2- Modified Thomas splint.
This splint has been widely used on small animals and can be used also onlarge animals. Its use is basically limited to restrict movement.
The common uses of modified Thomas splint :
For stable fracture.
As additional immobilization for internal fixation.
Immobilization following joint surgery, and treatment of joint.
Tendon and nerve injury.
The Thomas splint is adjustable and can be adapted to either fore-or hind
Limb. Rod
Duraluminum commonly used to construct the Thomas splint. It is light,
easily shaped, and sufficiently rigid to bear the animal weight.
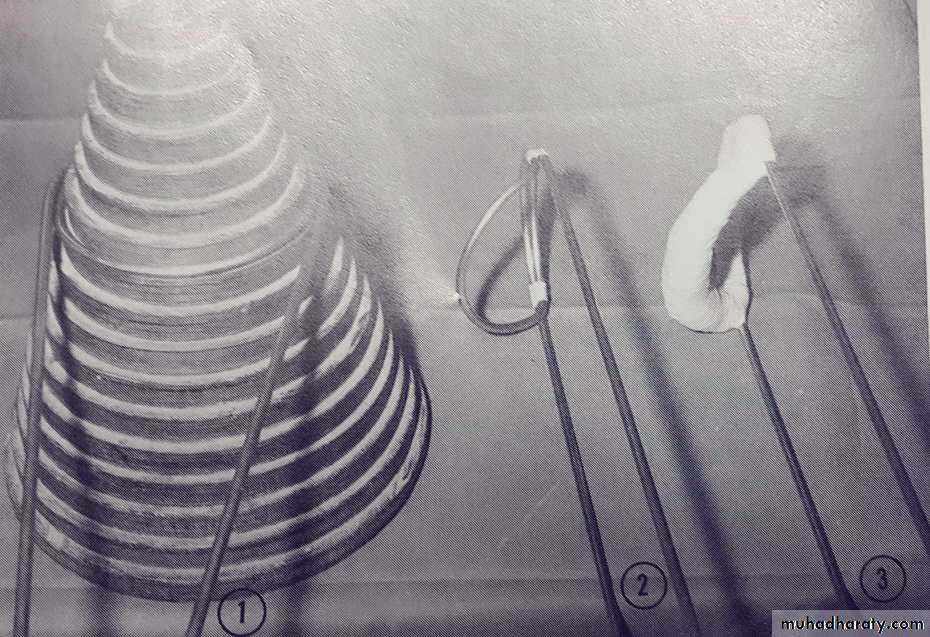
The mold used for construction of Thomas splint
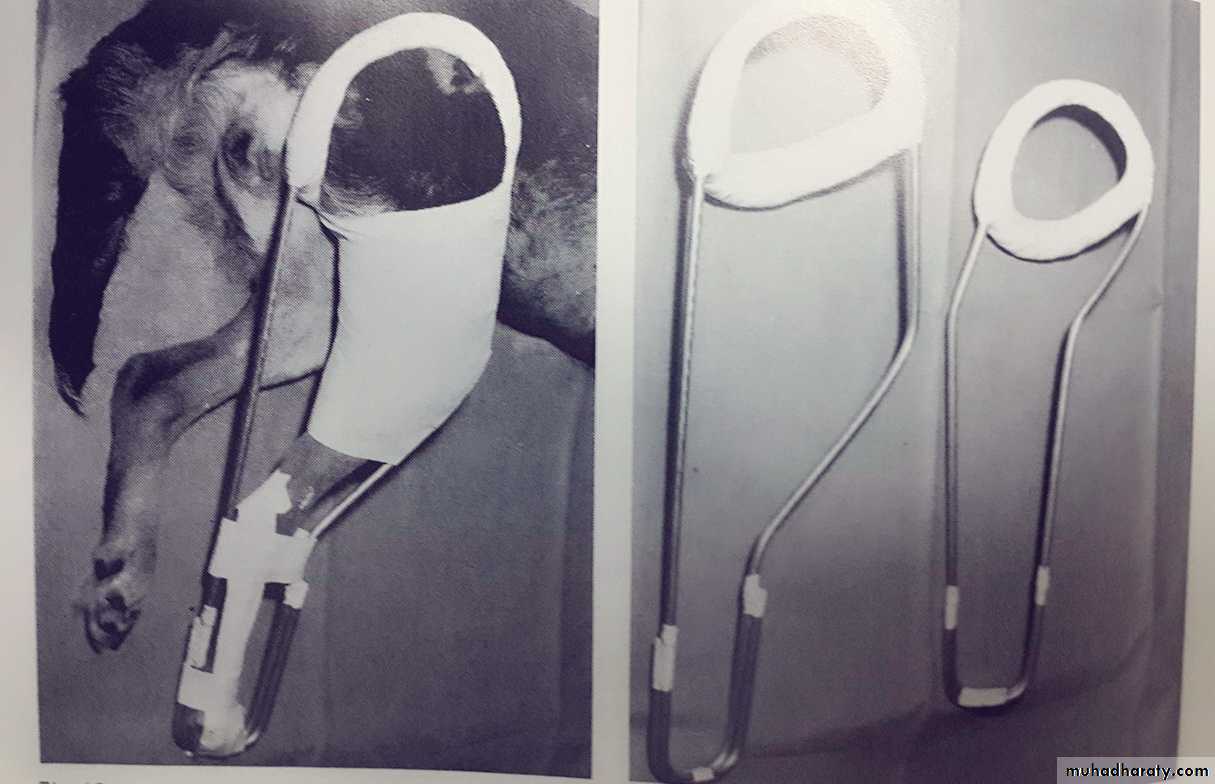
Thomas splint applied on hind limb
Hind limb Thomas splint (left)
Fore limb Thomas splint (right)
Internal fixation of fracture
Indications for uses internal fixation devices:If it is impossible to maintain an acceptable position by external splintage.
When external fixation is not tolerated by the animal.
When it is necessary to perform surgery to secure adequate reduction.
