CSF CEREBROSPINAL FLUID
Dr. Haythem Ali AlsayighDepartment of human anatomy and histology
College of Medicine /University of Babylon
MB.CHB-F.I.M.B.S (Clinical surgical anatomy)
Objectives of this seminar
• Production , circulation and absorption of CSF• Function of CSF
• Composition of CSF
• What is Blood brain Barrier (BBB)
• Clinical application of the subject
• Practical knowledge
4
5
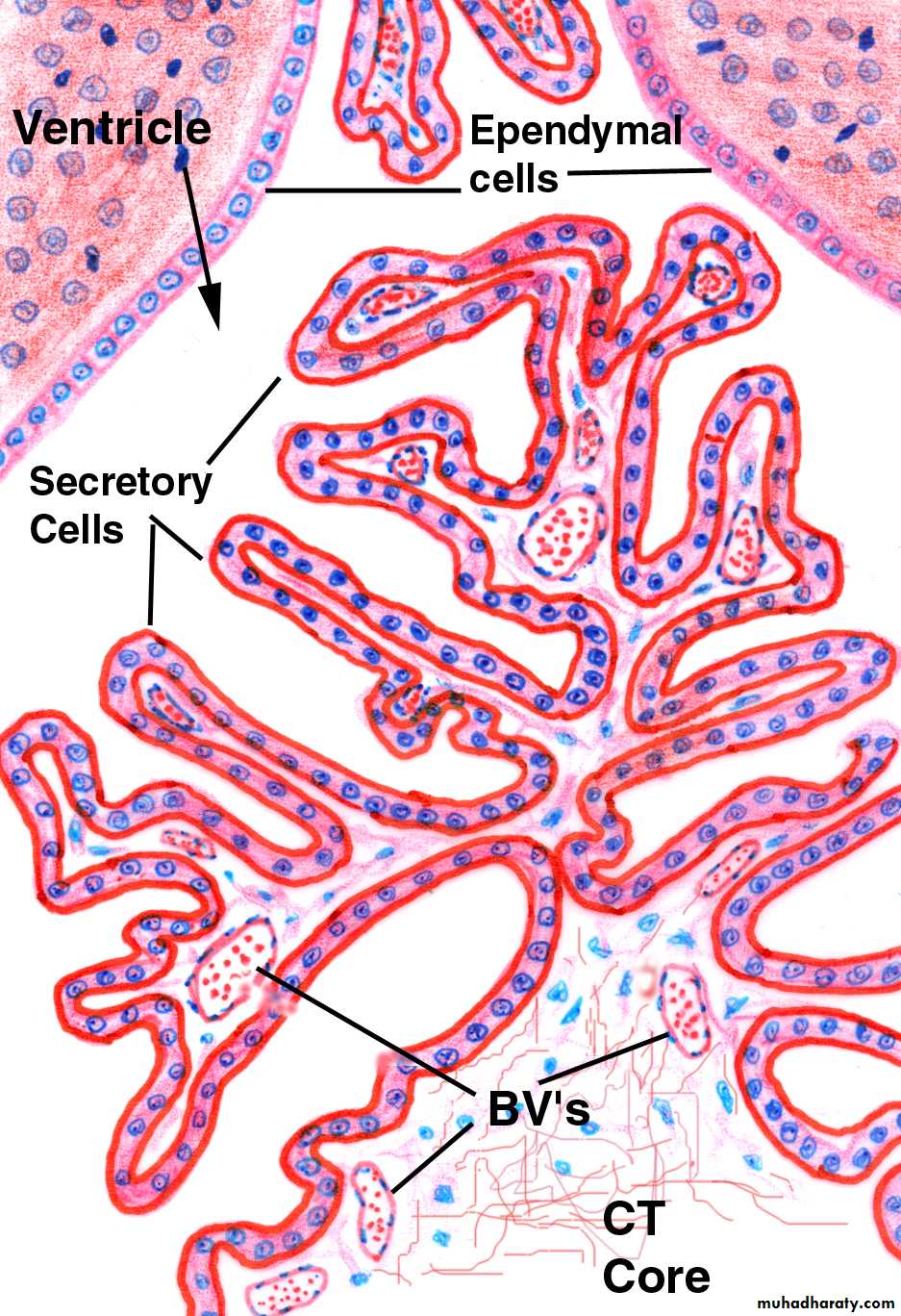
Choroid Plexus
6
7
Cerebrospinal Fluid
• Formation First recognized by Cotugno in 1764, CSF is the third major
• fluid of the body.
