalled
as an actual event)
o Sleeper effect: a piece of information from an unreliable source is initially discounted,
but is recalled after the source has been forgotten
o Misinformation effect: we incorporate outside information into our own memories
Using Psychology to Improve Our Memory:
Eight Tips for Memory Improvement:
1. Pay attention and reduce interference
2. Use rehearsal techniques
3. Organization
4. Counteract serial position effect
5. Time management
6. Use encoding specificity principle
7. Employ self-monitoring and overlearning
8. Use mnemonic devices (e.g., method of loci, peg-word, substitute word, word
associations)
Memory Strategies:
Mnemonic devices are strategies to improve memory by organizing information
o Method of Loci: ideas are associated with a place or part of a building
o Peg-Word system: peg words are associated with ideas (e.g. “one is a bun”)
o Word Associations: verbal associations are created for items to be learned
Other strategies for improving memory:
o Pay attention and avoid interference
o Use rehearsal techniques
o Improve the organization of your memory
o Manage your time
Important: all
Important: enumerate
29
Lec:17
Psychology
Biological basis of behavior (1)
Neuronal activity
Activity in the Central nervous system begins at
the cellular level, with both electrical and
chemical processes. In psychology, we first
study the activity of the central nervous system
at the cellular level.
Biology + environment --------------
behavior
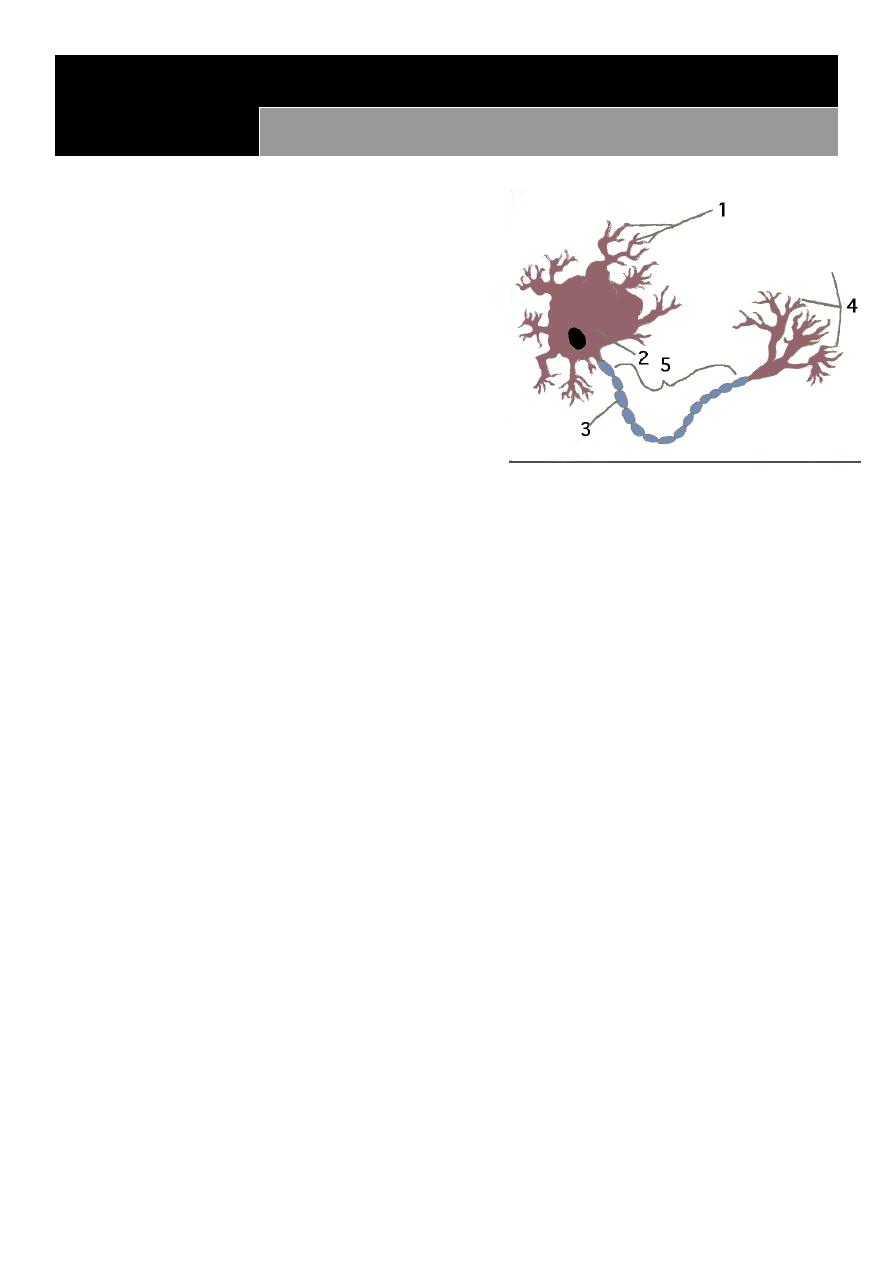
Neurons receive information via the dendrite
and pass information down the axon to the
synapse .
The basic unit of the nervous system,it hold the secret of how the brain work( nature of
consciousness,transmission of impulses ,emotion & thought).
