1
Thyroid gland
L2
It is a bilobed structure lies below and anterior to larynx structurly consist of follicles
lined by low cuboidal – columnar epithelium and filled by thyroglobulin rich colloid,
which's is converted by follicular cells as T3 and T4, realse to circulation and interact
with intracellular receptors to up-regulate of CHO and lipid catabolism, and protein
synthesis so cause increase basal metabolic rate.
Between these follicles there are parafollicular cells secrete calcitonin hormone which's
promotes absorption of calcium by skeletal system and inhibits resorption of bone by
osteoclast.
Diseases of thyroid glands:
1- overproduction (thyrotoxicosis)
2- hypothyroidism
3- thyroiditis.
4- neoplasia.
I- Thyrotoxicosis:
Is a hypermetabolic state caused by elevation circulating levels of free T3 &T4 .
The causes of thyrotoxicosis:
1- Primary overproduction
by thyroid gland itself which's the most common cause.
2- secondary overproduction
by realse of TSH from pituitary or realsing factors
from hypothalamus which's a minor cause.
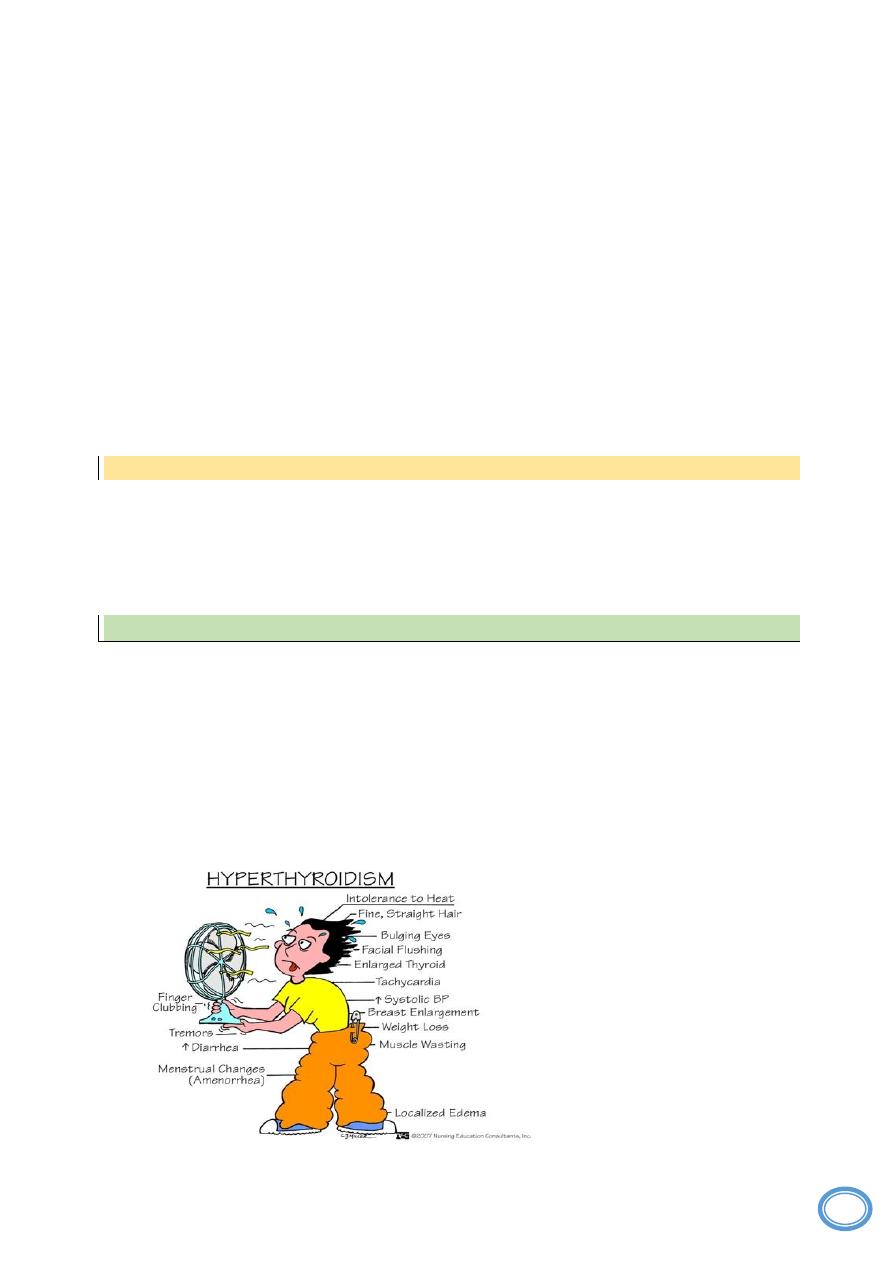
The clinical features
of thyrotoxicosis are related to hypermetabolic state indused by
excess thyroid hormones, so cause weight loss inspite of increase appetite, heat
intolerance, the skin is soft, warm and flushed, diarrhea, palpitation and tachycardia.
