Fifth stage
PediatricLec-1
د.خليل
19/10/2016
The cardiovascular systemCongenital Heart Disease
Epidemiology:Heart disease in children is mostly congenital.
8 per 1000 live-born infants have significant cardiac malformations
About 10% of stillborn infants have a cardiac anomaly.
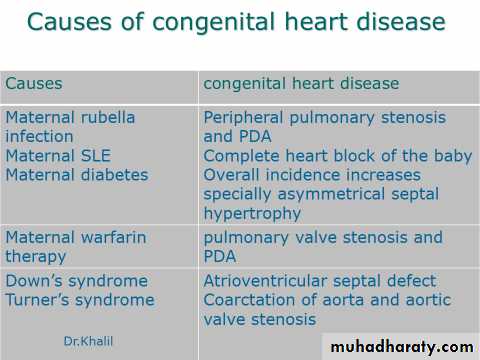
Etiology of congenital heart disease
Little is known about the etiology C.H.D.A small proportion are related to external teratogens
About 8% are associated with major chromosomal abnormalities.
Polygenic abnormalities probably explain why a previous child with congenital heart disease doubles the risk for subsequent children and the risk is still higher if either parent has congenital heart disease.
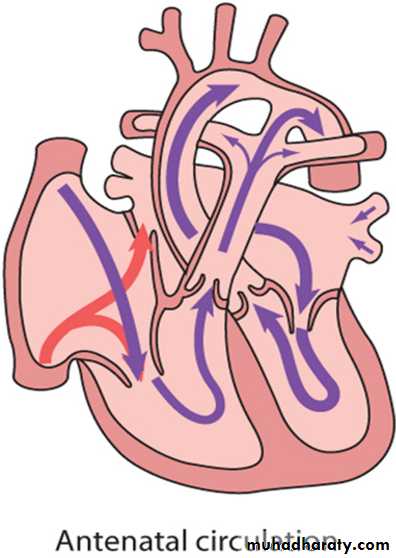
Circulatory changes at birth
In the fetus, the left atrial pressure is low, as relatively little blood returns from the lungs.The pressure in the right atrium is higher than in the left, as it receives all the systemic venous return including blood from the placenta.
The ductus arteriosus shifts the blood from the pulmonary artery to the aorta.
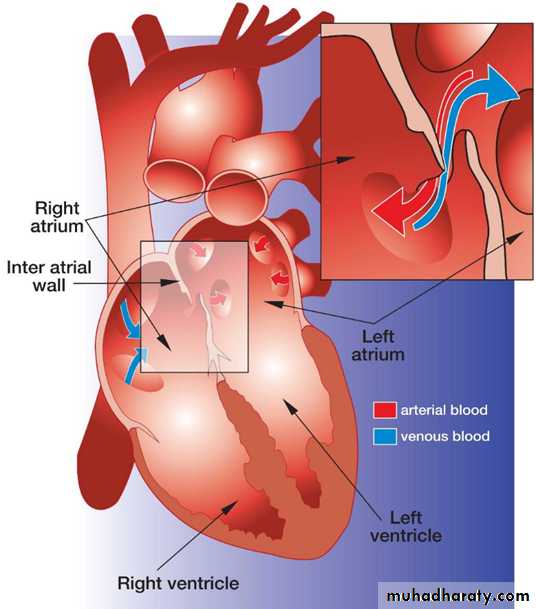
The flap valve of the foramen ovale is held open, blood flows across the atrial septum into the left atrium and then into the left ventricle, which in turn pumps it to the upper body.
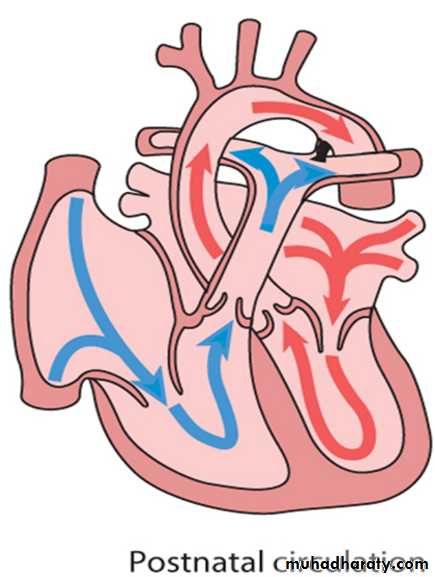
With the first breaths, resistance to pulmonary blood flow falls and the volume of blood flowing through the lungs increases sixfold. This results in a rise in the left atrial pressure. Meanwhile, the volume of blood returning to the right atrium falls as the placenta is excluded from the circulation. The change in the pressure difference causes the flap valve of the foramen ovale to be closed. The ductus arteriosus will normally close within the first few hours or days.