When it is the preferred method to secure rigid fixation and early ambulation.
The following devices are commonly used for internal fixation:
Kirschner SplintThis device involves inserting two pins or more in the proximal and distal bone segments. The pins are then connected by an external bars. The splint may be applied following open or closed reduction.
Characteristics of Kirschner splint.
It is adaptable to a wide variety of fractures, particularly those of long bones.
This technique is very suitable for compound fractures.
It is a very good technique for treatment of delayed or non union fractures.
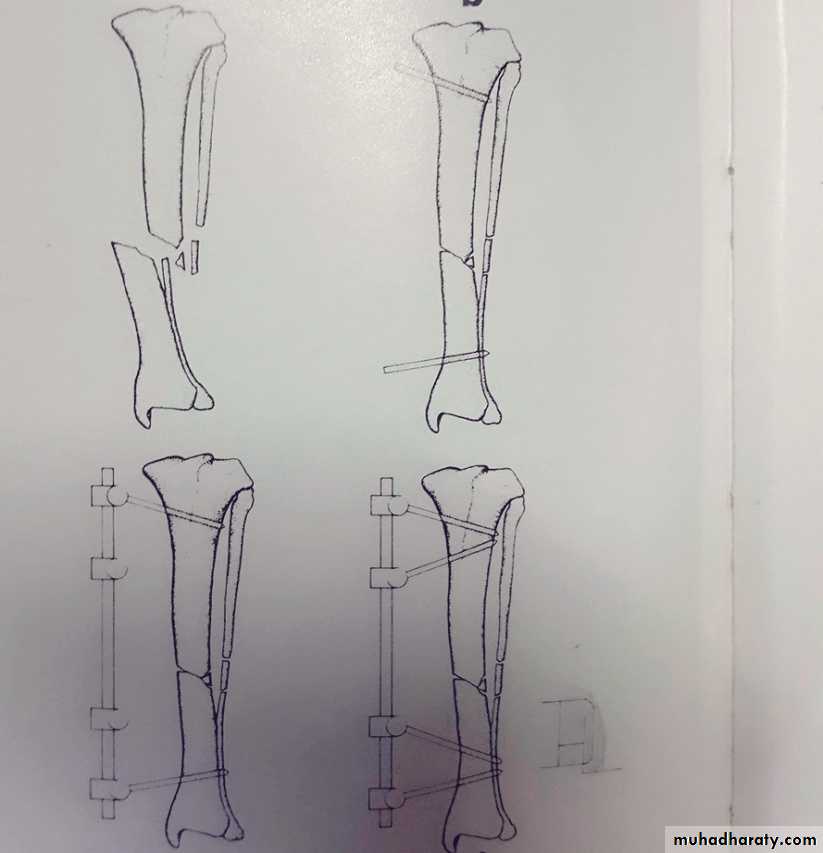
Application of Kirschner splint
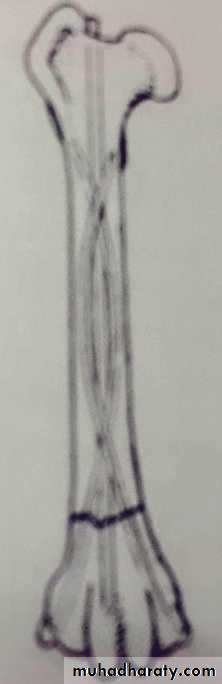
Intramedullary PinsThere are many types of pins available ( Steinmann, Kuntscher, Rush, Kirschner) are most commonly used. Intramedullary pins can be inserted by open or closed method.
Advantages of intramedullary pins:
Pins are readily available and easy to place and remove.
A single intarmedullary pin stabilizes the fractures against bending forces.
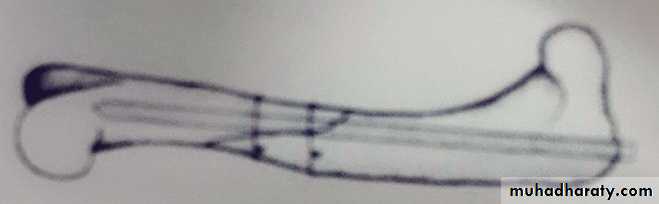
