1
L3
Peptic Ulcers
The histologic appearance varies with the activity, chronicity, and degree of healing. In a
chronic, open ulcer, four zones can be distinguished :
(1) the base and margins have a thin layer of necrotic fibrinoid debris underlain by
(2) a zone of active nonspecific inflammatory infiltration with neutrophils predominating,
underlain by
(3) granulation tissue, deep to which is
(4) fibrous, collagenous scar that fans out widely from the margins of the ulcer.
Vessels trapped within the scarred area are characteristically thickened and occasionally
thrombosed, but in some instances they are widely patent. With healing, the crater fills with
granulation tissue, followed by re-epithelialization from the margins and more or less
restoration of the normal architecture (hence the prolonged healing times). Extensive fibrous
scarring remains
Gastric tumors
Tumors arising from the mucosa predominate over mesenchymal tumors. Mucosal tumors
are classified into polyps and carcinoma.
Gastric Polyps
The term polyp is applied to any nodule or mass that projects above the level of the
surrounding mucosa. Occasionally, a lipoma or leiomyoma arising in the wall of the stomach
may protrude from under the mucosa to produce an apparent polypoid lesion.
Pathology of Gastrointestinal Tract
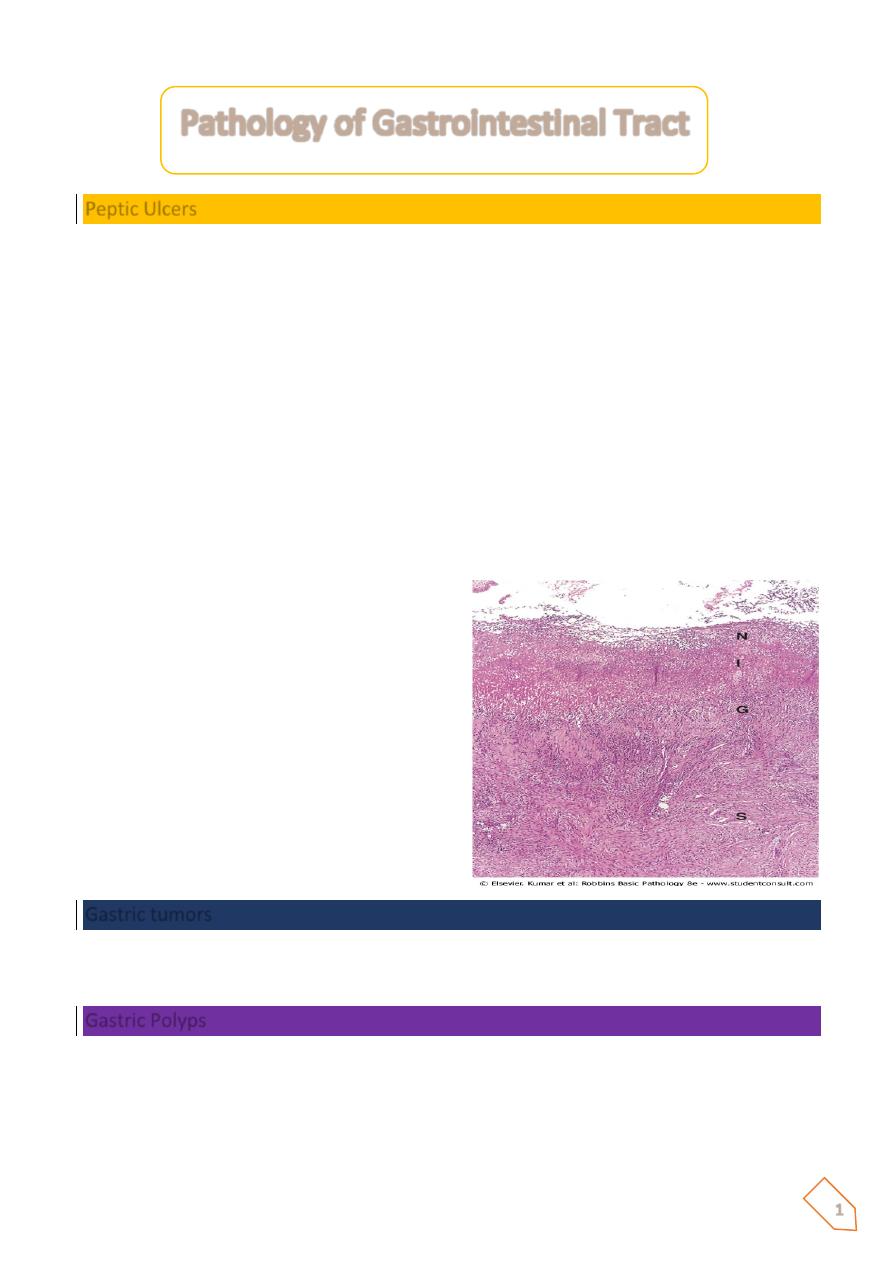
Medium-power detail of the base of a
nonperforated peptic ulcer, demonstrating
the layers of necrosis (N), inflammation (I),
granulation tissue (G), and scar (S) moving
from the luminal surface at the top to the
muscle wall at the bottom.

