Baghdad College of Medicine / 5
th
grade
Student’s Name :
SURGERY
LEC.77
Dr.Firas AL-Obaidi
Lec.9
scolisis
DONE BY : Noor Ali
مكتب اشور لالستنساخ
2016 – 2017
Orthopedics
(40)
By Noor Ali Majeed
Spine deformities
Ass. Prof. Firas Alobaidi
Aim :
Scoliosis :
diagnosis and treatment
Kyphosis :
diagnosis and treatment
Ortho
=
straight
To make deformed children straight =
Ortho
pedic
To treat
Scoliosis
=
Ortho
pedic
Nicolas Andry from paris at 1741
Orthopedic symbol

2
skoliosis
means "a bending"
Paidion
=
Child
Loading...
Scoliosis
:
is an apparent lateral ( sideways ) curvature of the spine. ( more than 10 degrees )
it is
triplanar
deformity with anteroposterior , lateral and rotational ( axial ) components.
Scoliosis can be
postural
( non structural ) or
structural
.
Postural ( non structural ) scoliosis :
The deformity is secondary or compensatory to some conditions outside the spine such as
,short leg , pelvic tilt due to hip contracture.
when the patient sits ( canceling the leg length asymmetry ) the curve disappears.
Sciatic scoliosis, due to muscle spasm in acute disc prolapse.
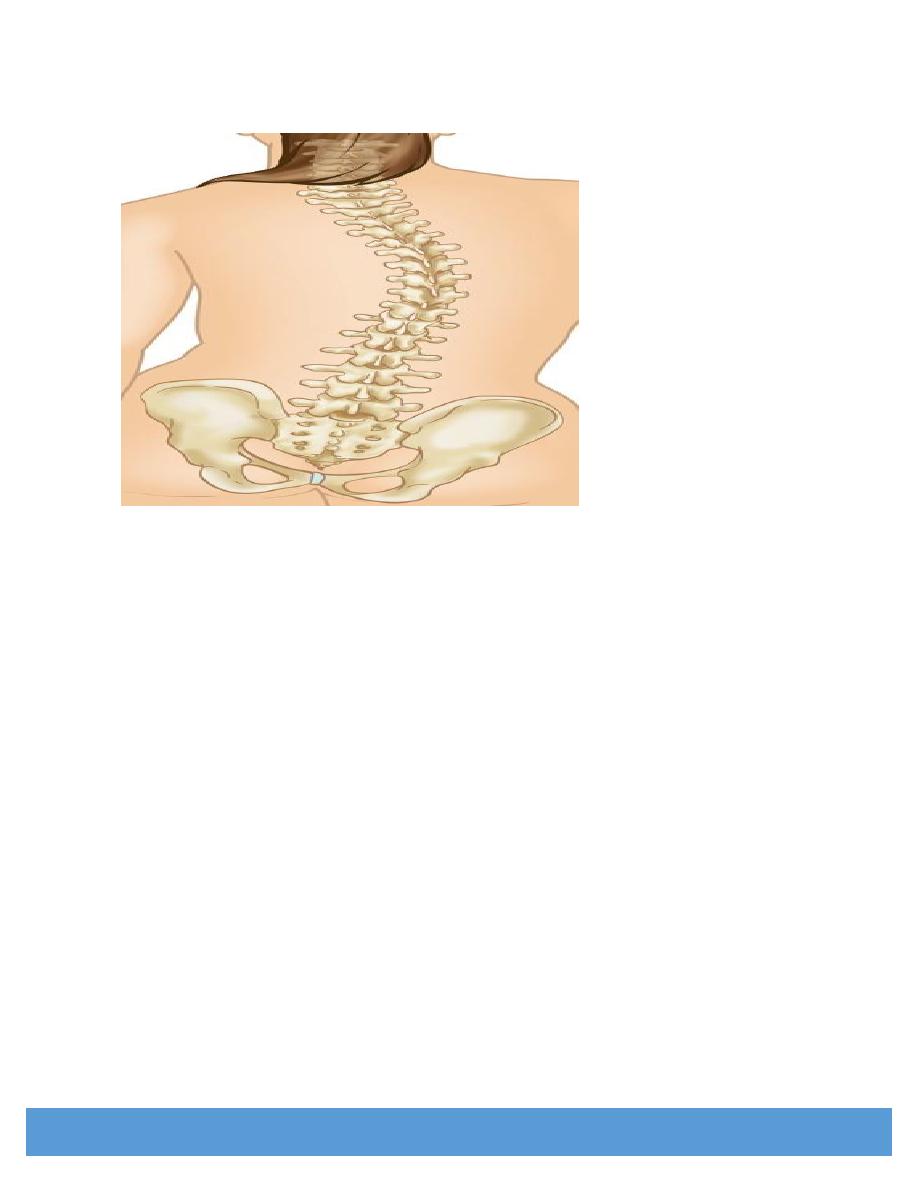
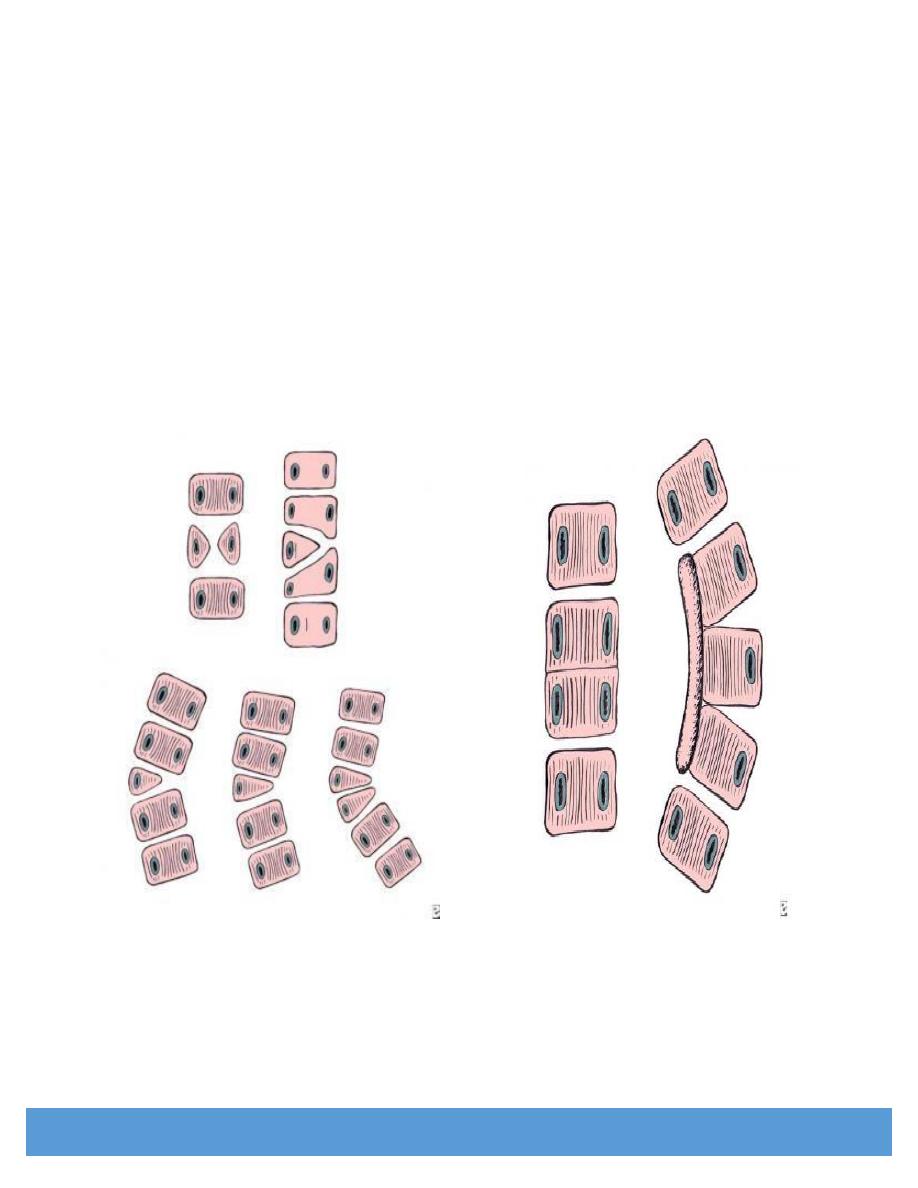
Structural scoliosis :
There is non correctable deformity ( by posture ) ,
an essential component of which is vertebral rotation.
The spinous processes go towards the concavity of the curve and the transverse processes
on the convexity rotate posteriorly.
In the thoracic spine , the ribs on the convex side stand out prominently, producing the
rib
hump
,
which is the characteristic part of the overall deformity.
Secondary
( compensatory ) curves nearly always develop to counterbalance the primary curves ,
they are usually less marked and more easily correctable , but with time they also become fixed.