Neurons vary in size,appearance ,neurons of the spinal cord may have an axonof 3-
4ft.long,brain neurons may have few thousands of an inch.
The nervous system in addition to the neurons consist of a large no. of non neuronal
cells =glial(glue)cells which present in a ratio of 9/1(G/N)its function is to hold the
neuron inplace,providing nutrient to neuron,& cleaning of neuronal
environment.Uncontolled proliferation of glial cells is the cause of most brain tumors.
In human brain there is 10bil-1tril.N X9=no. of glial cells!
At the synaptic junction more than70 diff neurotransmitters have been identified.
Action Potential:
Excitatory impulses and inhibitory impulses alter a cells internal potential or charge. When
a cell's potential reaches a certain level, the cell "depolarizes" or becomes positive, causing
an action potential .
Electrical impulses passes along the axon in speed of 2-200miles /hr.
Ion Movement within the Action Potential :
The action potential causes a rush of sodium ions (positive) into the neuron and potassium
ions (minus) out of the neuron, The cell "repolarizes" as the ions become balanced, often
causing a "hyperpolarization ."
Key in a lock:
As a result of the action potential, neurotransmitters are released into the synaptic
junction. Specific neurotransmitters bind with specific receptor sites to allow the passage of
chemicals into the receptor neuron .
31
The action potential causes a release of neurotransmitters which bind to the receptor site
much like a key in a lock. This triggers a post-synaptic potential, which opens the post-
synaptic membrane. Excess neurotransmitters are cleared from the synapse so future
action potentials can occur
Biological basis of behavior:
Reuptake of Neurotransmitter :
The terminal button of the axon reabsorbs (takes
up) the left-over neurotransmitter in the synapse.
This reduces the chance of the post-synaptic cell
from being re-excited by the initial action
potential .
Blocking the Receptor :
Antagonists can block the receptor site, thereby preventing neurotransmitters from binding
with receptor sites. Drugs such as Curare, can cause lethal paralysis by preventing activity in
motor neurons, including those which control the muscles in the lung. You may be more
familiar with Novicaine, a centrally-acting blocker. After being injected with Novicaine at
the dentist's office, you experience a loss of feeling, as Novicaine occupies or blocks sensory
receptors Drugs Acting as Transmitters :
Agonists, can act as neurotransmitters, thereby causing the post-synaptic membrane to
"open" or "fire". A drug such as Mescaline mimics the neurotransmitters Dopamine and
Norepinephrine which are responsible for initiating and maintaing arousal and alertness .
Drugs which Block Reuptake :
Cocaine, commonly known as a stimulant, blocks the reuptake of dopamine, seratonin, and
norepinephrine, which play a role in regulation of mood. Initial use can cause elevated
mood, as excess amounts are released. When the reuptake of these transmitters is blockes,
the excess dopamine continues to excite the receptor. However, over time the body
produces less and less, and the natural stores are depleted, resulting in decreased mood .
Synapse
Synapse Overview/Summary Cells communicate through electrical and chemical
interactions . Electric communication begins with Action Potential Depolarization causes
release of neurotransmitters Chemical interactions are caused by release of
neurotransmitters Neurotransmitters cause a change in the post-synaptic cell The post-
synaptic cell can also be changed through : drugs which act as neurotransmitters (agonists )
increase release of neurotransmitter increase production of neurotransmitter mimic
presence of neurotransmitter act directly on receptor drugs which block receptors
(antagonists ) drugs which cause neurotransmitters to remain (block re-uptake

31
Lec:18
Psychology
Biological basis of behavior (2)
Organization & Structure
The central nervous system has an inherent organization and structure. With an
understanding of cellular activity, we then study this organization .
The Central Nervous System comprises the brain and spinal cord.
The Peripheral Nervous System comprises the nerves external (peripheral) to the spinal
cord .
The Autonomic Nervous System is comprised of the Sympathetic and Parasympathetic
Nervous Systems. These systems are responsible for activating and de-activating internal
states needed at moments of "fight vs. flight ."
Division of the Lobes of the Cerebral Cortex
Frontal Lobes :
o Planning, coordinating, inhibiting actions
o Supervisory control over cortex
o Motor relay station
Temporal Lobes :
o Primary auditory reception and relay (cortical)
o Auditory and musical memory
o Sense of timing
Parietal Lobes :
o Primary somatosensory reception and relay
o Arithmetic & Language Organization (angular gyrus(
o Sense of position & direction
Occipital Lobes :
o Primary (cortical) visual reception and relay
o Visual perception
Sensory and Motor Areas :
o Cortical sensory perception
o Cortical motors control

32
Neuropsychology of Speech :
o Broca's Area (expressive) and Wernike's Area (receptive) are crucial to
communication.
Epilepsy:
Epileptic Seizures result from random electrical activity. This electrical activity spreads from
one brain area to many, creating an overload of synaptic activity .
Split-Brain Procedure:
In order to control the electrical activity caused by epileptic seizures, researchers separated
the hemispheres of the brain. By cutting the corpus collosum, which connects the two
hemispheres,
Explains the procedure and the resulting cognitive changes.
I. Neurons: The Messengers
A. Overview and general structural organization of nervous system
B. Structure of Neuron
o General
o Dendrites
o Cell body
o Axon
o Myelin sheath
o A Nerve or Tract is a group of axons
o Bundled together.