2
Diagnosis of hyperthyroidism:
Depend on
1-clinical features
2-laboratory data
the measurement of
a- Serum TSH concentration is a sensitive assay provides the most useful single
screening test for hyperthyroidism causing decrease it's level because of feed back
inhibition which's usually increase in case of secondary hyperthyroidism caused by
pituitary or hypothalamic over stimulation.
b- measurement of T3&T4 which are increased.
3- Measurment of radioactive iodine
uptake which's cause diffuse uptake of iodine in
cases of primary hyperyhyroidism.
Hypothyroidism:
Is decreased in level of thyroid hormones also caused by:
1. primary cause
is the most common cause occur in cases of :
a. Ablation of the thyroid by surgery or radiation therapy.
b. Hashimoto's thyroiditis.
c. primary idiopathic hypothyroidism.
2. secondary cause
due to decrease of TRH or TSH from hypothalamus and
pituitary resepectively.
Clinical features of hypothyroidism:
Include cretinism and myxedema .
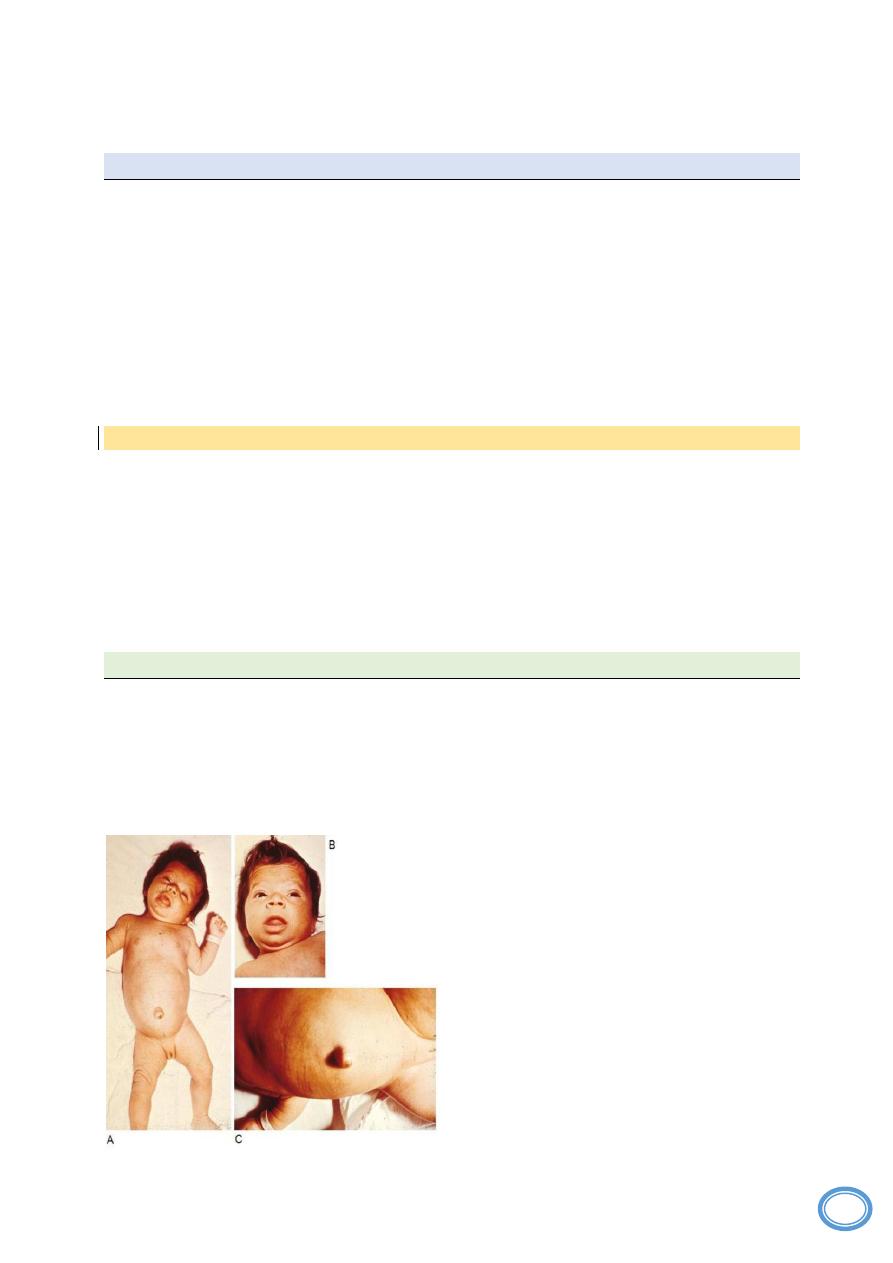
1- Cretinism
is hypothyroidism developing in infancy or early childhood caused by
hypothyroidism of mother during pregnancy, because the child take thyroid hormones in
1
st
months of his development in uterus from mother this cause impaired development
of skeletal system, CNS and mental retardation, so the baby have short stature, coarse
fascial feature and protruted tongue.
3
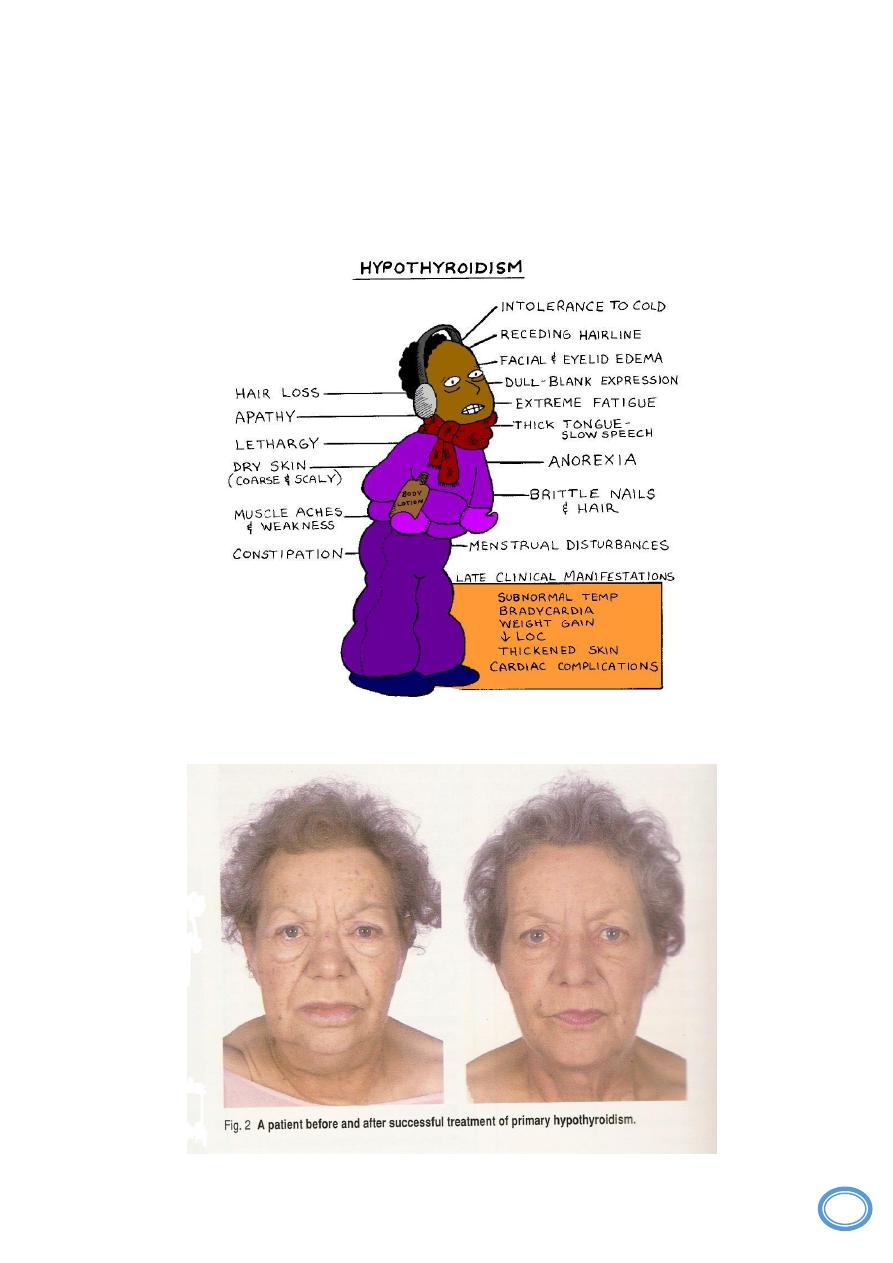
2- Myxedema:
occur in older children and adults cause mental sluggish, cold
intolerance, obesity, constipation and coarsening of fascial featues.
4
Diagnosis
depend on estimation of TSH which's increased with decreased level of
T3&T4.
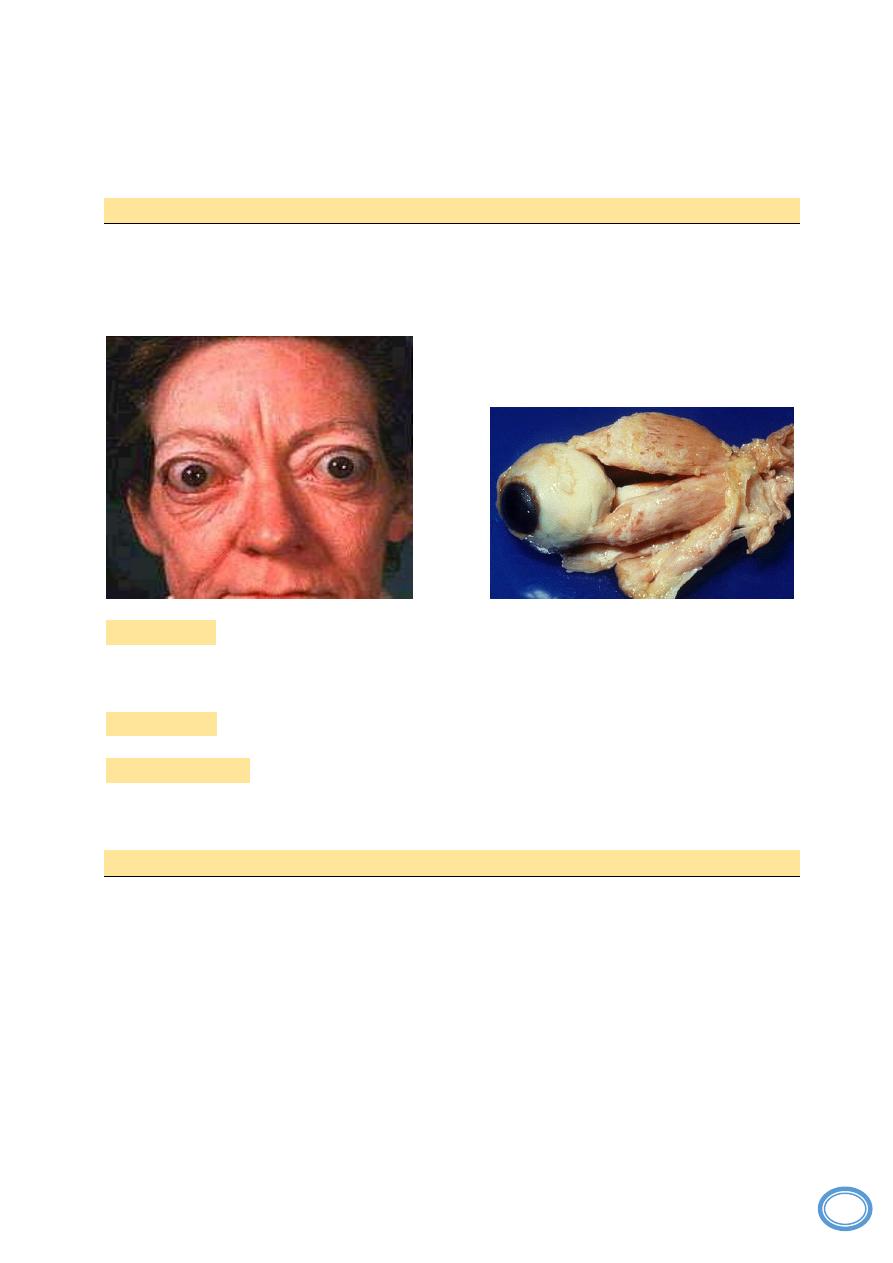
Grave's disease:
