1
L5
Small and Large Intestines
COLONIC DIVERTICULOSIS
A diverticulum is a blind pouch leading off the alimentary tract, lined by mucosa, that
communicates with the lumen of the gut.
Congenital diverticula have all three layers of the
bowel wall (mucosa, submucosa, and most notably the muscularis propria) and are distinctly
uncommon. The prototype is Meckel diverticulum,
Virtually all other diverticula are acquired and either lack or have an attenuated muscularis
propria.
Acquired diverticula may occur anywhere in the alimentary tract, but by far the most
common location is the colon, giving rise to diverticular disease of the colon, also called
diverticulosis.
It is attributed to the consumption of a refined, low-fiber diet, resulting in reduced stool bulk
with increased difficulty in passage of intestinal contents. Exaggerated spastic contractions of
the colon isolate segments of the colon in which the intraluminal pressure becomes markedly
elevated, with consequent herniation of the bowel wall through the anatomic points of
weakness.
TUMORS OF THE SMALL AND LARGE INTESTINES
ⱴ Epithelial tumors of the intestines are a major cause of morbidity and mortality
worldwide. The colon, including rectum, is host to more primary neoplasms than any
organ in the body.
ⱴ Colorectal cancer ranks second to bronchogenic carcinoma among the cancer killers.
Adenocarcinoma constitute the vast majority of colorectal cancers and represent 70%
of all malignancies arising in the GIT.
Pathology of Gastrointestinal Tract
MORPHOLOGY Most colonic
diverticula are small flasklike
or spherical outpouchings,
usually 0.5 to 1 cm in
diameter
2
ⱴ
Curiously, the small intestine is an uncommon for benign or malignant tumors despite
its great length, Whereas the small bowel represents 75% of the length of the
alimentary tract, its tumors account for only 3% to 6% of gastrointestinal tumors, with
a slight preponderance of benign tumors. The classification of intestinal tumors is the
same for the small and large intestine
.
Terminology
A polyp is a tumorous mass that protrudes into the lumen of the gut; traction on the mass
may create a stalked, or pedunculated, polyp. Alternatively, the polyp may be sessile, without
a definable stalk. Polyps may be formed as the result of abnormal mucosal maturation,
inflammation, or architecture.
These polyps are non-neoplastic and do not have malignant potential; an example is the
hyperplastic polyp. Those polyps that arise as the result of epithelial proliferation and
dysplasia are termed adenomatous polyps or adenomas. They are true neoplastic lesions
(“new growth”) and are precursors of carcinoma.
Non-neoplastic Polyps
Hyperplastic polyps
, which are small (less than 5 mm in diameter), nipple-like, hemispherical,
smooth protrusions of the mucosa. They may occur singly but are more often multiple.
Although they may be anywhere in the colon, well over half are found in the rectosigmoid
region.
Histologically
, they contain abundant crypts lined by well-differentiated goblet or absorptive
epithelial cells, separated by a scant lamina propria. The vast majority of hyperplastic polyps
have no malignant potential.
Juvenile polyps
are essentially hamartomatous proliferations, mainly of the lamina propria,
enclosing widely spaced, dilated cystic glands. They occur most frequently in children younger
than 5 years old but also are found in adults of any age; in the latter group they may be called
retention polyps
. usually large in children (I to 3 cm in diameter) but smaller in adults.
In general, they occur singly and in the rectum, and being hamartomatous they have no
malignant potential. Juvenile polyps may be the source of rectal bleeding and in some cases
become twisted on their stalks to undergo painful infarction.
Neoplastic polyp (Adenomas):
Adenomas are neoplastic polyps that range from small, often pedunculated tumors to large
lesions that are usually sessile. Because the incidence of adenomas in the small intestine is
very low, this discussion focuses on those adenomas that arise in the colon.
Adenomatous lesions arise as the result of epithelial proliferation and dysplasia, which may
range from mild to so severe as to represent transformation to carcinoma.
3
Adenomatous polyps are segregated into three subtypes on the basis of the epithelial
architecture:
Tubular adenomas: mostly tubular glands.
Villous adenomas: villous projections
Tubulovillous adenomas: a mixture of the above .
Tubular adenomas are by far the most common; 5% to 10% of adenomas are tubulovillous,
and only 1% are villous.