C. Kinds of Neurons:
o Sensory (afferent; inward)
o Motor (efferent; outward)
o Interneurons (between afferent and
o efferent)
o Note: also Glial cells (glia; "housekeeping)"
o but they don't transmit impulses)
D. The Neural Impulse: Transmission within a neuron Polarization and Resting
Potential
.
E. The Synapse: Transmission between neurons
The Synapse
The Pre-synaptic Anatomy and Activities
a. Terminal Button or Synaptic Knob

33
b. Synaptic Vesicles
c. Neurotransmitters
d. Synaptic Cleft or Synaptic Space
The Post-Synaptic Anatomy and Activities
a. Receptor Sites
b. Reuptake
Neurotransmitters
a. Acetylcholine
b. Dopamine,
c. Serotonin ,
d. Norepinephrine,
e. Endorphine
Over 50 different kinds. Fragments of other organic molecules can simulate
neurotransmitters. Some neurotransmitters have multiple functions (excitatory,
inhibitory). Antagonists block or inhibit the normal process. Agonists facilitate it
Acetylcholine (ACh):
Usually excitatory. Attention, arousal , motivation, memory, skeletal muscle
movement. Skeletal muscles and hippocampus. In muscles, botulism toxin prevents
release of Acetylcholine (Ach). Curare and cobra venom block receptor sites. Venom of
black widow spider and certain nerve gases have a destroy Enzyme (AchE) that degrades
Ach, allowing it to flood the synapse and prolong its action, causing convulsions. Possible
link to Alzheimer's via reduced production of Ach in brain cells.
Dopamine:
General Wide range of behavior and emotions.
Excess = schizophrenia; shortage = Parkinson's disease.
Chlorpromazine, a tranquilizer, blocks receptor sites in brain .
Cocaine also inhibits reuptake of dopamine. This was the neurotransmitter focused on in
the book/movie Awakenings, especially its chemical precursor L-Dopa.

34
Serotonin.
Generally inhibitory. Most activities, sleep onset, mood, eating. LSD has similar structure
and activates neurons in the brain that are normally inhibited by that neurotransmitter .
Medications for depression and anxiety such as Prozac, Paxil, Zoloft, and Luvox are all
Selective Serotonin Reuptake Inhibitors (SSRI.)
Norepinephrine (NE).
Generally excitatory. Arousal, wakefulness, learning, memory, mood. Neurons in brain
stem .
Amphetamines, cocaine slow down reuptake and prolong action, lithium speeds up the
reuptake
Gamma-aminobutyric acid (GABA): Inhibitory.
Glutamate. Involved in long term potentiation.
Endorphins: (name composed of endogenous morphine: natural
opiate-like neurotransmitter--or often referred to as
neuromodulator—which is linked to pain control and pleasure
II. Central Nervous System
A. Brain
Hindbrain (central core)
a. medulla - controls breathing, heart rate, and blood pressure.
b. pons -- connects the cerebral cortex at the top of the brain to the cerebellum .
c. cerebellum -- controls certain reflexes, coordinates body movement ,and maintains
equilibrium.
Midbrain (limbic system):
The region between hindbrain and forebrain which is important for hearing and sight and is
one of the primary places in the brain where pain is registered. Hippocampus and
amygdala.

35
Forebrain
a. Thalamus
b. Hypothalamus
c. Cerebrum/Cerebral hemispheres
d. Cerebral Cortex
B. Cortical areas and their functions .
Occipital: visual information
Temporal: auditory information
Parietal: somato-sensory
Frontal: voluntary motor movement
C. Hemispheric specialization
Corpus callosum
Left Hemisphere
Right Hemisphere
Split-brain"" Psychosurgery
D. Reticular formation: wakefulness,
alertness, arousal. Spread across
hindbrain, midbrain, and into forebrain.
E. Limbic system
Memory and emotions
Primary structures:
a. Hippocampus
b. Amygdala
36
Cerebral lateralization
Left hemisphere right hemisphere
Memory for words & numbers Memory for shapes &music
Word recognition
Facial recognition
Positive emotion negative emotion
Response to complex commands Response to simple commands
F. Spinal cord
Structure
Spinal reflexes
G. Tools for studying nervous system
Microelectrode techniques: inside the neuron itself
Macroelectrode techniques: EEG Alpha, Beta, Delta and Theta Waves
Structural imaging (CAT scan) Functional imaging (fMRI
III. Peripheral Nervous System
A. Somatic nervous system
Skeletal (striped) muscles
B. Autonomic nervous system
1.
Smooth muscles.
2.
Sympathetic branch:
a. Prepares for emergency or arousal.
b. Fight or Flight
3. Parasympathetic branch:
a. calms, relaxes body, returns to
normal; involved in digestion and
processes which conserve and protect
bodily functions.
b. controlled in relaxation work, especially bio-feedback
A. Function
1
.
Release hormones from ductless glands into bloodstream
Important: all

37
2
.
Organize nervous system and body tissues
3
.
Activate behavior
B. Thyroid
1
.
Regulates metabolism
2
.
Affects activity level and emotional state.
C. Parathyroids
D. Pineal gland: Day-night activity levels
E. Pancreas
1
.
Insulin/glucagon
2
.
Blood sugar regulation
F. Pituitary
1
.