Once fully established , the deformity is liable to increase throughout the growth period, thereafter,
further deterioration is slight though curves greater than
50
degrees may go on increasing by
1
degree per year.
With very severe curves, chest deformity is marked and
cardiopulmonary function is usually affected.
3
Types ( causes ) :
1-
Idiopathic scoliosis : there is no obvious cause
2-
Congenital or osteopathic : due to bone anomalies
3-
Neuropathic
4-
Myopathic : associated with some muscular dystrophy
5-
Degenerative (de novo scoliosis)
6-
Miscellaneous group of connective tissue disorders
Clinical features :
-
Deformity
is the usual presenting symptom.
-There may be obvious skew back , rib hump in the thoracic spine and
asymmetrical prominence of one hip in thoracolumbar curves.
-Balanced curves sometimes pass unnoticed until an adult presents with
backache.
-
Pain
is a rare compliant ( in children ) and if present , should alert the
clinician to the possibility of a neural tumor and the need for MRI.
- There may be family history of scoliosis.
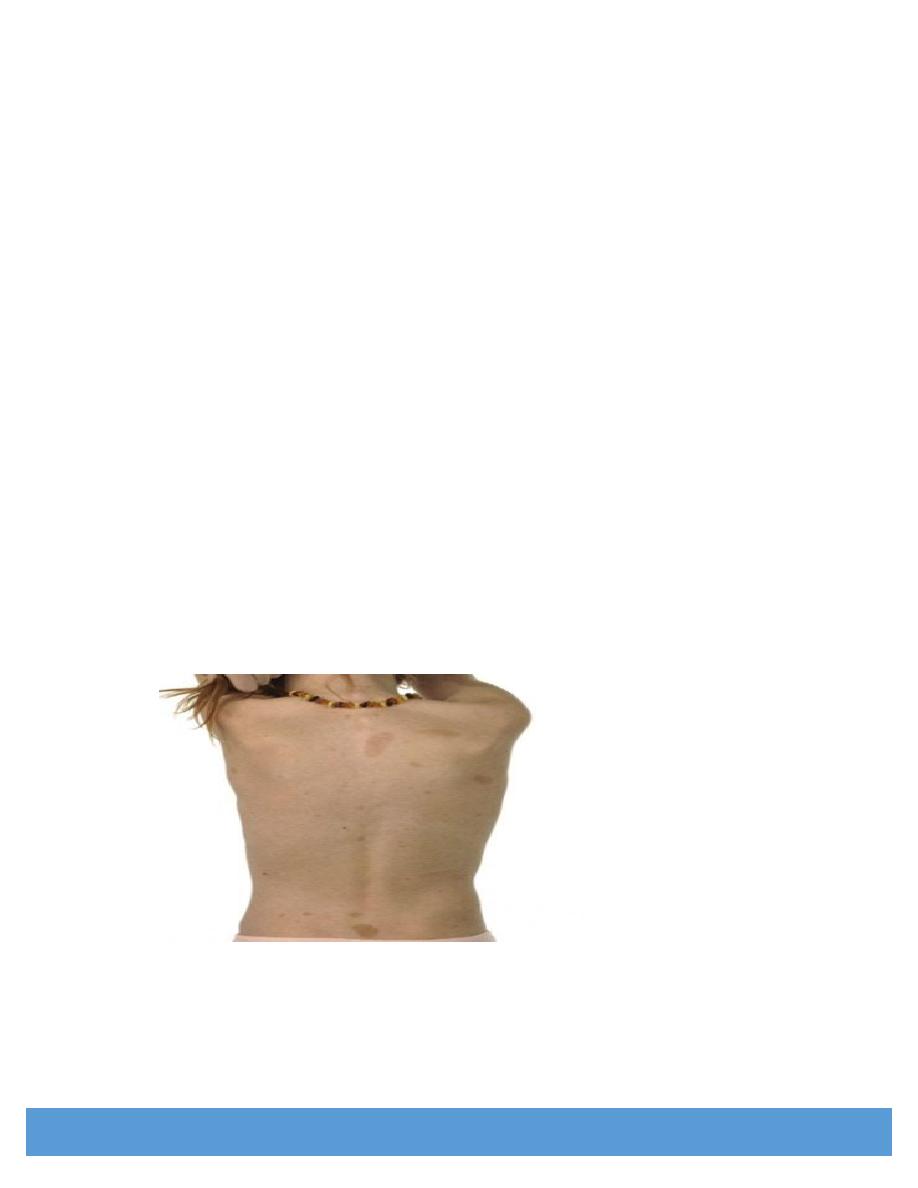
On examination , the trunk should be completely exposed.