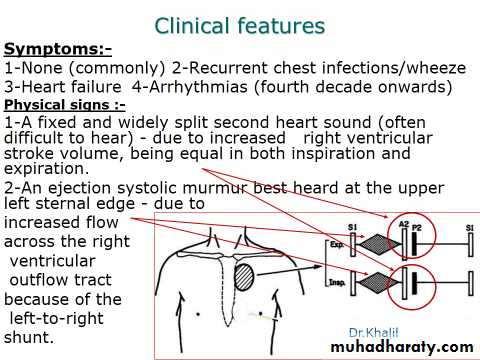
Presentation:
Congenital heart disease could present in any way of the followings:Antenatal cardiac ultrasound diagnosis
Detection of a heart murmur
Cyanosis
Shock.
Heart failure
Antenatal diagnosis

Fetal anomaly scan is performed between 18 and 20 weeks' gestation. If an abnormality is detected, detailed fetal echocardiography is performed by a paediatric cardiologist, who also checks any fetus at increased risk, e.g. where Down's syndrome is suspected, where the parents have had a previous child with heart disease or where the mother has C.H.D. The continuation of pregnancy and delivery then planned.

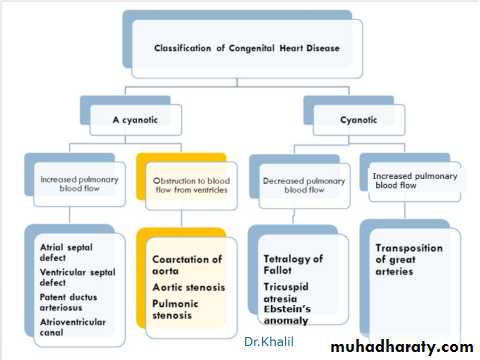
Obstructive (stenotic lesions)
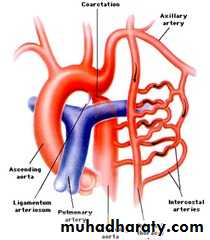
Coarctation of aortaIt is constrictions of the aorta just below the origin of the left subclavian artery at the origin of the ductus arteriosus.
Etiology and Epidemiology
During development of the aortic arch, the area near the insertion of the
ductus arteriosus fails to develop correctly,resulting in a narrowing of
the aortic lumen. This leasion forms 5-10% of all congenital heart defects.
Clinical Manifestations
The more the severe the narrowing the earlier the presentation.
Infants present with poor feeding, respiratory distress,and shock and may have hypoplastic aortic arch with VSD.
Older children re usually asymptomatic or presenting With leg discomfort with exercise, headache, or epistaxis.
On examination
A-Decreased or absent lower extremity pulsesB-Upper extremity hypertension.
C-Murmur may be present which is systolic and best heard in the left interscapular area of the back. If significant collaterals have developed, continuous murmurs may be heard throughout the chest.
Investigations
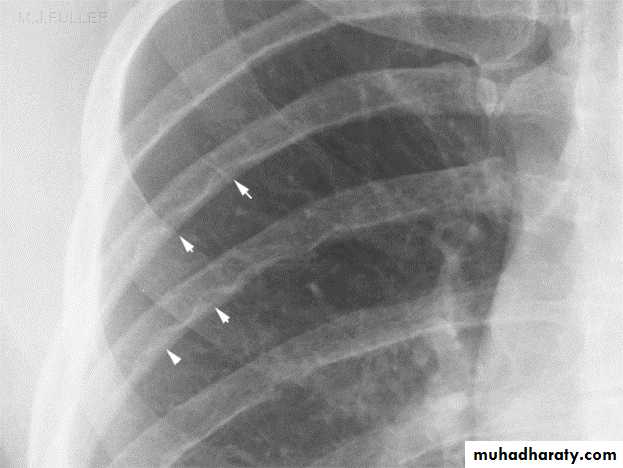
In infantile type ECG and CXR show right ventricular hypertrophy with cardiomegaly and pulmonary edema while in older children they show left ventricular hypertrophy and a mildly enlarged heartIn older children(>8 years) the chest x-ray film may show notching
of the ribs due to the development of collaterals.