2
However, the use of the term polyp in the gastrointestinal tract is generally restricted to mass
lesions arising in the mucosa. Gastric polyps are uncommon and are found in about 0.4% of
adult autopsies, as compared with colonic polyps, which are seen in 25% to 50% of older
persons.
In the stomach, these lesions are most frequently
1. hyperplastic polyps (80% to 85%),
2. fundic gland polyps (∼10%), and
3. adenomatous polyps (∼5%).
All three types arise in the setting of chronic gastritis and so are seen in the same patient
populations, there is a definite risk of an adenomatous polyp harboring adenocarcinoma,
which increases with polyp size. Because the different types of gastric polyps cannot be
reliably distinguished by endoscopy, histologic examination is mandatory.
Gastric Carcinoma
Among the malignant tumors that occur in the stomach, carcinoma is the most important and
the most common (90% to 95%). Next in order of frequency are lymphomas (4%), carcinoids
(3%), and stromal tumors (2%).
Gastric cancers show two morphologic types, called intestinal and diffuse.
ⱴ The
intestinal type
is thought to arise from gastric mucous cells that have undergone
intestinal metaplasia in the setting of chronic gastritis. This pattern of cancer tends to
be better differentiated and is the more common type in high-risk populations.
ⱴ
The diffuse variant
is thought to arise de novo from native gastric mucous cells, is not
associated with chronic gastritis, and tends to be poorly differentiated.
Whereas the intestinal-type carcinoma occurs primarily after age 50 years with a 2 : 1 male
predominance,
The diffuse carcinoma occurs at an earlier age with female predominance.
The intestinal and diffuse forms of gastric carcinomas can be considered as distinct entities,
although their clinical outcome is similar.
Morphology
The location of gastric carcinomas within the stomach is as follows:
Pylorus and antrum, 50% to 60%; cardia, 25%; and the remainder in the body and fundus.
The lesser curvature is involved in about 40% and the greater curvature in 12%.
Thus, a favored location is the lesser curvature of the antropyloric region. However, less
frequent, an ulcerative lesion on the greater curvature is more likely to be malignant than
benign.
3
Gastric carcinoma is classified on the basis of depth of invasion, macroscopic growth pattern,
and histologic subtype.
The morphologic feature having the greatest impact on clinical outcome is the
depth of
invasion.
Early gastric carcinoma is defined as a lesion confined to the mucosa and submucosa,
regardless of the presence or absence of perigastric lymph node metastases.
Advanced gastric carcinoma is a neoplasm that has extended below the submucosa into the
muscular wall and has perhaps spread more widely.
The four macroscopic growth patterns of gastric carcinoma,(
Bormann classification
) which
may be evident at both the early and advanced stages, are
1.
Exophytic,
with protrusion of a tumor mass into the lumen;
2.
Flat or depressed
, in which there is no obvious tumor mass within the mucosa; and
3.
Excavated
, whereby a shallow or deeply erosive crater is present in the wall of the
stomach.