-Skin pigmentation and congenital anomalies e.g. sacral dimples or hair
tufts can be seen.
4
Adams foreward bending test :
Forward bending makes the curve more obvious
The level and direction of the major curve convexity are noted,
e.g. right thoracic curve
means
a curve in the thoracic spine and convex to the right.
The hip ( pelvis ) sticks out on the concave side and the scapula on the convex.
The breasts and shoulders may be asymmetrical.
In the thoracic scoliosis , rotation causes the rib angles to protrude
, thus producing a symmetrical rib hump on the convex side of the curve.
Spine mobility should be assessed and the effect of lateral bending on the curve noted.
Side - on posture should also be observed , there may be excessive kyphosis or lordosis.
Full neurological examination is important.
General examination including the cardiopulmonary function .
5
Imaging :
X - Ray
: full length PA and lateral view of the spine and iliac crests must be
taken with the patient erect, and bending views.
Note that PA in relation to patient is not PA in relation to the rotated vertebrae.
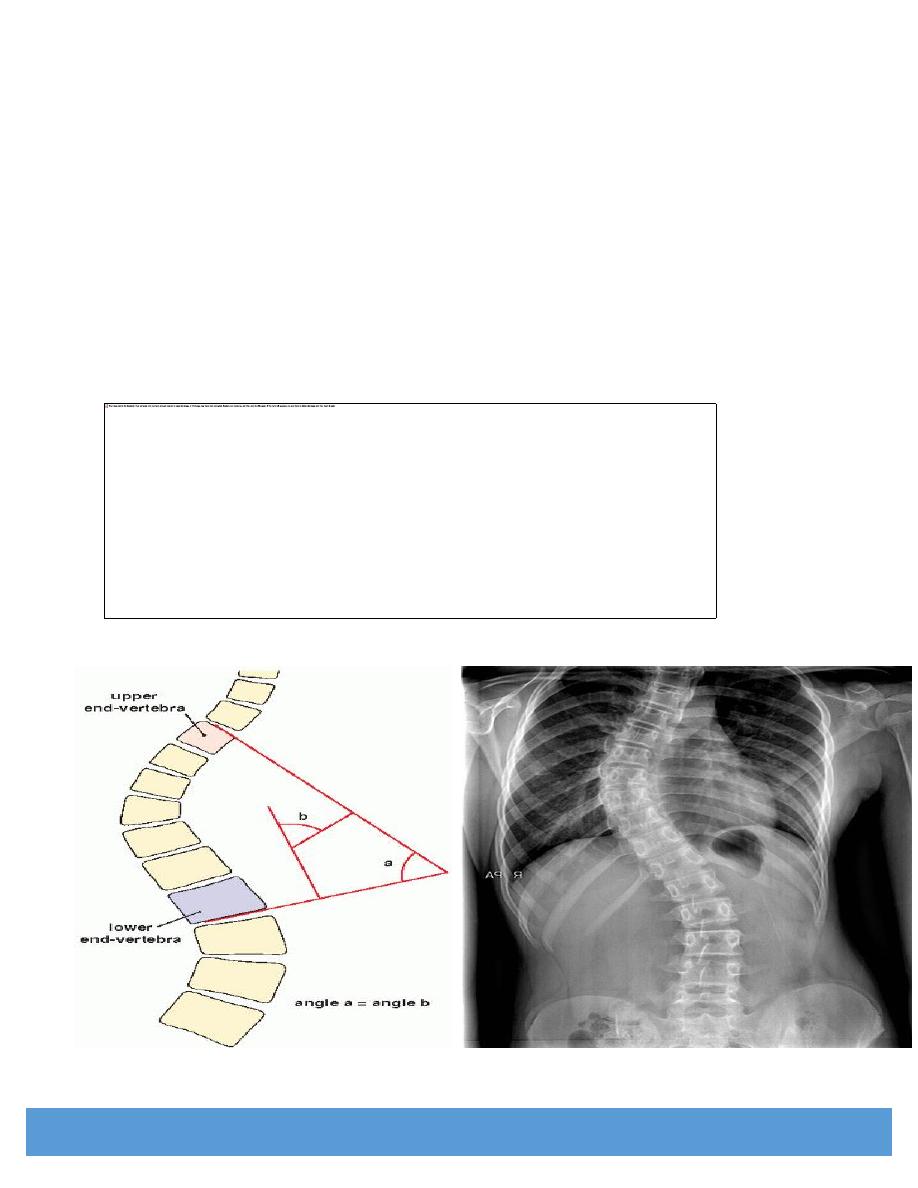
The upper and lower end vertebrae are the most tilted vertebrae in the upper and lower end
of the curve respectively.