The malignant risk with an adenomatous polyp is correlated with three interdependent
features:
1. Polyp size,
2. Histologic architecture
3. Severity of epithelial dysplasia, as follows:
ⱴ Cancer is rare in tubular adenomas smaller than 1 cm in diameter.
ⱴ The likelihood of cancer is high (approaching 40%) in sessile villous
adenomas more than 4 cm in diameter.
ⱴ Severe dysplasia, when present, is often found in villous areas.
MORPHOLOGY
Tubular adenomas
Histologically the stalk is covered by normal colonic mucosa but the head is composed of
neoplastic epithelium.
All degrees of dysplasia may be encountered, ranging up to cancer confined to the mucosa
(intramucosalcarcinoma) or invasive carcinoma-like masses.
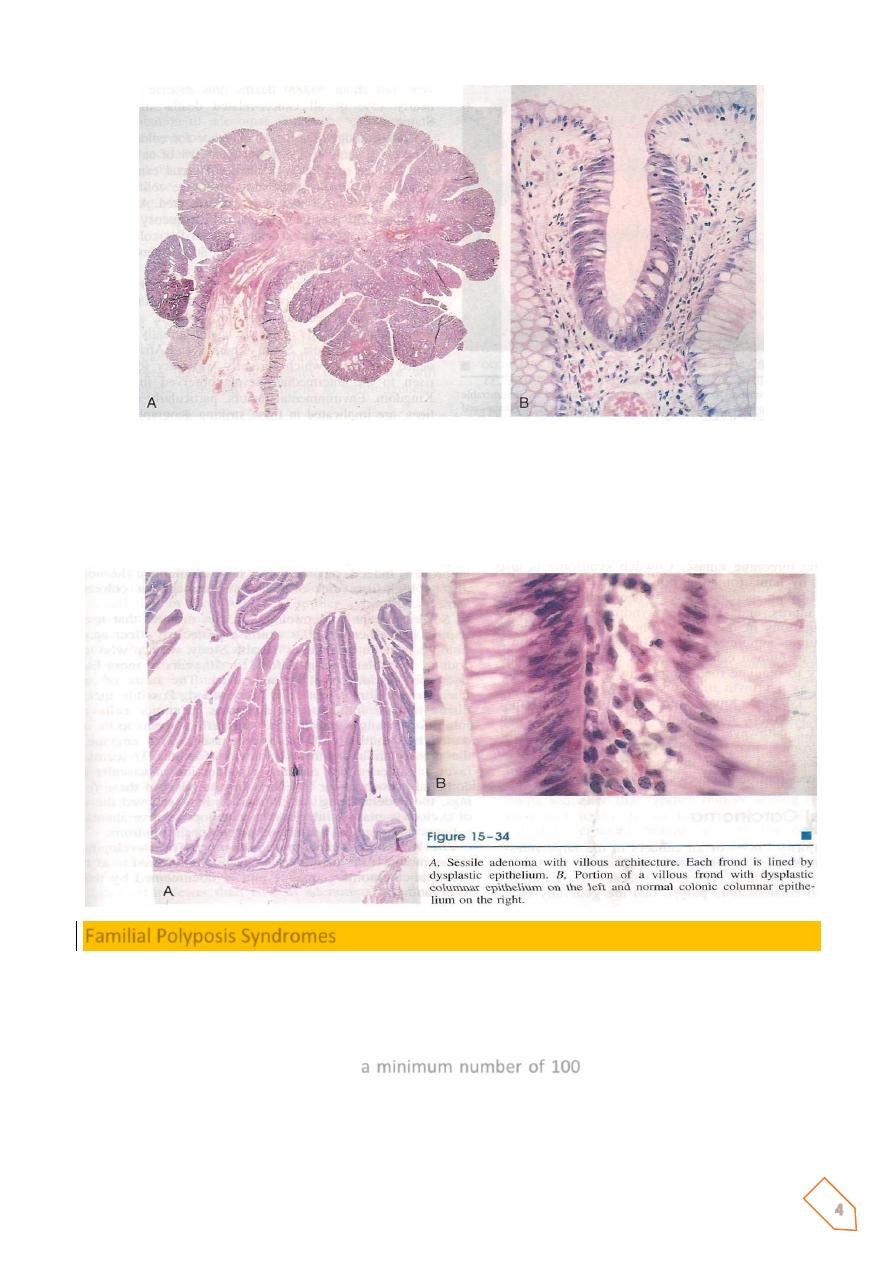
Villous adenomas
are larger and more ominous of the epithelial polyps. They tend to occur in
older persons, most commonly in the rectum and rectosigmoid. but they may be located
elsewhere. They generally are sessile covered by dysplastic, columnar epithelium. All degrees
of dysplasia may be encountered, and invasive carcinoma is found in up to 40% of these
lesions, the frequency being correlated with the size of the polyp.