Exophytic tumors may contain portions of an adenoma.
Flat or depressed malignancy presents only as regional effacement of the normal surface
mucosal pattern. Excavated cancers may mimic, in size and appearance, chronic peptic ulcers,
although more advanced cases show heaped-up margins .Uncommonly, a broad region of the
gastric wall, or the entire stomach, is extensively infiltrated by malignancy.
The rigid and thickened stomach is termed a leather bottle stomach, or 4
- linitis plastica
;
metastatic carcinoma from the breast and lung may generate a similar picture
Histologic appearances of gastric cancer (lauren histological classification)
Are best classified into the intestinal type and diffuse type.
The
intestinal variant
is composed of malignant cells forming neoplastic intestinal glands
resembling those of colonic adenocarcinoma.
The
diffuse variant
is composed of gastric-type mucous cells that generally do not form glands
but rather permeate the mucosa and wall as scattered individual "
signet-ring" cells
or small
clusters in an "infiltrative" growth pattern.
Whatever the histologic variant, all gastric carcinomas eventually penetrate the wall to
involve the serosa, spread to regional and more distant lymph nodes, and metastasize widely.
For obscure reasons, the earliest lymph node metastasis may sometimes involve a
supraclavicular lymph node (
Virchow node
).
Another somewhat unusual mode of intraperitoneal spread in females is to both the ovaries,
giving rise to the so-called
Krukenberg tumor.
4
Pathogenesis
Environmental Factors
• Cigarette smoking
• Low socioeconomic status
Nitrites derived from nitrates (water, preserved food)
Smoked and salted foods, pickled vegetables, chili peppers
Lack of fresh fruit and vegetables diet
Present in most cases of intestinal-type carcinoma
• Infection by H. pylori
Host Factors
• Barrett esophagus
• Gastric adenomas
• Favors reflux of bilious, alkaline intestinal fluid
• Partial gastrectomy
• Intestinal metaplasia is a precursor lesion
• Hypochlorhydria: favors colonization with H. pylori
• Chronic gastritis
Genetic Factors