Cobb s angle : is the angle of the curvature :
measured between the line drawn at the upper border of the upper end vertebra
and the line drawn at the lower border of the lower most vertebra.
6
Sometimes there are multiple primary curves.
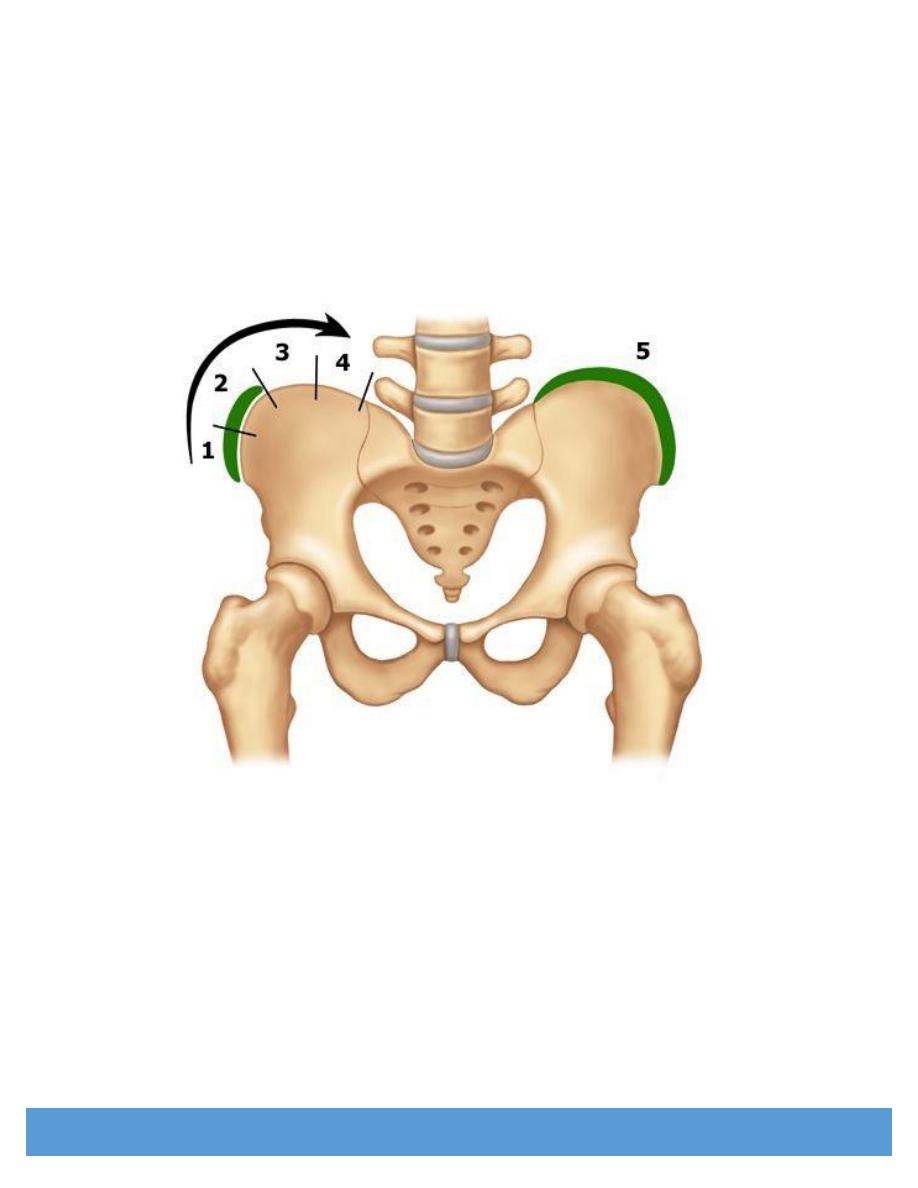
Risser s sign
: to assess skeletal maturity : from zero to 5 grades
This is important because the curve often progresses most during
the period of rapid skeletal growth and maturation.
The iliac apophyses start ossifying shortly after puberty , ossification extends medially and
, once the iliac crests are completely ossified, further progression of the scoliosis is minimal.
CT and MRI : may be necessary to show vertebral abnormality or cord
compression.
Note
: be careful of hazards of radiation , don't order unnecessary CT scan
or unnecessary x - ray repetition especially in children.
Pulmonary function test : especially in cases of severe thoracic curves.