Tubulovillousa denomos
are composed of a broad mix of tubular and villous areas. They are
intermediate between the tubular and the villous lesions in their frequency of having a stalk
or being sessile, their size, the degree of dysplasia, and the risk of harboring intramucosal or
invasive carcinoma.
4
Pedunculatcd adenoma showing a fibrovascular stalk covered by normal colonic mucosa and a head
that contains abundant dysplastic epithelial glands, hence the blue color. B, A small focus of
adenomatous epithelium in an otherwise normal (mucin-secreting. clear) colonic mucosa, showing
how the dysplasric columnar epithelium (deeply stained) can populate a colonic crypt (“tubular’
architecture).
Familial Polyposis Syndromes
Familial polyposis syndromes are uncommon autosmal dominant disorders. Their importance
lies in propensity for malignant transformation.
In familial adenomatous polyp (FAP), patients typically develop 500 to 2500 colonic adenomas
that carpet the mucosal surface ;
a minimum number of 100
is required for the diagnosis.
Multiple adenomas may also be present elsewhere in the alimentary tract.
Most polyps are tubular adenomas; occasional polyps have villous features. Polyps usually
become evident in adolescence or early adulthood.

5
The risk of colonic cancer is
virtually
100% by midlife, unless a prophylactic colectomy is
performed. The genetic defect underlying FAP has been localized to the APC gene on
chromosome(5q2).
Colorectal Carcinoma
A great majority (98%) of all cancers in the large intestine are adenocarcinomas.
Epidemiology
• The peak incidence for colorectal cancer is 60 to 70 years of age.
• When colorectal cancer is found in a young person, preexisting ulcerative colitis or
one of the polyposis syndromes must be questioned.
• Males are affected more often than females.
• Colorectal carcinoma has a worldwide distribution, with the highest incidence rates
in the United States.
Environmental factors
, particularly dietary practices, are implicated in these striking
geographic contrasts.
The dietary factors receiving the most attention are
1. A low content of unabsorbable vegetable fiber
2. High content of refined carbohydrates,
3. A high fat content (as from meat),
4. Decreased intake of protective micronutrients such as vitamins A, C, and B.
It is theorized that reduced fiber content leads to decreased stool bulk, increased fecal
retention in the bowel, and an altered bacterial flora of the intestine. M
oreover, high fat intake enhances the synthesis of cholesterol and bile acids by the liver, which
in turn may be converted into potential carcinogens by intestinal bacteria. Refined diets also
contain less of vitamins A, C, and E, which may act as oxygen radical scavengers.

6
Several recent epidemiologic studies suggest that use of aspirin and other NSAIDs exerts a
protective effect against colon cancer.
MORPHOLOGY
About 25% of colorectal carcinomas are in the cecum or ascending colon, with a similar
proportion in the rectum and distal sigmoid. An additional 25% are in the descending colon
and proximal sigmoid; the remainder are scattered elsewhere.
Hence, a substantial portion of cancers is undetectable by digital or proctosigmoidoscopic
examination.
• Tumors in the proximal colon tend to grow as polypoid, exophytic masses.
Obstruction is uncommon.
• When carcinomas in the distal colon are discovered, they tend to be annular,
encircling lesions that produce so-called napkin-ring constrictions of the bowel and
narrowing of the lumen.
• All colon carcinomas are microscopically similar. Almost all are adenacarcinamas
that range from well-differentiated to undifferentiated, and anaplastic masses.
• Many tumors produce mucin which is secreted into the gland lumina or into
interstitium of the gut wall. Because these dissect through the gut wall, they
facilitate extension of the cancer and worsen the prognosis.
• Cancers of the anal zone are predominantly squamous cell in origin.
All colorectal tumors spread by direct extension into adjacent structures and by metastasis
through the lymphatics and blood vessels.
Serum markers for disease, such as elevated blood levels of
carcinoembryonic antigen,
are of
little diagnostic value, because they reach significant levels only after the tumor has achieved
considerable size and has very likely spread.