• CSF is formed in:
• Choroid plexus.
• Around blood vessels.
• Along ventricular walls.
8
Cerebrospinal Fluid
• CSF is absorbed by:
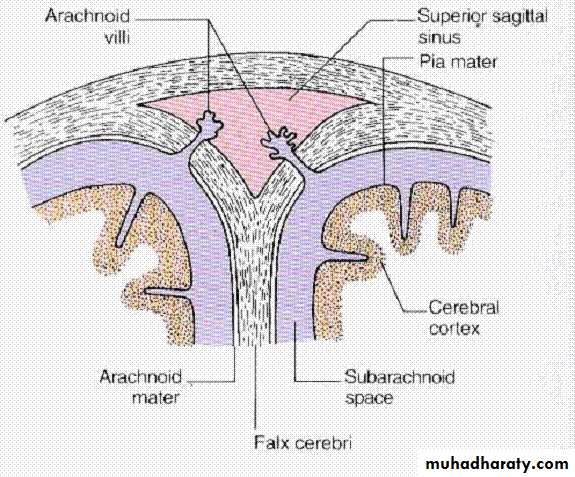
• Arachnoid villi
Secreted by choroid plexuses into each ventricle
Choroid plexus are areas where the lining wall of the ventricle is very thin and has a profusion of capillariesThe cerebrospinal fluid is formed mainly in the choroid plexuses of the lateral, third, and fourth ventricles;
some originates from the ependymal cells lining the ventricles
and from the brain substance through the perivascular spaces.
9
Cerebrospinal Fluid
Drainage
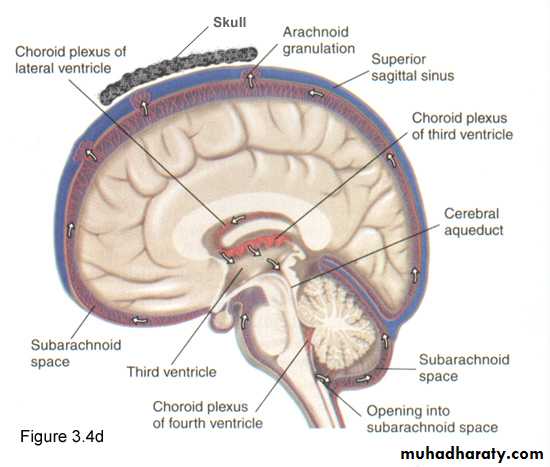
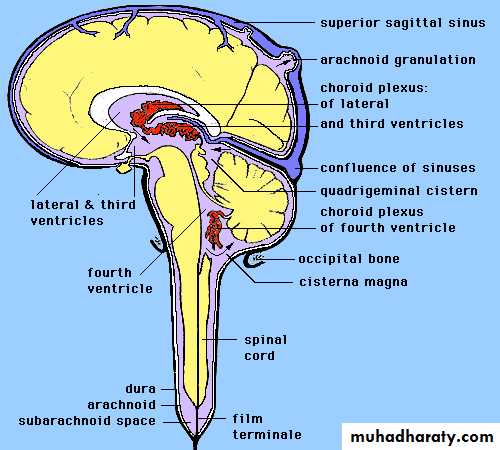
From the roof of the 4th ventricle CSF flows through foramina into the subarachnoid space and completely surrounds the brain and spinal cord10
Cerebrospinal Fluid
When CSF pressure is higher than venous pressure CSF passes into the blood and when the venous pressure is higher the arachnoid villi collapse, preventing the passage of blood constituents into the CSF
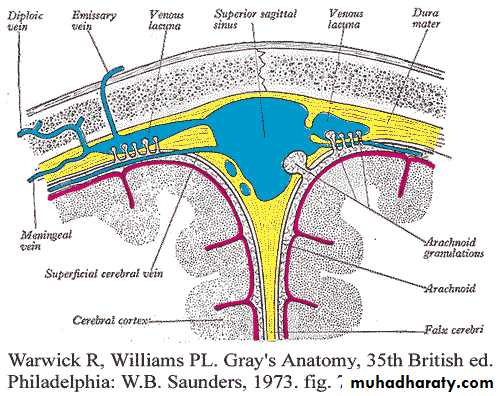
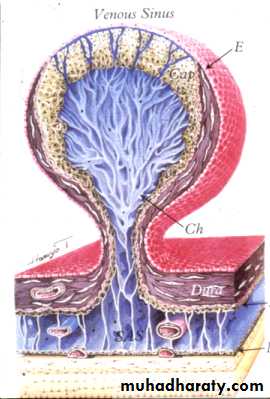
The CSF passes back into blood through tiny diverticula of arachnoid mater called arachnoid villi (arachnoid granulations), which project into the venous sinuses
Some reabsorption of CSF by cells in the walls of the ventricles occurs
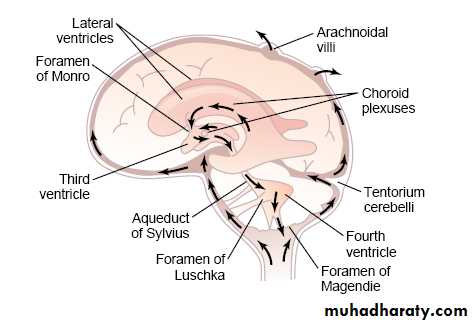
Circulation• The circulation begins with its secretion from the choroid plexuses in the ventricles
• The fluid passes from the lateral ventricles into t third ventricle through the interventricular foramina
• It then passes into the fourth ventricle through the narrow cerebral aqueduct.