When three or more pins are used to fill the intramedullary cavity, the bone may also resist rotation forces.
Disadvantages of intramedullary pins:
Variation in bone size and shape often limits the ability of pins to provide fracture stability.
Pins protruding from bone (e.g. proximal femur) cause soft tissue irritation.
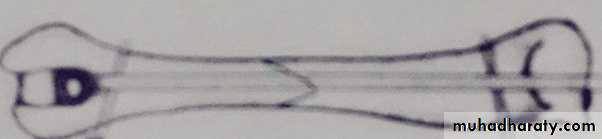
Intramedullary pin application
Multiple intramedullary pins application
Bone screws:There are 2 basic types of bone screws:
Cancellous bone screws are used to compress fragments of epiphyseal or metaphyseal bone and the thread of the screw does not cross the fracture line.
Cortical bone screws are used primarily in diaphysis.
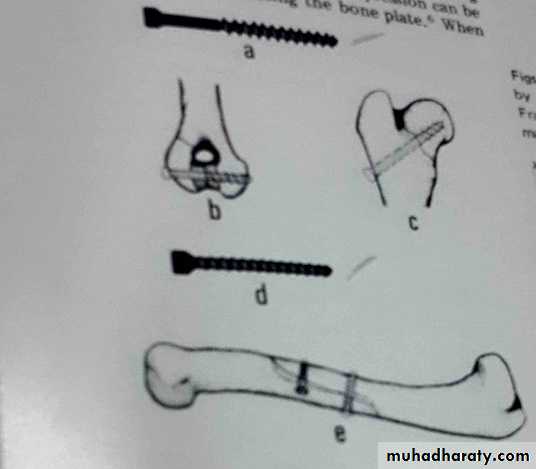
Cancelleous screw
Epiphyseal application of cancelleous screwMetaphyseal application of cancelleous screw
Cortical screw
Diaphyseal application of cortical scrwe
Bone plates:
A bone plate and screws are used to realign and stabilize bone fragments in a simple or comminuted long or flat bone fractures.
Advantages of bone plate:
Because bone plates can stabilize fractures by apposing (compressing) the bone, they provide a quick return of limb function.