Moreover, “positive carcinoembryonic antigen levels may be produced by carcinomas of the
lung, breast, as well as non-neoplastic disorders .
Because APC mutations occur early in colon cancers, molecular detection of APC mutations
in epithelial cells, isolated from stools, is being evaluated as a diagnostic test.
The single most important prognostic indicator of colorectal carcinoma is the extent (stage)
of the tumor at time of diagnosis
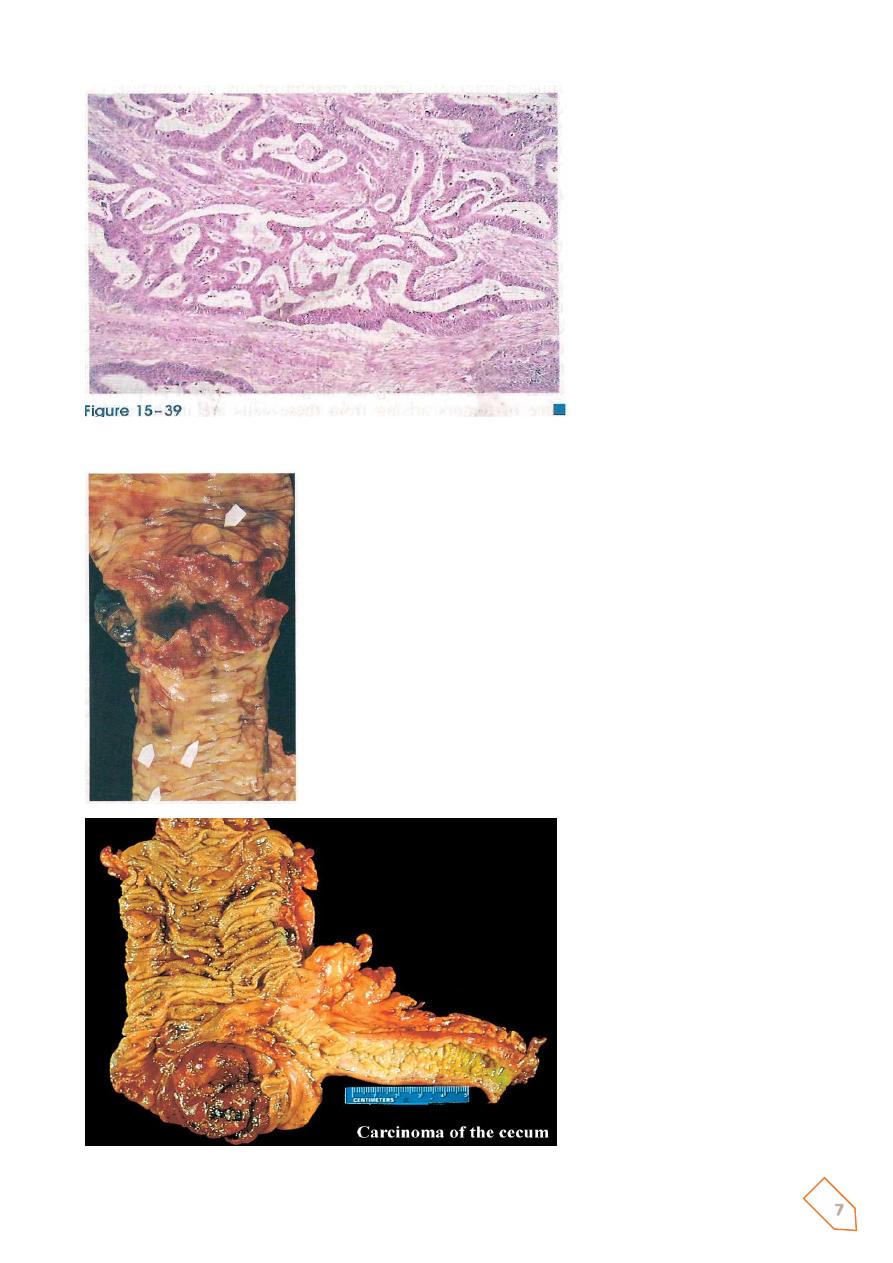
7
Invasive adenocarcinoma of
colon
showing
malignant
glands infiltrating the muscle
wall
Tumors in the proximal colon:
polypoid, exophytic masses
that extend along one wall of
the cecum and ascending
colon
8
This is an adenocarcinoma of the
cecum which demonstrates an
exophytic growth pattern, as the
bulk of the mass is within the
bowel lumen. The patient had
iron deficiency anemia.