• The circulation is aided by the arterial pulsations of the choroid plexuses and by the cilia on the ependymal cells lining the ventricles.
• From the fourth ventricle, the fluid passes slowly through the median aperture and the lateral foramina of the lateral recesses of the fourth ventricle and enters the subarachnoid space
CSF Circulation
lateral ventricles--> foramen of Monro— <third ventricle --> aqueduct of Sylvius -->
fourth ventricle --> foramina of Magendie and Luschka -->
subarachnoid space over brain and spinal cord -->
reabsorption into venous sinus blood via arachnoid granulations
13
Force of circulation
Movement of the CSF is by pulsating blood vessels, respiration and changes of posture
CSF is secreted continuously at a rate of about 0.5ml per minute i.e. 720 ml per day
Total CSF in the brain 120 ml
CSF pressure can be measured by attaching a vertical tube to the lumbar puncture needle – 10 cm water
CSF Production
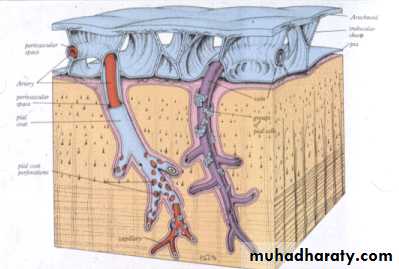
Virchow-Robin spaces• CSF Production
• 70 % CSF produced in choroid plexuses of lateral, third and fourth ventricles• CSF flows through the subarachnoid space between the arachnoid and pia mater
• produced at rate of 500 cc/day or approximately 20cc/hour (0.3-0.5 cc/kg/hr)
CSF Production
• The secretion of fluid by the choroid plexus depends on the active Na+-transport across the cells into the CSF.• The electrical gradient pulls along Cl-, and both ions drag water by osmosis.
• The CSF has lower [K+], [glucose], and much lower [protein] than blood plasma, and higher concentrations of Na+ and Cl-.
• The production of CSF in the choroid plexuses is an active secretory process, and not directly dependent on the arterial blood pressure.
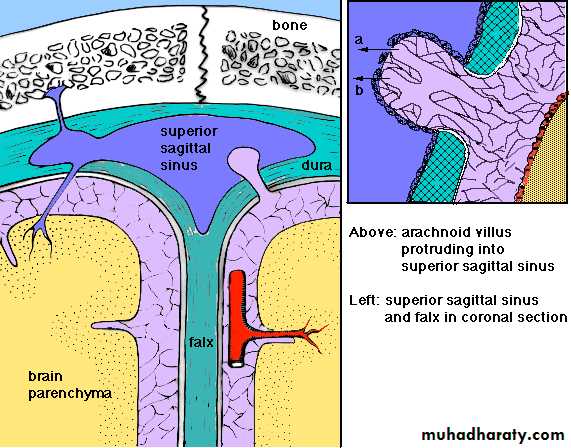
Arachnoid Villus
CSF Absorption
eliminated by being absorbed into the arachnoid villi --> dural sinus --> jugular systemCSF is reabsorbed into the blood of the venous sinuses via the arachnoidal villi. The absorption here is directly related to the CSF pressure in the cranial cavity.