Familial gastric carcinoma syndrome (E-cadherin mutation)
Hereditary nonpolyposis colon cancer syndrome
Family history of gastric cancer
Slightly increased risk with blood group A
5
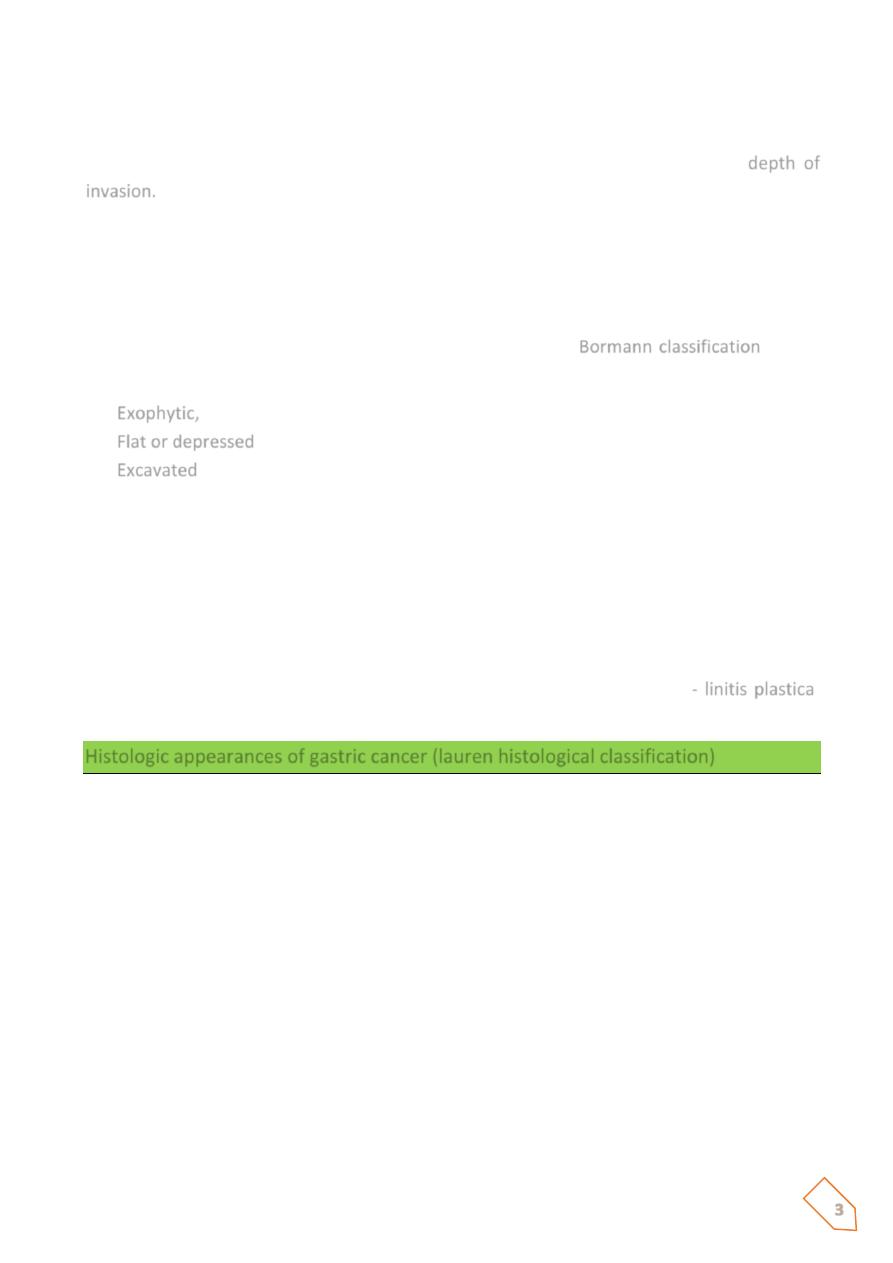
Gastric carcinoma.
Gross photograph showing an
illdefined, excavated central ulcer
surrounded by irregular, heaped-up
borders
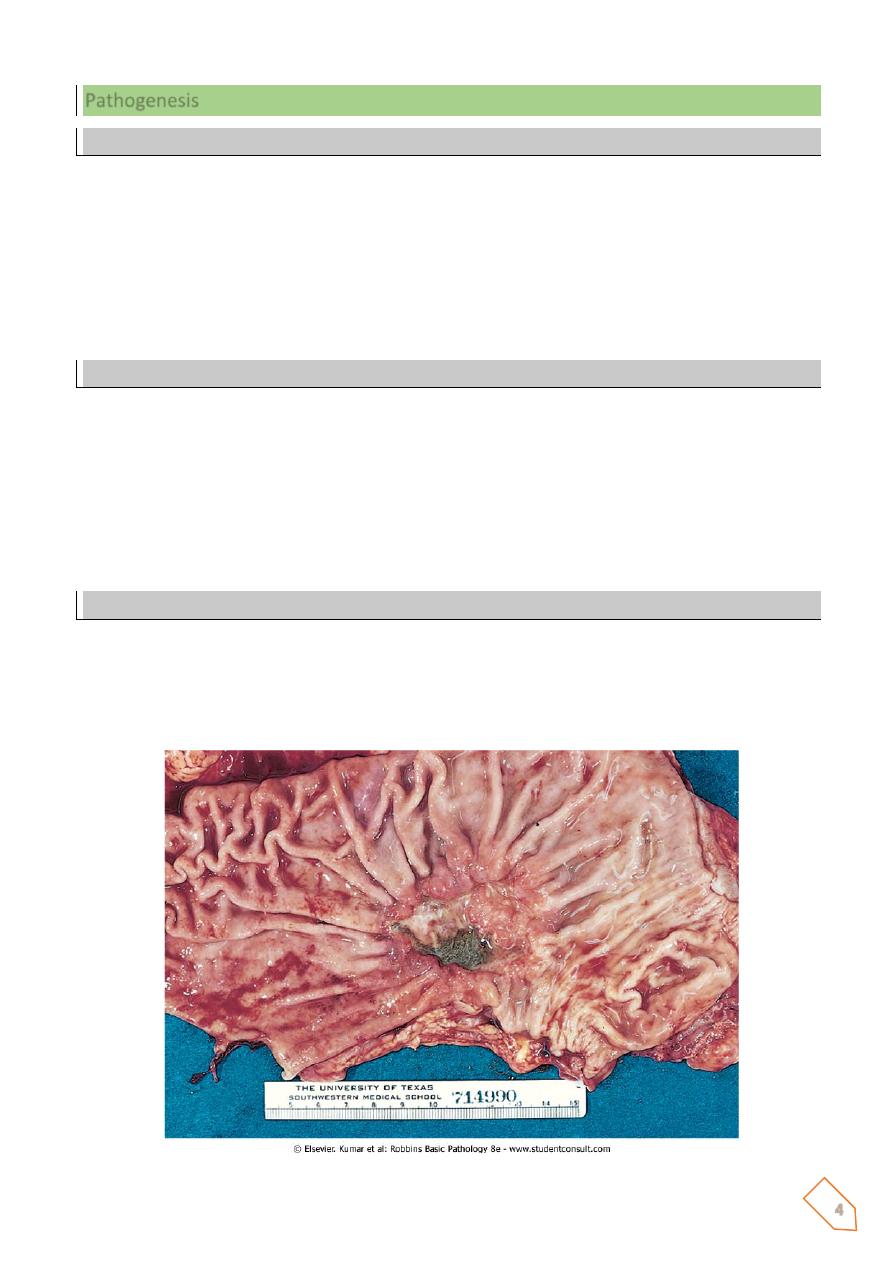
Here is a much larger 3 x 4 cm
gastric ulcer that led to the
resection of the stomach shown
here. This ulcer is much
deeper with more irregular margins
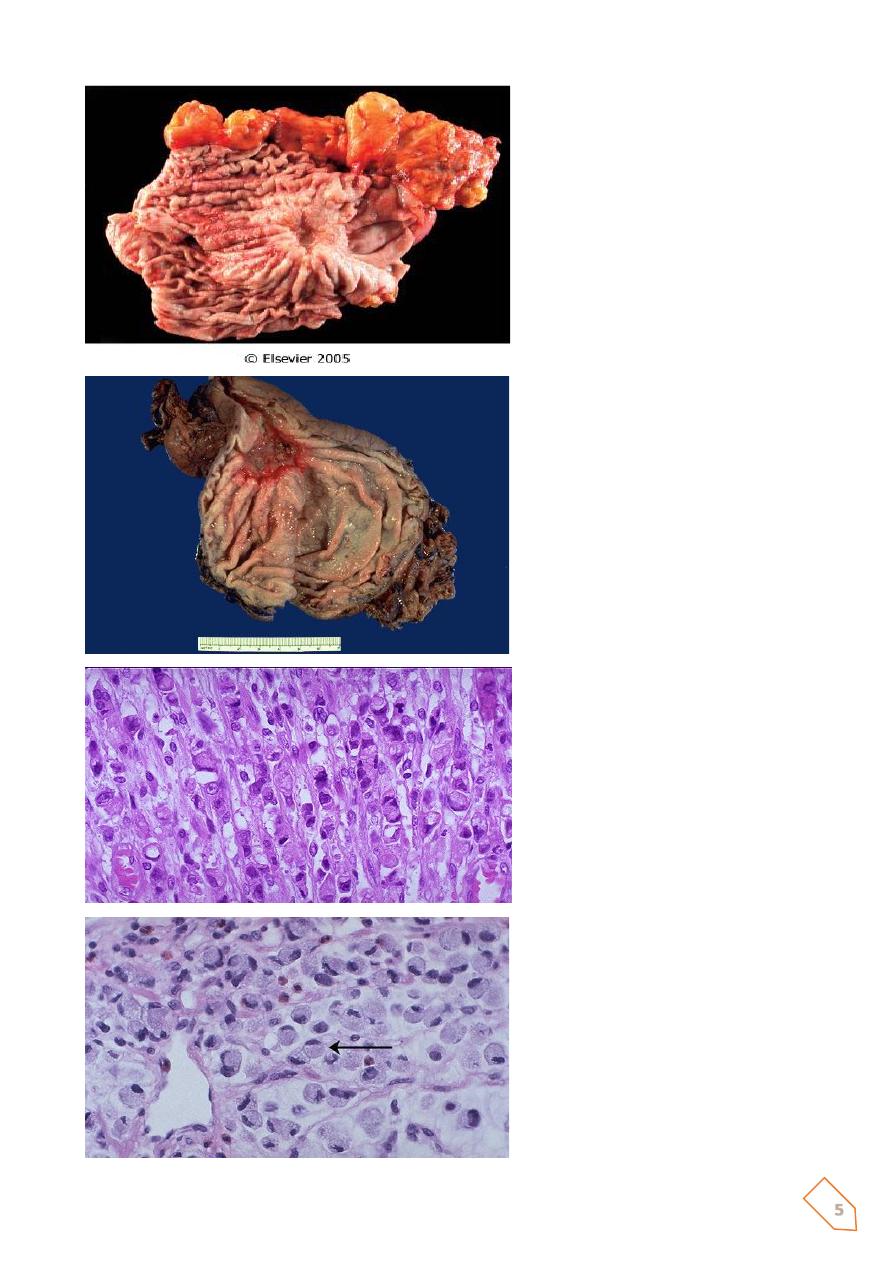
At high power, this gastric
adenocarcinoma is so poorly
differentiated that glands are not
visible. Instead, rows of
infiltrating neoplastic cells with
marked pleomorphism are seen.
Many of the neoplastic cells have
clear vacuoles of mucin.
This is a signet ring cell pattern of
adenocarcinoma in which
the cells are filled with mucin
vacuoles that push the nucleus to
one side, as shown at the arrow.
6
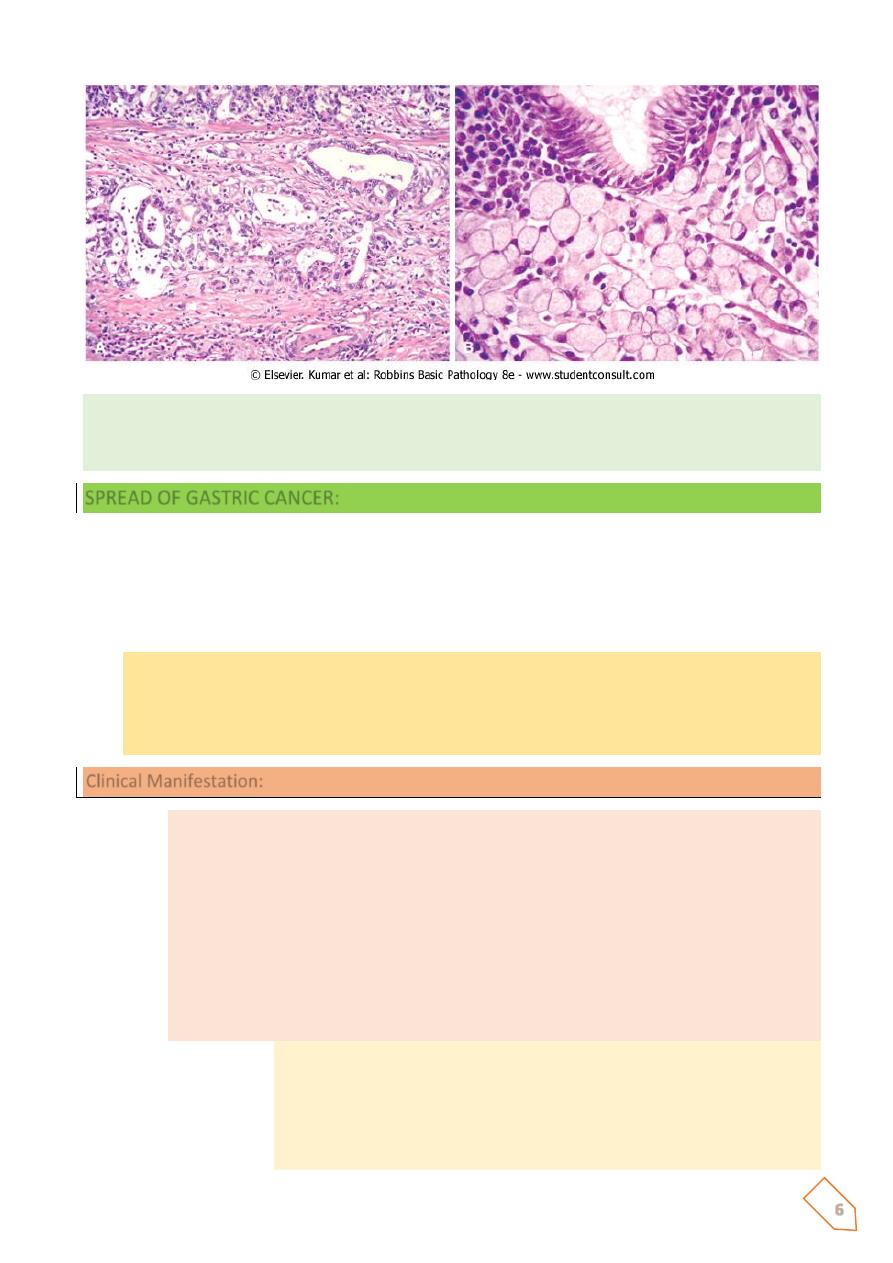
Gastric cancer. A, H&E stain demonstrating intestinal type of gastric carcinoma with gland