Patients with muscular dystrophies or connective tissue disorders needs full biochemical
and neuromuscular investigation of the underlying condition.
7
Prognosis
: generally the younger the child and the higher the curve the worse the prognosis.
ScoliScore™ is a DNA test that can indicate the likelihood of progression into
a severe curve for children diagnosed with idiopathic scoliosis ( saliva test ) :
the patient s saliva is used
Idiopathic scoliosis :
This group forms about
80
%
of all cases of scoliosis. it is often familial.
The age at onset has been used to define three groups :
1- Infantile idiopathic scoliosis :
occurs in children aged 3 years or under.
- most curves are thoracic with convexity to the left ( left thoracic )
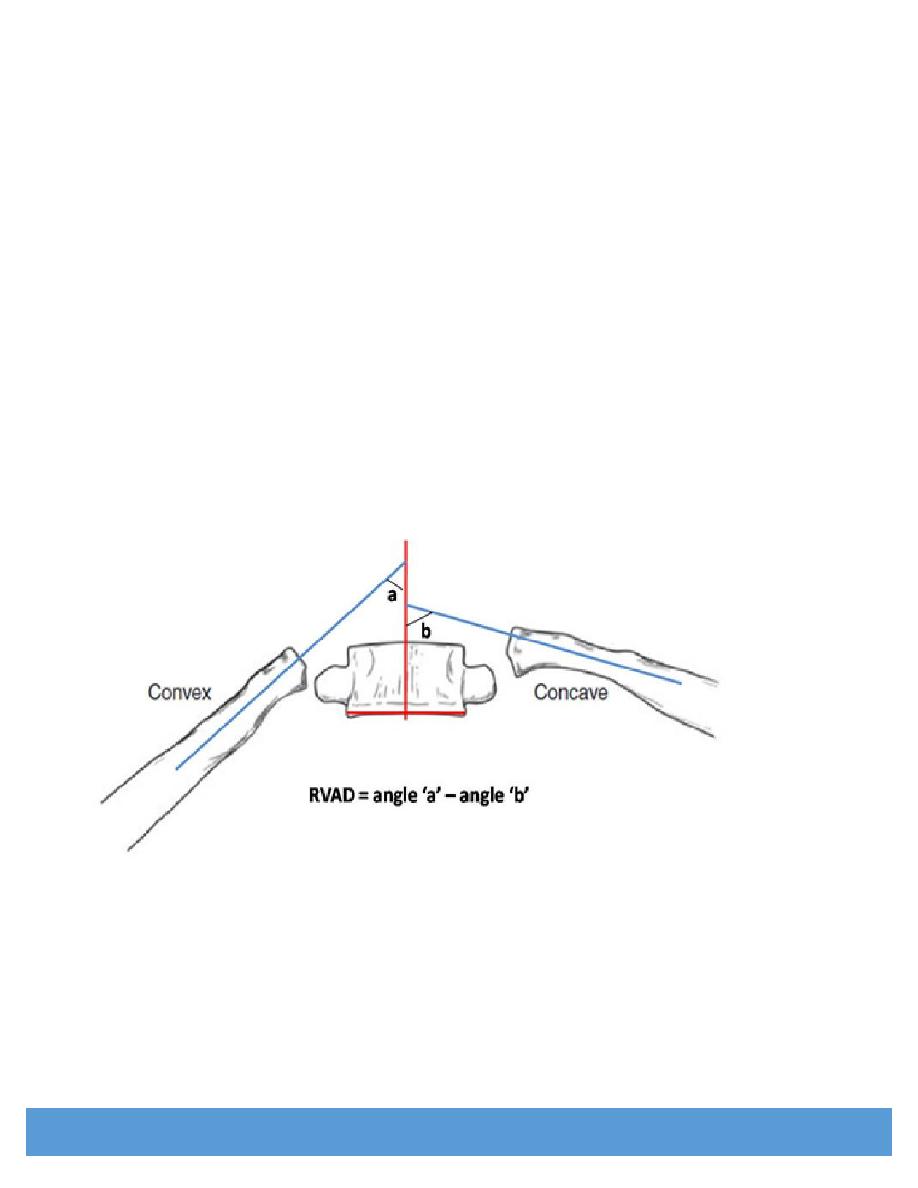
-although 90 % of infantile curves resolve spontaneously , progressive curves
can become very severe, especially those that have rib -vertebra angle
difference at the apex of the curve RVAD > 20 degrees
- there is high incidence of cardiopulmonary dysfunction.