Lymphatics/cribiform plate
Transependymal flow
Route and Absorption of CSF
Arachnoid villi are microscopic one-way valves (modified pia and arachnoid) that penetrate the meningeal dural layer that line the sinuses; hence, arachnoid villi reside within the sinuses (especially the superior sagittal sinus).Clumps of arachnoid villi = arachnoid granulations = macroscopic.
Route and Absorption of CSF
Hydrostatic pressure in subarachnoid space > pressure in dural sinusesTypical hydrostatic values of CSF are 150 mm H2O (11 mm Hg) in subarachnoid space vs. about 70 mm H2O (5 mm Hg) in dural sinuses.
Arach. villi are one-way valves that open when the hydrostatic pressure of CSF in the subarachnoid space is about 1.5 mm Hg greater than venous hydrostatic pressure in the dural sinuses (i.e., passive process).
CSF Functions
provide mechanical protection Cushion and protect the CNS from trauma.
maintain a stable extracellular environment for the brain Serves as reservoir and assistant in the regulation of the content of the skullRemove some waste products
Nutrition the CNS
Convey messages? (hormones/releasing factors/neurotransmitters) Serves as pathway for pineal secretion to reach the pituitary gland. it is involved in intra-cerebral transport, ex. hypothalamic releasing factors
CSF Functions
It protects against acute changes in arterial and venous blood pressureProvides mechanical buoyancy((تعويم_ and support for the brain
Blood brain Barrier (BBB)
It is formed by the tight junctions between capillary endothelial cells of the brain and between epithelial cells in the choroid plexus.This effectively prevents proteins from entering the brain in adults and slow the penetration of smaller molecules.
Mechanisms of transport:
Bulk flow.
Carrier mediated transfer
Vesicular transport.
Penetration of substances into the brain
Molecules pass easily:H2O, CO2, O2, lipid-soluble free forms of steroid hormones.Molecules not pass: proteins, polypeptides.
Slow penetration: H+, HCO3-
Glucose : its passive penetration is slow, but is transported across brain capillaries by GLUT1
Functions of BBB
Maintanins the constancy of the environment of the neurons in the CNS.
Protection of the brain from endogenous and exogenous toxins.
Prevent escape of the neurotransmitters into the general circulation.
Development of BBB
Premature infants with hyperbilirubinemia, free bilirubin pass BBB, and may stain basal ganglia causing damage (Kernicterus).Clinical implications
Some drugs penetrate BBB with difficulty e.g. antibiotics and dopamine.BBB breaks down in areas of infection, injury, tumors, sudden increase in blood pressure, and I.V injection of hypertonic fluids.
Injection of radiolabeled materials help diagnose tumors as BBB is broken down at tumor site because of increased vascularity by abnormal vessels.
28
Applied Anatomy
TB meningitis – block of aqueduct of Sylvius - hydrocephalus
Some pathological condition
• Increase of CSF pressure often caused by large tumor that elevate the CSF pressure by decreasing reabsorption of CSF back into the blood .•
• CSF pressure also rises when hemorrhage or infection .
• In this case large number of red and white blood cells appear in CSF and They can cause blockage of small absorption channels throw the arachnoidal villi .
• Some congenital condition may cause high pressure of CSF caused by few number of arachnoidal villi or abnormal proprieties of the villi
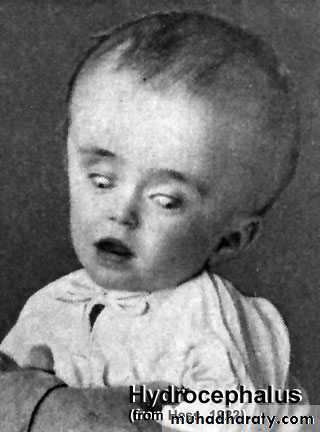
Hydrocephalous
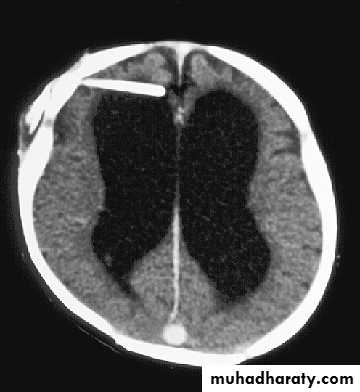
• accumulation of cerebrospinal fluid (CSF) in the ventricles, or cavities, of the brain .
• two types :
• communicating hydrocephalous :
• fluid flows from the ventricular system into the subarachnoid space.
• In communicating type blockage is in the subarchnoid space by blockage of arachnoidal villi themselves .
