1
Fifth stage
Gynecology
Lec-8
د. احمد جاسم
6/4/2016
Metastatic Tumors of Ovary
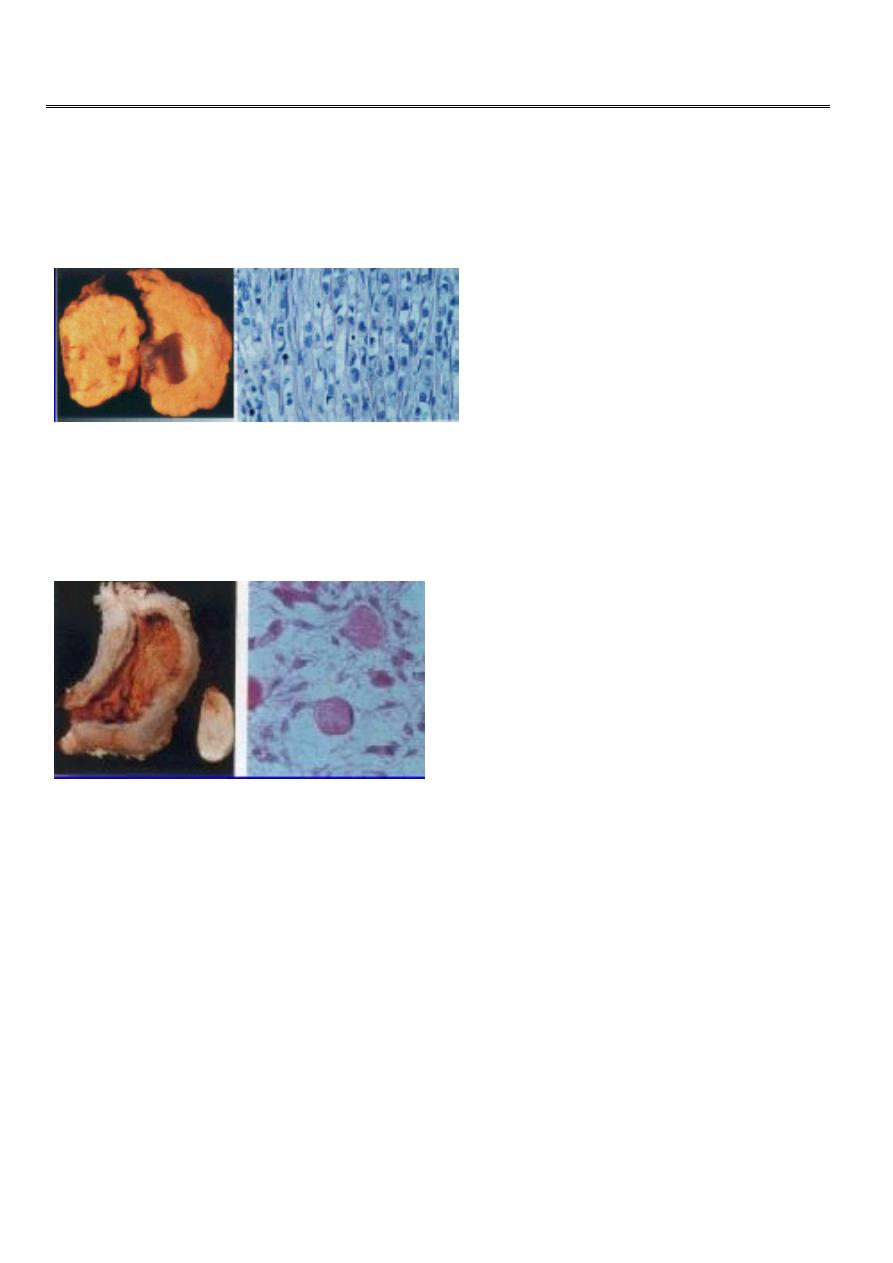
METASTATIC TUMOR FROM BREAST CANCER
both ovaries replaced by pale, rather nodular tumor, with breast cancer cells arranged in
long lines perpendicular to the surface of the ovarian cortex
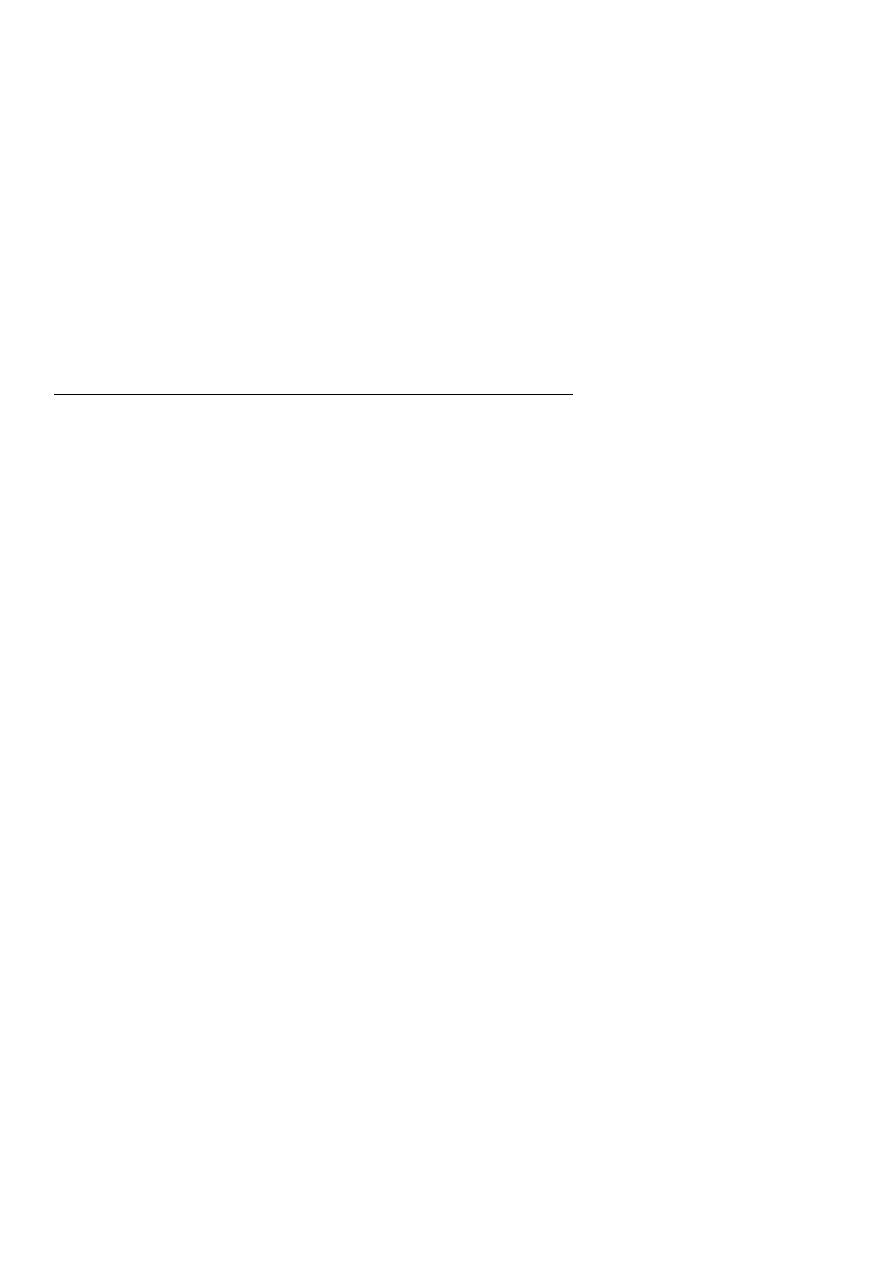
METASTATIC TUMOR FROM GASTRIC CANCER (Krukenberg )
gastric carcinoma of the fundus, with secondary ovarian tumor (Mucus-secreting signet-ring
cells)
Neoplastic Ovarian Tumours
• Surface epithelial – 65-70%
• Germ cell tumors – 15-20%
• stromal – 10-15%
• Metastatic tumors – 5%
Epidemiology
• 15,900 deaths annually

2
• 4th common cause of cancer mortality
• Most (70%) diagnosed at advanced stage where cure is uncommon.
• 23,000 cases annually
• Ranks 3r
d
among gynecologic cancers
• Ranks 5
th
among women cancers.
Risk Factors
• Personal H :
• Any age ( common >40ys) .
• Nulliparous.