Posterior
a. Vasopressin
b. Oxytocin
2
.
Anterior: "master gland;"
a. Linked also to nervous system and
i. hormones released by hypothalamus
b. Produces growth hormone
c. Releases ACTH (stress hormone) and
i. can effect the adrenal glands
G. Gonads
1
.
Males: androgens (testosterone )
2
.
Females: estrogens (progesterone)
3
.
Sexual/reproductive function. Studies suggest that they have some other
effects, e.g., effects on aggression and on learning
H. Adrenal Gland
V. Behavior Genetics and Our Human Heritage
A. Genetics
1
.
Basic Facts.
2
.
Chromosomes and Genes
a. Genes
38
b. Chromosomes
c. DNA
d. Dominant and recessive genes
e. Sex-linked genes (M > F)
(
1
)
color blindness
(
2
)
hemophilia
f. Blueprints or recipes?
B. Genetics and Behavior
1
.
Animal Behavior Genetics:
a. Heritability of behavioral traits
b. Selective brding: Thompson
2
. Human Behavior Genetics:
a. Human Genome Project: Map all 23
i. sets of human chromosomes.
b. Family Studies
c. Twin studies: identical vs fraternal.
i. Schizophrenia: Identical twins 50%;
ii. fraternal 15%
d. Adoption studies
C. Evolution:
1
.
Natural selection: How evolution occurs
and which traits survive.
3.
Can restate Darwin using gene theory.
D. Evolutionary Psychology
1
.
Environmental influences on gene action
2
.
Evolution with its natural selection, predisposes humans in certain ways, thus is
the direct cause of certain behavioral traits, e.g., aggressiveness and sexuality in men,
submission and nurturance in women.
E. Social Implications
F. Environment-Genetic Interaction :
1
.
Genes predispose to environmental influence, environment supplies
influence to actually produce behavioral effect