• Hydrocephalous
• Non communicating :• Fluid cant pass to the subarachnoid space
• In this type is blockage of the aqueduct of sylvius .
• Obstruction of villi blockage ↑ CSF pressure hydrocephalous may lead to edema .

33
Normal Brain

34
Normal Ventricles

35
Hydrocephalus

36
Hydrocephalus
37
Normal ventricles and hydrocephalus
Drugs affecting Rate ofCSF Production
DrugsCarbonic anhydrase inhibitors (acetozolamide/Diamox)
Cardiac glycosides (digoxin) inhibit ATPase pump, thereby reducing CSF formation in a dose-dependent manner.
Steroids- Effects on CSF formation are inconsistent.
Future- AqP inhibitors?, 5-HT2C receptor inh ?
Causes of an increased ICP
Conditions Increasing Brain Volumeintracranial mass (tumor, hematoma, aneurysm, AVM)
cerebral edema
CNS infection (abscess, inflammatory process)
Causes of an increased ICP
Conditions Increasing Blood Volumeobstruction of venous outflow
hyperemia – decreased pO2- inc. CBF
hypercapnea – >pCO2 increases vasodilation inc CBV , CBF, and ICP
Causes of an increased ICP
Conditions Increasing CSF Volumeincreased production(Choroid plexus papilloma)
decreased reabsorption of CSF (meningitis, SAH)
Obstruction to flow of CSF (e.g. aq stenosis)
Practical
Specimen Collection and handling
CSF is collected by lumbar puncture between third, fourth, fifth lumbar vertebrae. It requires certain precautions and careful technique to prevent the introduction of infection or the damaging of neural tissue.
CSF usually collected in three sterile tubes
Label 1 / Tube 1 – used for chemical and serologic test
( tubes are frozen)
Label 2 / Tube 2 – used for microbiology lab
( room temp.)
Label 3 / Tube 3 – used for hematology (cell count)
( refrigerated)
Normal and Pathological Findings
- The general appearance of CSF is clear and colorless, because it is more than 99% water. Color of CSF is observed only in pathological circumstances.- A yellowish tinge can be found with any cause of a markedly increased protein (greater than 200mg per 100mL).
xanthochromic (yellow) - If there is no liver failure (jaundice can cause CSF to be yellow), xanthochromic CSF suggests that a subarachnoid hemorrhage has recently occurred [within days).
The yellow color is due to bilirubin generated in the CNS by the breakdown of hemoglobin released from ABC's.
APPEARANCE
Major terminology used to describe CSF appearance:
Crystal clear
Cloudy or turbid – result of an increased protein or lipid conc/presence of WBC
milky
hemolyzed / bloody
xanthochromic – supernatant is pink, orange, or yellow
pink – very slight amount of oxyhemoglobin
orange – heavy hemolysis
yellow – conversion of oxyhemoglobin to unconjugated bilirubin
* other causes:
Elevated serum bilirubin
Presence of the pigment carotene
Markedly increase protein concentration
Melanoma pigment
TRAUMATIC COLLECTION
Grossly bloody CSF can be an indication of intracranial hemorrhage or due to the puncture of a blood vessel during spinal tap procedure (traumatic tap)UNEVEN DISTRIBUTION OF BLOOD
From the three test tubes whereas the heaviest concentration of blood was in the first tube then gradually diminishing amounts in tube 2 and 3.
CLOT FORMATION
Meningitis, Froin’s syndrome, and blockage of CSF circulation through subarachnoid space
XANTHOCHROMIC SUPERNATANT
Additional testing for differentiation includes microscopic examination and the D-dimer test
CELL COUNT
RBC and WBC count
METHODOLOGY
Normal adult 0 – 5 WBCs/µL
Children 30 mononuclear cells/µL ( 200WBC/ 400RBCs)
TOTAL CELL COUNT
WBC COUNT
CORRECTIONS FOR CONTAMINATION
QUALITY CONTROL OF CSF AND OTHER BODY FLUID CELL COUNTS
DIFFERENTIAL COUNT ON A CSF SPECIMEN
Identifying the types of cells in the CSF is a valuable diagnostic aid.the differential count should be performed on a stained smear and not from the cells in the counting chamber. Poor visualization of the cells as they appear in the counting chamber led to the laboratory practice of reporting only the percentage of mononuclear and polynuclear cells present.CSF CONSTITUENTS
Cells found in normal CSF are lymphocytes and monocytesPleocytosis is considered abnormal cells.