• Late age 1
st
preg
• History of breast or colon cancer.
• Gonadal Dysgenesis
• Talcum powder
– Increased risk in women who use talc powder on genital area
• M.H:
– Early menarche.
– Late menopause
– prolonged use of fertility drugs without achieving pregnancy
– Hormone replacement therapy > 10 years
– Uninterrupted ovulation.
• F.H
– Mother, sister or daughter with ovarian cancer.
Protective factors
Multiparity: First pregnancy before age 30
Oral contraceptives.
Hysterectomy
Lactation
Bilateral oopherectomy

3
complications of benign ov Tumours
• torsion
• hemorrhage
• rupture
• infection
• incarceration
• malignant change
• complications during pregnancy
Diagnostic tools
• History
• Exam (including rectal)
• Investigations:-
– TVS –masses and mass characteristics
– Tumor markers – CA-125, LPA (plasma
lysophosphatidic acid)
– CT – assess spread to LN, pelvic and abdominal structures
– MRI – best for distinguishing malignant from
benign tumors
Clinical picture of benign ov tumors
• Symptoms:
– functioning tumors
– nonfunctioning tumors
• swelling
• pressure symptoms
• pain
• menstrual disturbances
• ovarian cachexia
4
• Signs
– small ov tumors
– large ov tumors
• DD:
– from other pelvic swellings
– from other abdominal swellings
Clinical picture cancer ovary
Benign ovarian Tumours + The following suggest malignancy
age:mostly postmenopausal
pain: chronic and persistent
rapid course
bilaterality
Solidity ( variegated consistency )
fixity
metastases :nodules in DP, lymph nodes
ascitis
edema LL
cachexia
Staging:
Vertical incision.
Aspirate, or saline washing.
Careful assessment., Liver, rt hemidaphragm, All other organs as omentum,
intestine,….
Para aortic LN sampling.
Proper staging, for prognosis, selection of adjuvant therapy…..
Ovarian Cancer Staging
• Stage 1
– 1A: One ovary
– 1B: Both ovaries
– 1C: with malignant ascites, rupture surface tumor

5
• Stage 2
– 2A: Reproductive organs
– 2B: Other pelvic organs
– 2C: with malignant ascites or washings
• Stage 3
– 3A: microscopic upper abdominal disease
– 3B: upper abdominal metastasis less than 2 centimeters
– 3C: upper abdominal metastasis greater than 2 centimeters
• Stage 4 is disease outside the peritoneal cavity
– Liver parenchymal metastasis.
– Pleural effusion
– Supraclavicular nodes
Treatment
• Depends on
– Staging
– Tumor type
– Age
– Desire for future fertility
• Include surgery, chemotherapy and/or radiation therapy
• Surgery for ov. cancer
• Complete surgery:TAH/BSO +omentectomy+lymphadenectomy
– other cases of stage Ia
• Conservative surgery: unilateral adnexectomy indicated:
– stage Ia: intact capsule, negative peritoneal washing, free omentum,
– well differentiated T,
– young patient with low parity
– Stage Ib,c
6
Surgery for ov. Cancer cont…
• Cytoreductive surgery: for all other stages
– optimum cytoreduction leaving no macroscopic lesion or one less than 1.5 cm.
– consist of TAH/BSO +omentectomy+lymphadenectomy+may be bowel resection &
anastmosis.
– Second look surgery after chemotherapy
Surgical treatment
• Primary debulking and cytoreduction; may include:
– Bilateral salpingo-oopherectomy
– Hysterectomy
– Lymphadenectomy (Para-aortic, inguinal)
– Omentectomy
– “brushing” of diaphragm
– Examination of liver
Chemotherapy & radiotherapy for ov cancer
• Chemotherapy:
– adjuvant to surgery to improve prognosis in early stages
– induce remission in advanced cases
– agents: alkylating agents,platinum: single drug and multible drug regimens
• Radiotherapy:
– has less place in modern practice, replaced by chemotherapy
– was given for cases with small residual lesions (< 2 cm)
– forms are:
• radioactive isotope: intraperitoneal
32
P ,
• external-beam radiotherapy
Chemotherapy and Radiation
• Usually 6 cycles of chemotherapy
• Cisplatin (or Carboplatin) plus Paclitaxel most commonly used combination therapy
• XRT