2
.
Examples : Diabetes <=> overweight Schizophrenia <=> stress
39
Lec:19
Psychology
Sleep and dream
Theories of Sleep:
Repair/Restoration:
o Sleep allows for recuperation from physical, emotional, and intellectual fatigue
Evolutionary/Circadian
o Sleep is part of a circadian cycle
o Sleep evolved to conserve energy and protect from predators
Myths of Sleep:
Everyone needs 8 hrs of sleep per night to maintain health
Learning of complicated subjects can be done during sleep
Some people never dream
Dreams last only a few seconds
Genital arousal during sleep reflects dream content
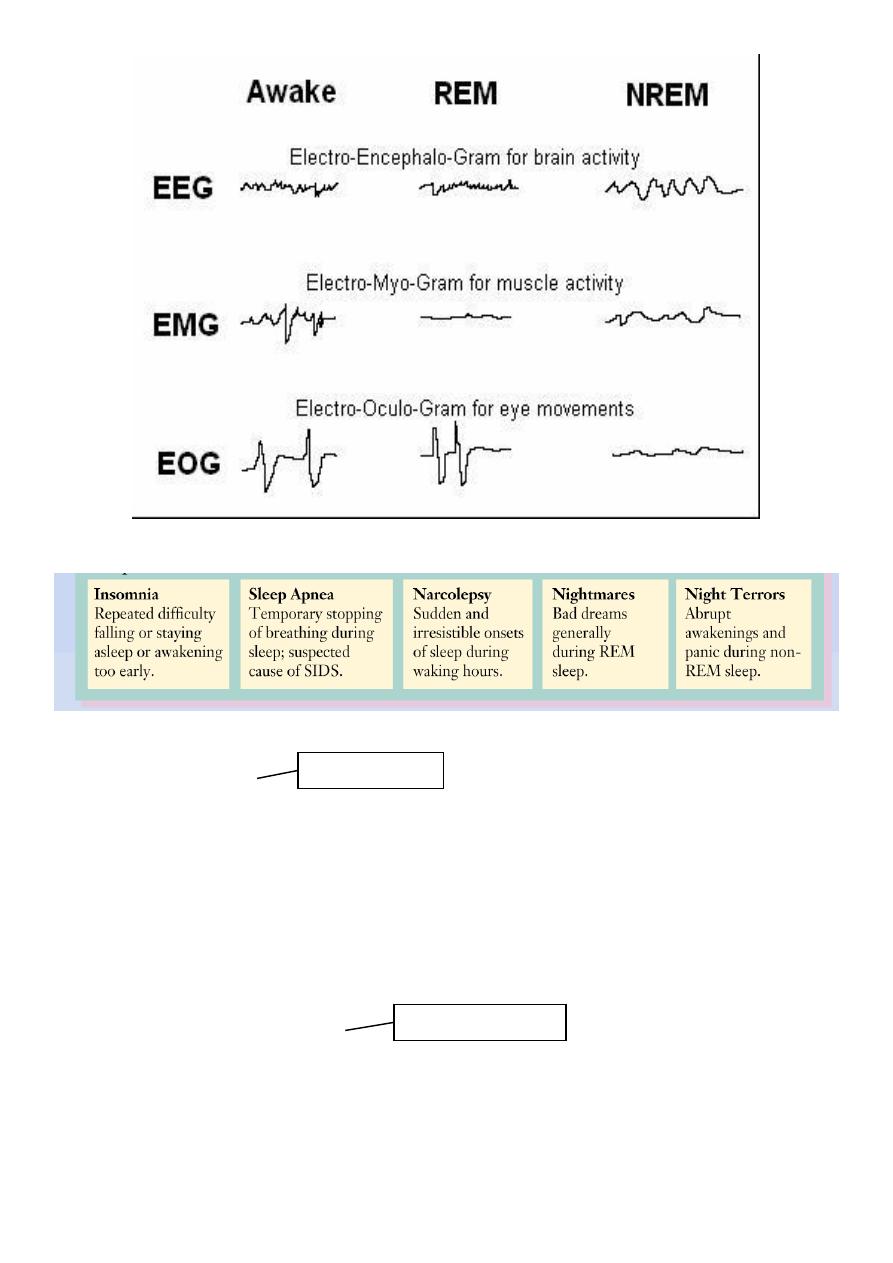
STAGES OF SLEEP:
Sleep stages:
non-rapid eye movement (NREM or non-REM)sleep
rapid eye movement (REM)sleep
Important: all
Important: all
Important: all
41
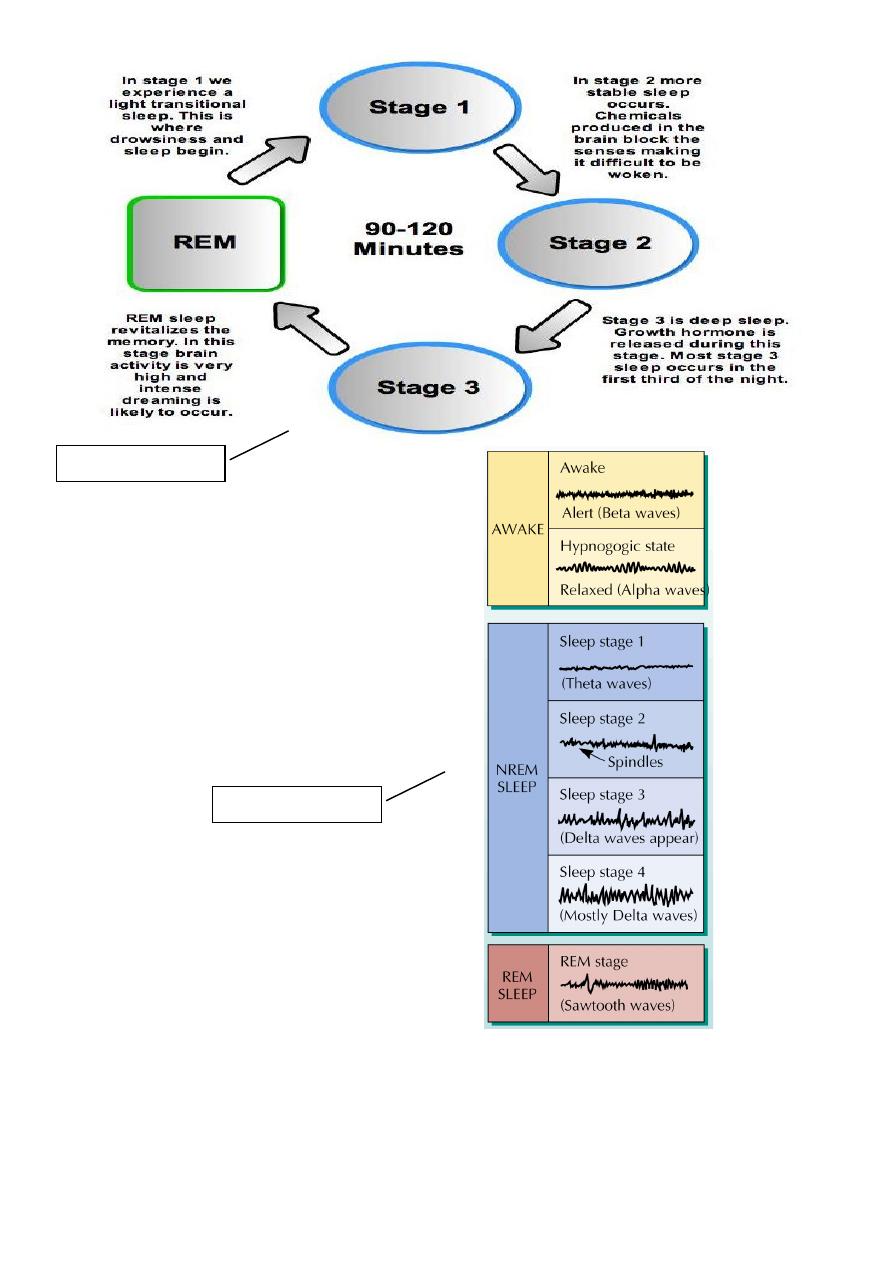
EEG Changes during Sleep:
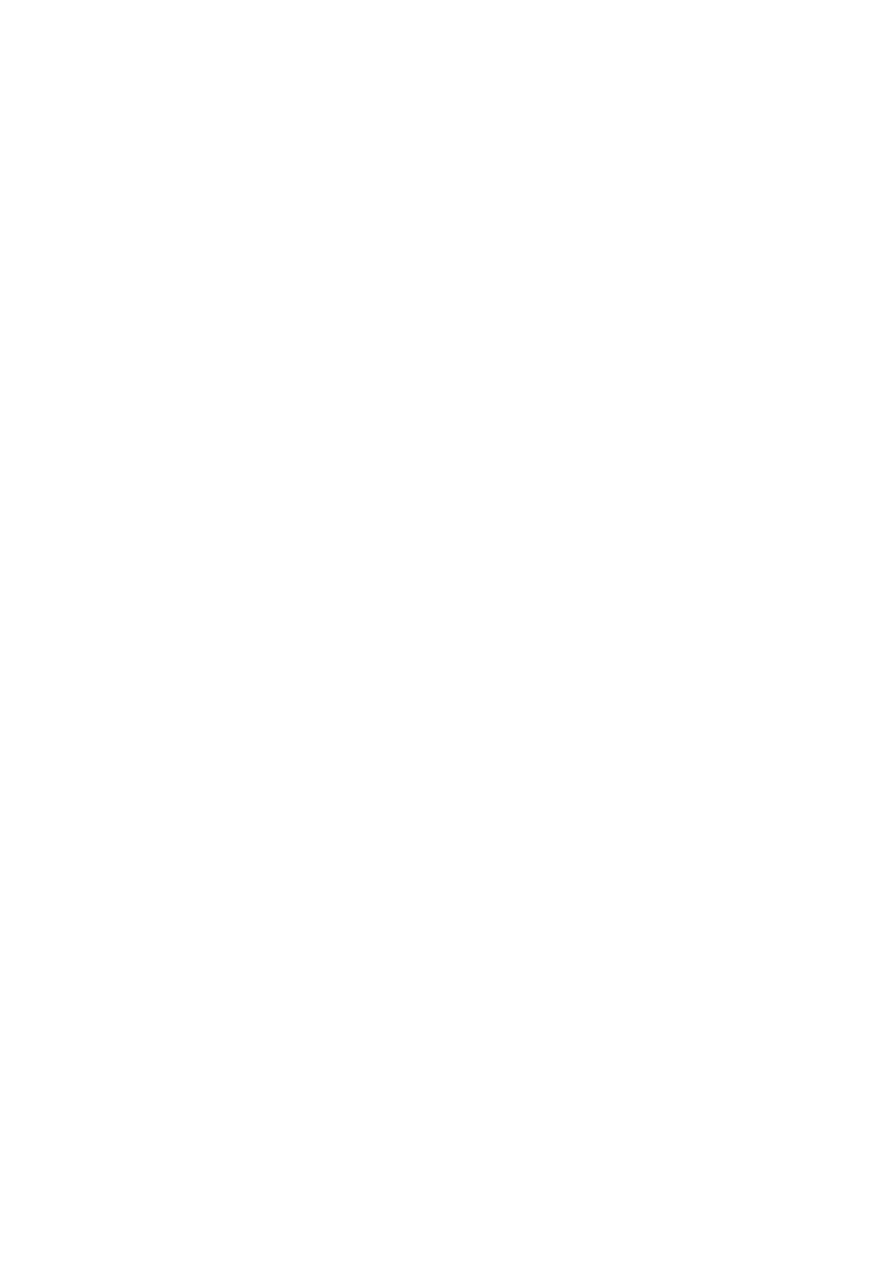
Sleep:
Sleep proceeds in cycles of REM and NREM, the order normally being N1 → N2 → N3 → N2
→ REM. There is a greater amount of deep sleep (stage N3) earlier in the sleep cycle, while
the proportion of REM sleep increases later in the sleep cycle and just before natural
awakening.
Important: MCQ
Important: MCQ
41
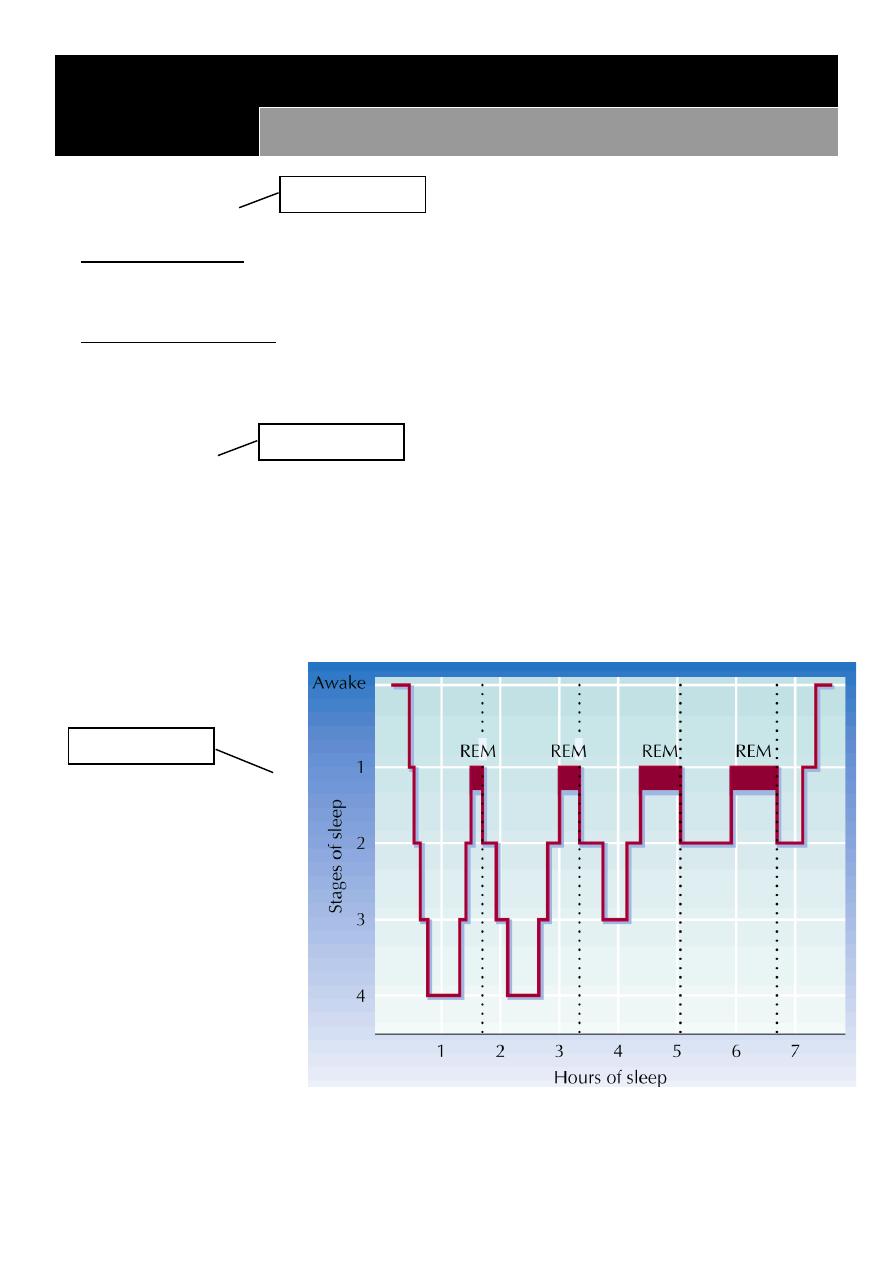
(NREM or non-REM) sleep:
o Stage N1 refers to the transition of the brain from alpha waves having a frequency of 8–
(common in the awake state) to theta waves having a frequency of 4–7 Hz. This
stage is sometimes referred to as somnolence or drowsy sleep. Sudden twitches and
hypnic jerks, also known as positive myoclonus, may be associated with the onset of
sleep during N1. During N1, the subject loses some muscle tone and most conscious