WBC count majority of the cells are neutrophils considered bacterial meningitis. And if moderately high percentage o flymphocytes and monocytes, meningitis of viral, tubercular, fungal, or parasitic origin.
CSF CONSTITUENTS
Cells found in normal CSF are lymphocytes and monocytesPleocytosis is considered abnormal cells.
WBC count majority of the cells are neutrophils considered bacterial meningitis.
And if moderately high percentage of lymphocytes and monocytes, meningitis of viral, tubercular, fungal, or parasitic origin.
Composition of CSF
In addition to the major ions, CSF contains oxygen, sugars (e.g., glucose, fructose, polyols), lactate, proteins (e.g., albumin, globulins), amino acids, urea, ammonia, creatinine, lipids, hormones (e.g., insulin), and vitamins.
Substance
PlasmaCSF
Sodium (mEq/L)
140.0
144.0
Potassium (mm/L)
4.6
2.9
Magnesium (mEq/L)
1.6
2.2
Calcium (mg/dL)
8.9
4.6
Chloride (mEq/L)
99.0
113.0
Bicarbonate (mm/L)
26.8
23.3
Inorganic phosphate (mg/dL)
4.7
3.4
Protein (g/dL)
6.8
0.028 (28mg/dL)
Glucose (mg/dL)
110.0
50 to 80
Osmolality
0.3
0.29
pH
7.4
7.3
Pco2 (mmHg)
41.1
50.5
• CSF
• SERUM
• RATIO
• mg/dl
• mg/dl
• Prealbumin
• 1.7
• 23.8
• 14
• Albumin
• 15.5
• 3600
• 236
• Ceruloplasmin
• 0.1
• 36.6
• 366
• Transferrin
• 1.4
• 204
• 142
• Immunoglobulin G
• 1.2
• 987
• 802
• Immunoglobulin A
• 0.13
• 175
• 1346
CSF PROTEIN
CLINICAL SIGNIFICANCE OF ELEVATED PROTEIN VALUES
Elevated total protein values are most frequently seen in pathologic conditions. Abnormally low values will be present when fluid is leaking from the CNS. Cause of elevated CSF protein include the damage to the blood brain barrier
Protein fractions
Electrophoreseis
Myelin basic protein
CSF GLUCOSE
Glucose enters the CSF by selective transport across the blood-brain barrier, which result in a normal value that is approximately 60 – 70 percent that of the plasma glucose. The diagnostic significance of CSF glucose is confined to the finding of values that decreased in relation to plasma values.low CSF glucose can be considerable diagnostic value in determining the causative agents in meningitis.
• CSF LACTATE
• The determination of CSF lactate levels aid in the diagnosis and management of meningitis cases. In bacterial, tubercular and fungal meningitis.elevations of CSF lactate greater than 25mg/dl. Destruction of tissue within the CNS owing to oxygen deprivation (hypoxia) causes the production of increaded CSF lactic acid levels.• CSF GLUTAMINE
• Glutamine is produced in the CNS by the brain cells from ammonia and alpha-ketoglutarate. This process serves to remove the toxic metabolic waste product ammonia from the CNS. Normal concentration of ammonia is 8-18 mg/dl. Elevated levelsassociated with liver disorders.
• CSF ENZYMES
• LDH – LD1, LD2, LD3, LD4, LD%
• CK – BB
MICROBIOLOGY TEST
For positive identification, the microorganism must be recovered from the fluid by growing it on the appropriate culture medium. Can take 24 hrs I cases of bacterial meningitis to 6 weeks for tubercular meningitis. In many instances, CSF culture is actually a confirmatory testGRAM STAIN
Is routinely performed on CSF from all suspected cases of meningitis although its value lies on the detection of bacterial and fungal organisms.
Organisms most frequently encountered:
S. pneumoniae (gram positive cocci)
H. influenzae ( pleomorphic gram negative rods)
E. coli (gram negative rods)
Acid-fast is not routinely performed on specimens unless tubercular menoingitis is suspected.
Latex Agglutination and ELISA provides a rapid means for detecting microorganisms in CSF.
• SEROLOGIC TESTING• Serologic testing of the CSF is performed to detect the presence of neurosyphilis. However, detection of the antibodies associated with syphilis in the CSF still remains a necessary diagnostic procedure.
• Serologic tests:
• VDRL
• FTA –ABS
• TEACHING CSF ANALYSIS
• Many of the problems that occur in the analysis of CSF are result of inadequate training of the personnel performing the tests. This is considered that not only is CSF is difficult to collect.