Bone plating effectively counteracts all destructive fracture forces and screws are used to appose small bone fragments.
Disadvantages of bone plate:
Specialized training and equipment are required.
Extensive soft tissue dissection is necessary to permit plate application.
Second surgeries may be needed to remove broken plates, which can cause irritation, or excessively stiff plates, which can cause
thinning of the underlying bone.
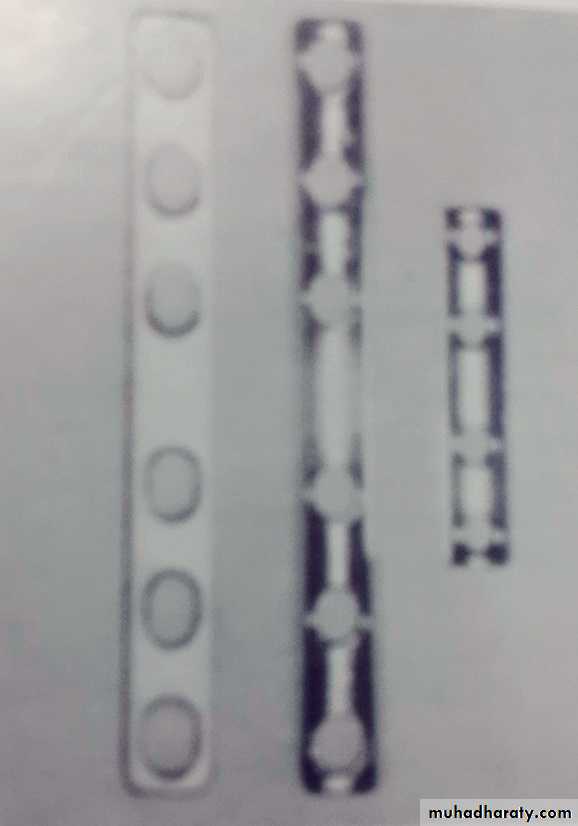
Different size of bone plate

Application of bone plate
Orthopedic wires :
Are used to encircle (cerclage) or penetrate (hemicirclage) the bone and provide fragmentary apposition. Wires are always used in conjunction with other implants (e.g. pins ,bone plates) .Advantages: Wires are affordable and easily applied.
Disadvantages: Wires require ancillary fixation to provide fracture stability against bending and compression forces.
Circalege wire application
Hemicirclage wire application
Delayed union and Nonunion of the fractureDelayed union: refers to a fracture that has not healed within the usual time. By radiograph it will give the following appearance:
The fracture line is evident.
Callous formation is minimal.
The fracture site has a feathery or wooly appearance.

Radiograph showing delayed union of radial and ulnar fractures
Nonunion: refers to a fracture in which all evidence of osteogenic activity at the fracture site has ceased, movement is present, and union is no longer possible without surgical intervention. The radiographic features of nonunion are:Rounding and increased density of the bones at the fracture site.
Sclerosis between the fracture segments wit well defined gap.
Bowing at the fracture site.
Closure of the medullary cavity.
Demineralization of the bone above and below the fracture line.

Radiograph showing nonunion of a femoral fracture
The fractures most likely to result in delayed union and nonunion are:Transverse or short oblique fractures of radius and ulna.
Fractures of the femoral neck.
Fractures of distal 1/3 of the tibia.
Transverse mid shaft fractures.
The most common causes of delayed or nonunion are:
Inadequate immobilization or failure to maintain it.Inadequate reduction.
Impairment of blood supply as a result of the original trauma or damage occurs during surgery.
Infection and loss of bone from open fracture.
Treatment of delayed union:
If reduction is satisfactory, rigid fixation should be applied for extended period.If there is good bone contact with malalignment or bending at the fracture site, the bone should be straightened and rigid fixation is applied.
If reduction is unsatisfactory, surgical intervention should be applied.
Treatment of nonunion:
Rigid stabilization using a compression plate or external skeletal fixation to convert the fibrous union to osseous consolidation.Cancellous bone grafting.
Rechannelization of the medullary canal to promote osteosynthesis.