awareness of the external environment.
o Stage N2 is characterized by sleep spindles ranging from 11 to 16 Hz (most commonly
12–14 Hz) and K-complexes. During this stage, muscular activity as measured by EMG
decreases, and conscious awareness of the external environment disappears. This stage
occupies 45–55% of total sleep in adults.
o Stage N3 (deep or slow-wave sleep) is characterized by the presence of a minimum of
20% delta waves ranging from 0.5–2 Hz. This is the stage in which parasomnias such as
night terrors, nocturnal enuresis, sleepwalking, and somniloquy occur.
o Many illustrations and descriptions still show a stage N3 with 20–50% delta waves and a
stage N4 with greater than 50% delta waves; these have been combined as stage N3.
(REM) sleep:
o The criteria for REM sleep include rapid eye movements as well as a rapid low-voltage
EEG. Most memorable dreaming occurs in this stage. At least in mammals, a descending
muscular atonia is seen. Such paralysis may be necessary to protect organisms from self-
damage through physically acting out scenes from the often-vivid dreams that occur
during this stage. It start 90 min after sleep also called paradoxical sleep
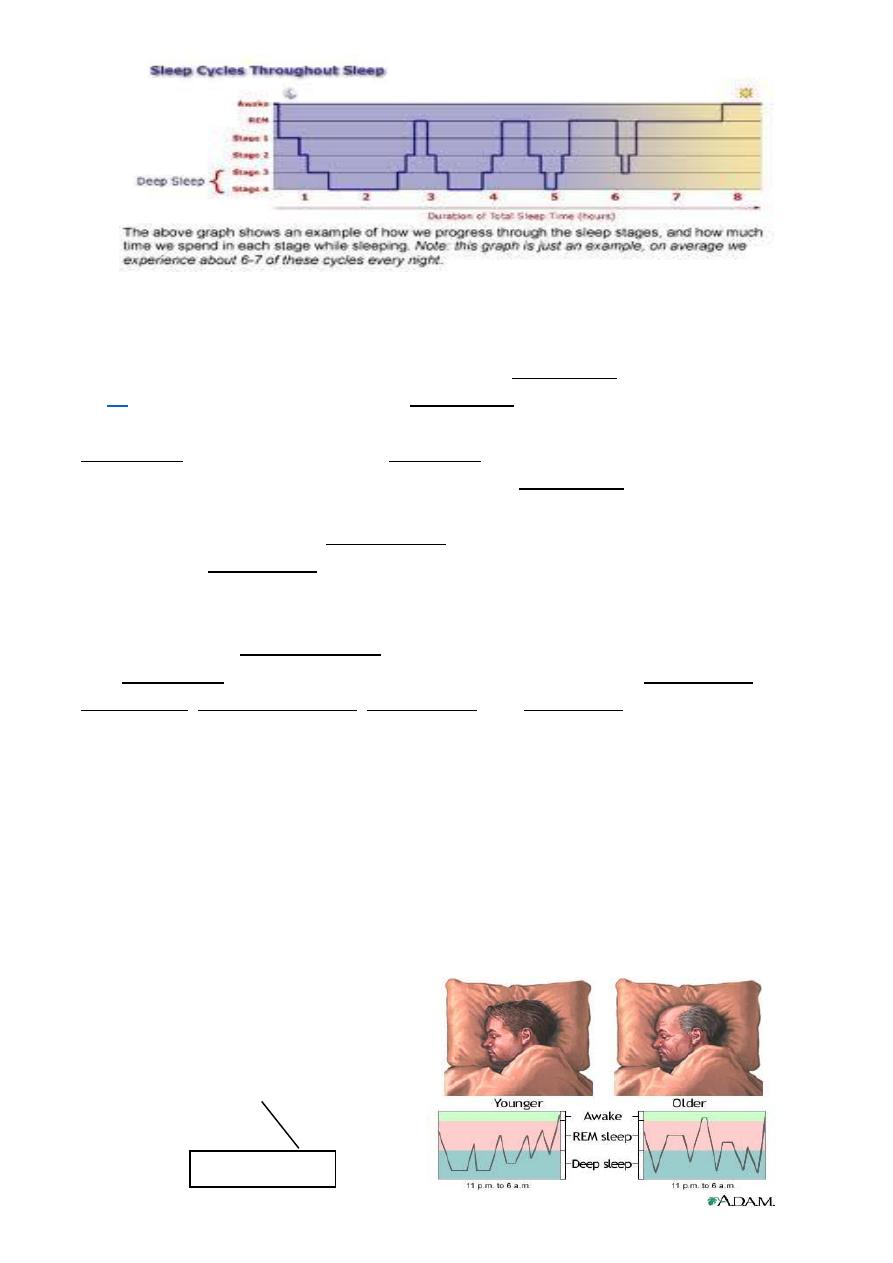
(REM) sleep:
o Infant spend half their sleep in rem
o 20-25% by age of five
o 18% in adult
o Elderly 3-4%
Important: all
42
Sleep Disorders:
Functions of Sleep:
REM Sleep:
o Consolidation of new memories
o Role in learning
o Absent in lower mammals
Non-REM sleep
o People deprived of all sleep show greater time spent in non-REM sleep the next
night
Effects of Sleep Deprivation:
Reduced immunity
Mood alteration