Is the most common cause of primary hyperthyroidism, this usually occur in young age
female 20-40 years, present with diffuse goiter (enlargement of thyroid gland) and
clinical features of thyrotoxicosis in addition to exophalamous because of muscular
hypertrophy.
Pathogensis:
It is an autoimmune disorder, different auto antibodies present in serum
most common are TSH receptors autoanti-body, which's act on TSH receptors of
follicular cells, causes over-stimulation and increased secretion of T3&T4.
Morphology:
diffuse symmetrical enlargement of thyroid gland, because of
hypertrophy and hyperplasia of follicular cells.
Microscopically:
proliferated follicles lined by tall columnar active follicular cells
with forming of infolding, the follicles filled by pale colloid with scalloped margin, the
stroma infiltrated by B lymphocytes which are the source of auto Ab.
Diffuse non-toxic and multinodular goiter:
This is most common thyroid disease occur due to :
1- impaired synthesis of thyroid hormones due to dietary iodine deficiency.
2- increased thyroxin demand especially in young age female.
3- less commonly hereditary enzymatic defects that decreased thyroid
hormone synthesis
These cause compensatory rise in serum TSH level, hypertrophy and hyperplasia of
thyroid follicular cells, so cause enlargement of thyroid gland, when the cause subside
by iodine intake or decrease of demand to thyroxin, so the TSH level will return to
normal, the follicles enlarged and filled by colloid with lining by flat to cuboidal
follicular cells so cause diffuse colloid goiter or multinodular goiter.
5
Hormonal assay
at this stage reveal normal hormonal level or called authyroid, so signs
and symptoms of disease reveal only thyroid enlargement and pressure effect.