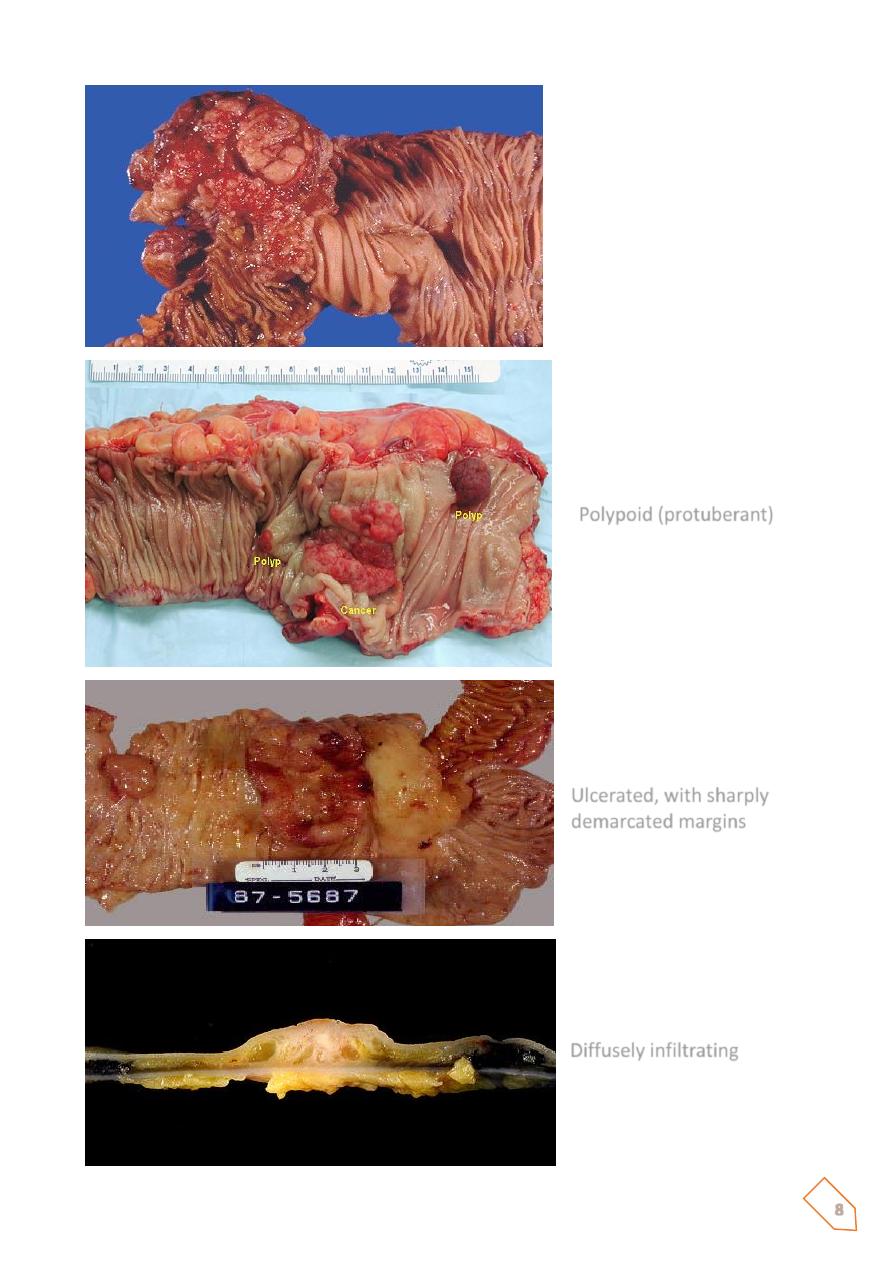
Polypoid (protuberant)
Ulcerated, with sharply
demarcated margins
Diffusely infiltrating
9
Colorectal Cancer and Early Detection
• Colorectal cancer can be prevented through regular screening and the removal of
polyps
• Early diagnosis means a better chance of successful treatment
• Screening should begin at age 50 for all “average risk” individuals or sooner if you have
a family history of colorectal cancer, symptoms, or a personal history of inflammatory
bowel disease
Mubark A. Wilkins
10
Notes