Reduced concentration and motivation
Increased irritability
Lapses in attention
Important: all
Important: assay

43
Reduced motor skills
Sleep regulation:
Most researchers think that sleep is regulated by small numbers of interconnecting
systems or center that locate chiefly in the brain stem and that mutually activate and
inhibit one another
Many studies support the role of serotonin in sleep regulation, lack of serotonin found
to reduce sleep for considerable time
also Adenosine which is created over the course of the day, high levels of adenosine
lead to sleepiness
Function of sleep:
Restoration of homeostatic function
Appear to be crucial for normal thermal regulation and energy conservation
Rem stage may associated with satisfying metabolic needs
Sleep deprivation & sleep debt:
Prolong period of sleep deprivation lead to ego disorganization
Rem deprivation lead to irritability and lethargy
Sleep debt is the effect of not getting enough rest and sleep; a large debt causes
mental, emotional and physical fatigue.
Sleep debt results in diminished abilities to perform high-level cognitive functions.
Sleep requirement:
Some persons normally sleep fewer than 6 hours to function adequately called short
sleeper
Those who sleep more than9 hours each night called long sleeper
Long sleeper have more rem sleep
Sleep need increased with physical work, exercise, illness, pregnancy, general mental
stress and increased mental activity
44
Dreams
Dreams:
State of consciousness in which remembered image and fantasies which are
temporarily confused with external reality
Dreaming is the perceived experience of sensory images and sounds during sleep, in a