formation by malignant cells that are invading the muscular wall of the stomach. B, Diffuse
type of gastric carcinoma with signet-ring tumor cells.
SPREAD OF GASTRIC CANCER:
The diffuse type spreads rapidly through the submucosal and serosal lymphatic and
penetrates the gastric wall at early stage, the intestinal variety remains localized for a while
and has less tendency to disseminate.
The spread by:
1. Direct (loco regional)
2. Lymphatic
3. Blood (Haematogenous)
4. Transcoelomic
Clinical Manifestation:
1. Weight loss due to anorexia and early satiety is the most common symptoms
2. Abdominal pain (not severe) common
3. Nausea / vomiting
4. Chronic occult blood loss is common; GIT bleeding (5%)
5. Dysphagia (cardia involvement)
6. Paraneoplastic syndromes ( Trousseau’s syndrome – thrombophlebitis;
acanthosis nigricans – hyperpigmentation of axilla and groin; peripheral
neuropathy)
7. Signs of distant metastasis:
a. Hepatomegally / ascites
b. Krukenbergs tumor
c. Blummers shelf (drop metastasis)
d. Virchow’s node
e. Sister Joseph node (pathognomonic of advances dse)
7
Screening of Gastric Cancer
Patients at risk for gastric CA should undergo yearly endoscopy and biopsy:
a. Familial adenomatous polyposis
b. Hereditary nonpolyposis colorectal cancer
c. Gastric adenomas
d. Menetrier’s disease
e. Intestinal metaplasia or dysplasia
f. Remote gastrectomy or gastrojejunostomy
SUMMARY
Gastric Tumors More than 90% of gastric tumors are carcinomas; lymphomas, carcinoids and
stromal tumors are relatively infrequent.The two main types of gastric adenocarcinomas are
the intestinal and diffuse types; macroscopic patterns of both types may be exophytic, flat or
depressed, or excavating.Intestinal type of adenocarcinoma is associated with chronic
gastritis caused by H. pylori infection, with gastric atrophy and intestinal metaplasia;
composed of malignant cells forming intestinal glands.Diffuse type of adenocarcinoma is not
associated with H. pylori infection; composed of gastric type of mucous cells (signet ring cells)
that permeate the mucosa without forming glands.
Mubark A. Wilkins