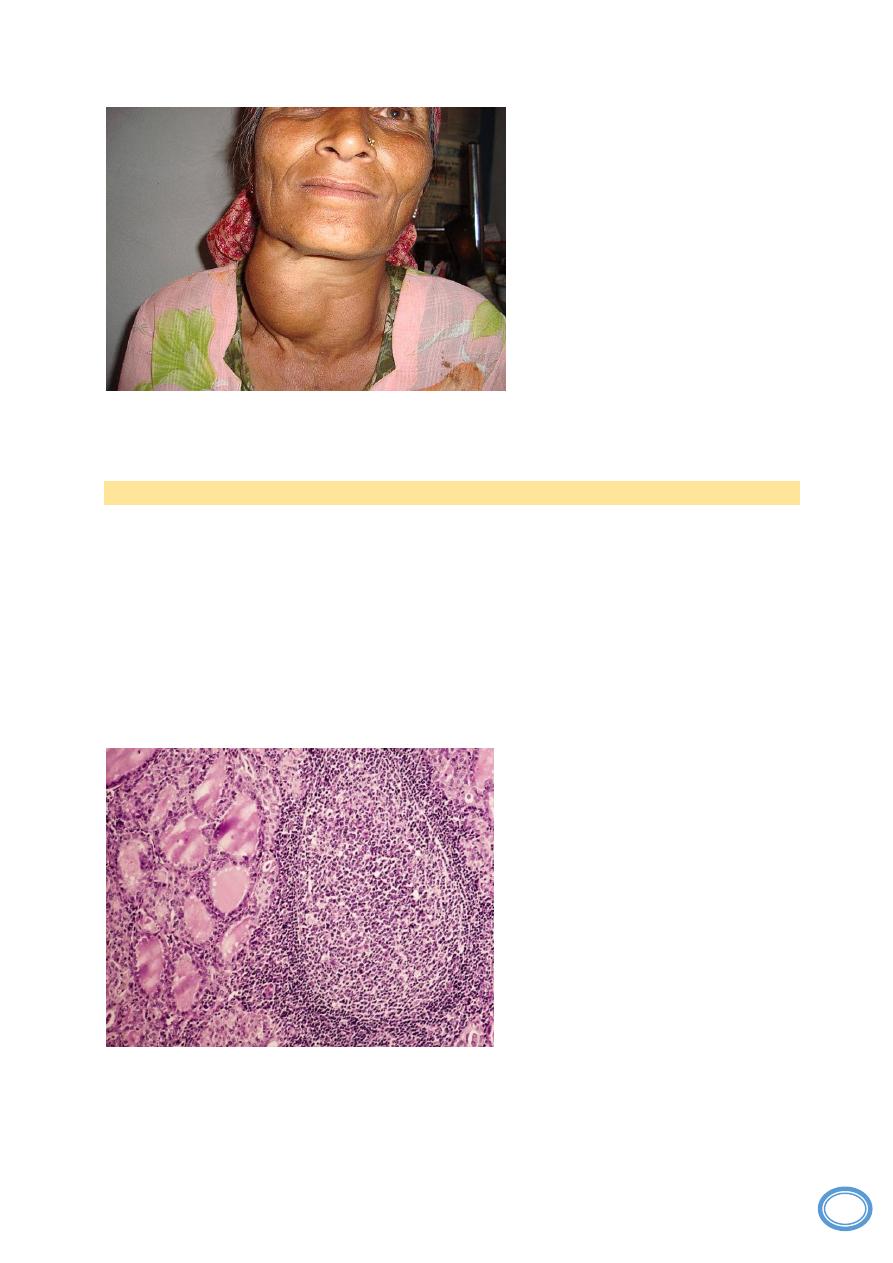
Thyroiditis:
The most common type of thyroiditis is
Hashimoto's thyroiditis
It is an auto-immune disorder, the serum of patient contain auto-anti TSH receptors Ab
like present in Grave's disease but block the action of TSH so cause hypothyroidism.
Morophology:
diffuse enlargement of thyroid gland.
Microscopically:
the stroma is heavily infiltrated by lymphocytes and plasma cells
forming lymphoid follicles with germinal center, the thyroid follicles are usually small,
lined by follicular cells having eosinophilic cytoplasm in some areas.
Clinical features:
the patient is
usually female present with diffuse,
painless enlargement of thyroid
gland
with
features
of
hypothyroidism, but in early stage of
disease
there
is
transient
thyrotoxicosis because of distruption
of thyroid follicles during this phase
hormonal assay reveal increased
level of T3&T4 with decline of TSH
level but radioactive iodine uptake is
diminished, during hypothyroidism
state there are decline in level of
T3&T4 with increased of TSH.