sequence which the dreamer usually perceives more as an apparent participant than as
an observer
Theories of Dreaming:
Psychoanalytic: Dreams represent disguised symbols of repressed desires and
anxieties
Biological: Dreams represent random activation of brain cells during sleep
Cognitive: Dreams help to sift and sort the events of the day
Freud’s theory: His psycholytic theory states that dreams are unconscious wish
fulfillment of need unmet during waking states. He believe that dreams often involve
combination of early childhood experience and daily residue
Cognitive theory: proposes that dreaming can best be understood by relying on the
same cognitive concept that are used in studying the waking mind, it mean that dreams
involve in processing information, memorization and possibly problem solving.
Activation-synthesis theory : this theory state that dreams are powered by
spontaneous firing of neurons, dreams reflect the brains effort to make sense out or
find meaning in the neuronal activity take place during sleep
Dreaming:
Do you know when you are dreaming?
Yes some times during occasional awaking
Can people control the content of their dreams?
Yes by pre dream suggestion post hypnotic suggestion
Do males and females dream about different things?
Males dreams have more content about males , aggression , gross anatomy , sexuality
and dreamer involve success
Females dreams are more likely to be about females, friends and victimization
Why can't we remember all of our dreams?
We can't because dreaming occur at such a low level of consciousness , we remember
it best we awake while dreaming or just after
Important: First 3 points only