- it is rare and boys are mainly affected
Curves that are progressive should be treated by applying serial Elongation -
Derotation - Flexion ( EDF) plaster casts under general anesthesia until the
the deformity resolves or until the child is big enough to use brace
If the deformity continues to deteriorate , surgical correction may be required.
surgery includes : anterior disc excision and fusion to control the apex of the curve ,
combined with posterior fusion to prevent posterior overgrowth.
8
2- Juvenile idiopathic scoliosis :
occurs at age of 4 to 9 years
-it is uncommon , its features are similar to those of adolescent group , but
the prognosis is worse and surgical correction may be necessary before
puberty , however , sometimes the brace can hold the curve until the age
of 10 years when fusion may be indicated.
3- Adolescent idiopathic scoliosis :( AIS )
it occurs at age of 10 years or over
- it is the commonest type of idiopathic scoliosis consists 90 % of cases
- it occurs mostly in girls
-Primary thoracic curves are usually convex to the right. ( right thoracic )
- Primary lumbar curves are usually to the left ( left lumbar )
- Thoracolumbar curves and double primary curves also occur

9
-Not all curves will progress , most curves less than 20 degrees resolve
spontaneously.
-However, once a curve starts to progress, it usually goes on doing so
throughout the remaining growth period ( and to a much lesser degree
beyond that ).
-
Predictors of progression are
:
1- Very young age
2-Marked curvature
3- Incomplete Rissers sign at presentation and girls who still not stating
menstrual cycle.
Treatment of AIS :
The aims of the treatment are :
1- Prevent a mild deformity from becoming severe
2- To correct an existing deformity that is unacceptable to the patient
Non-operative treatment :
indicated if ALL of the followings are there :
- if the patient is near skeletal maturity
-if the deformity is acceptable ( cobb s angle less than 30 degrees and
well balanced )
- if the sequential x ray shows NO definite rapid progression
Conservative treatment consists of Exercises and Bracing
Exercises
: have no effect on the curve but they do maintain the muscle tone
Bracing
: used for curves between 20 and 30 degrees
They should be worn
23
hours out of 24
The child can do daily activities including sports while wearing brace
These braces will NOT improve the curve but it may just stoping its progression.
Types of braces :
Milwaukee brace
: thoracic support
Boston brace
: lumbar or thoracolumbar support

10
Surgical treatment :
Indications
:
1-
For curves larger than 30 degrees that are cosmetically unacceptable,
especially in pre-pubertal children who are liable to develop severe
progression during growth spurt
2-
For milder deformity that has rapid progression
Note
: balanced double primary curves require operation only if they are
larger than 40 degrees and progressing
Aims of surgery are :
1-
To stop progression of the deformity
2-
To straighten the curve ( including the rotational component ) by some
form of instrumentation
3-
To arthrodese the entire primary curve by bone grafting
11
The surgery can be done by anterior , posterior or combined approach using
different instrumentation systems.
Complications of surgery :
1- Neurological compromise
2- Spinal decompensation : overcorrection may produce an unbalanced
spine
3- Pseudarthrosis
4- Implant failure
12
Congenital scoliosis : ( osteopathic )
Can be caused by :
1-
Failure of formation : hemivertebra , wedge vertebra
2-
Failure of segmentation : fused vertebrae
congenital scoliosis may be associated with other congenital malformations
like spina bifida, heart or kidney anomalies and diastematomyelia.
Treatment for progressing curves is usually surgery,no response to bracing
3-
Both types

13
Neuropathic and Myopathic scoliosis :
Neuromuscular conditions associated with scoliosis includes :
Poliomyelitis
Cerebral palsy
Syrinogmyelia
Friedreich s ataxia
The curve may take some
years
to develop.
The typical paralytic curve is
long
, convex towards the side with
weak
muscles and
at first is
mobile
Mild
curves need no treatment ,
severe
curves that associated with pelvic obliquity and
loss of sitting balance can often be managed by sitting support if no benefit then
surgical stabilization is done.
Scoliosis and Neurofibromatosis :
About one-third of patients with neurofibromatosis develop spinal deformity
Typically scoliosis is associated with skin lesions and the curve is sharp and short.
Kyphosis :
Excessive thoracic curvature may be better described as hyperkyphosis
Kyphosis can be :
1- Postural
: associated with flat feet , or can be secondary to other
deformities
2- Structural kyphosis
: is fixed and associated with changes in the shape
of the vertebrae
Structural kyphosis can be caused by
:
Congenital vertebral defects : failure of formation or
failure of segmentation or both
Skeletal dysplasia such as achondroplasia
Osteogenesis imperfecta
T.B of the spine
Scheuermann s disease in adolescents
Trauma in adults
Osteoporosis and compression vertebral fractures in elderly
Adolescent kyphosis : Scheuermann s disease
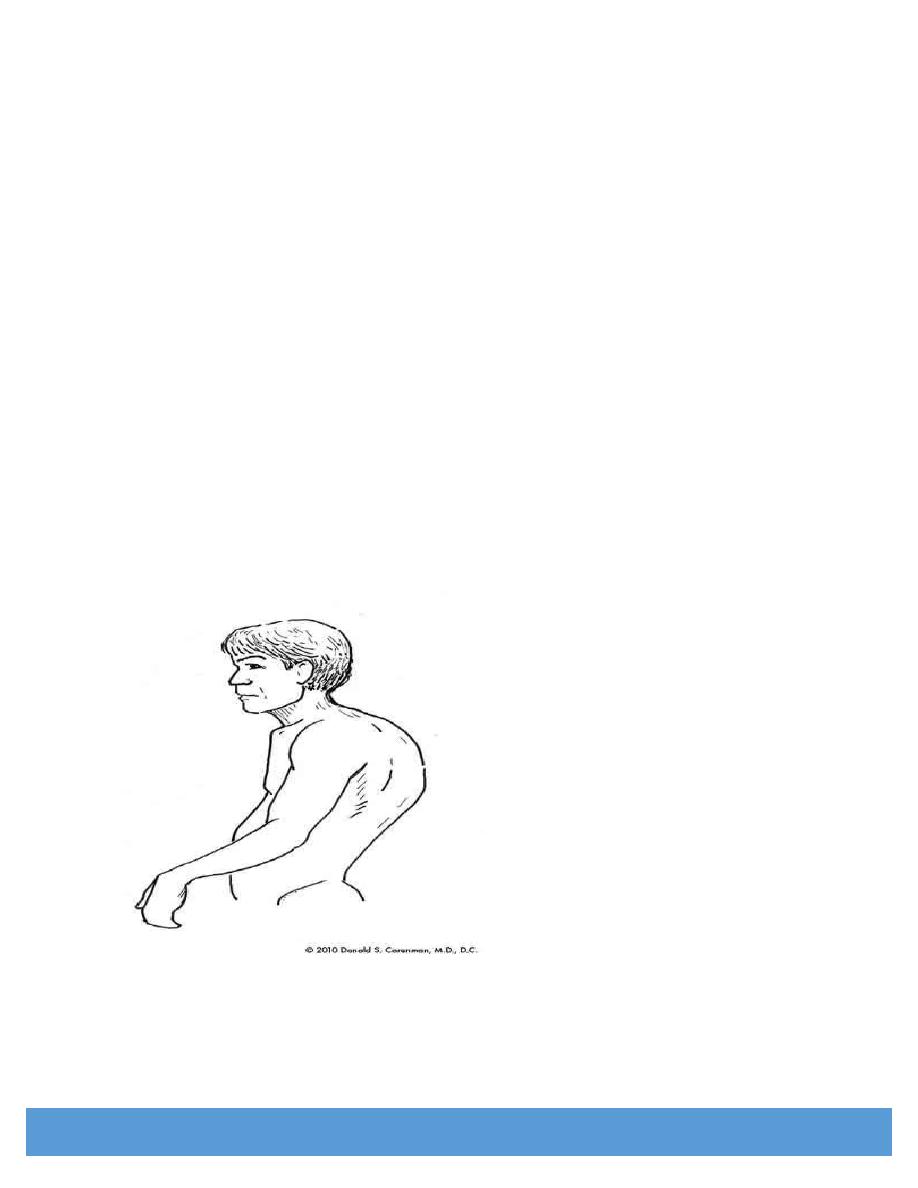
14
Scheuermann described this disease in 1920
The characteristic feature was a fixed round back deformity associated with wedging of several
thoracic vertebrae in adolescents.
It starts at puberty and affects boys more than girls
The patient may complain of back pain
This deformity sometimes increases after the end of the growth and becomes severe
X -Ray : Lateral view will show
irregular
and
fragmented
vertebral endplates
usually
T 6 - T10
The changes are more marked anteriorly
Wedging of more than 5 degrees in three adjacent vertebrae and an overall kyphosis angle
of more than 40 degrees are abnormal
Treatment
:
Curves less than 40 degrees only exercises and postural training
More severe curves may responds to brace treatment
Young adult with a rigid curve more than 60 degrees may need operative correction and fusion with fixation
15