2-
Echocardiography shows the site and degree of coarctation, presence of left ventricular hypertrophy, and aortic valve morphology and function

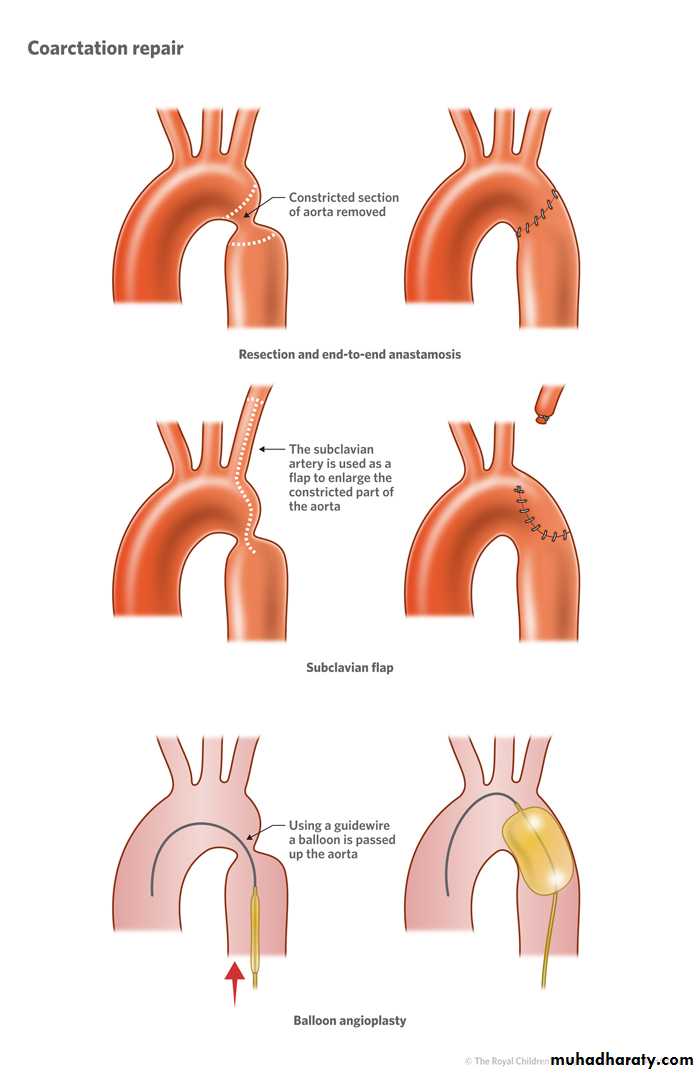
Treatment
In infants management of heart failure and PGE2 infusion to maintain ductus patency then balloon dilatation or surgical repair.
In older children balloon dilatation and stenting or surgical repair.
Acyanotic Congenital Heart Disease with increased pulmonary blood flow
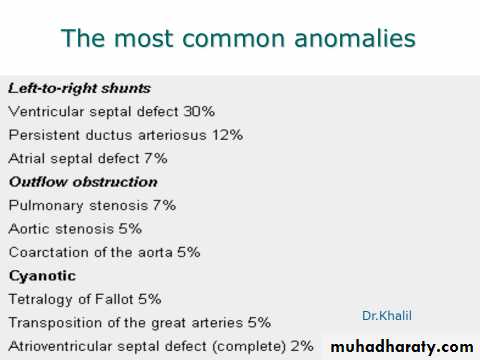
(Left-to-right shunts)Atrial Septal Defect
PREVALENCE
ASD (ostium secundum defect) occurs as an isolated anomaly in 5 % to 10% of all congenital heart defects.
It is more common in females than in males (male/female ratio of 1:2).
PATHOLOGY ;
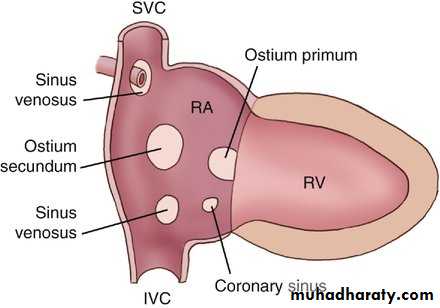
1- Ostium secundum defect is the most common type of ASD, accounting for 50% to 70% of all ASDs. This defect is present at the site of fossa ovalis, allowing left-to-right shunting of blood from the left atrium to the right atrium
2- Ostium primum defects occur in about 15-30% of all ASDs.
3- Sinus venosus defect occurs in about 10% of all ASDs.
The defect is most commonly located at the entry of the superior vena cava (SVC) into the RA (superior vena caval type) and rarely at the entry of the inferior vena cava (IVC) into the RA (inferior vena caval type).

1-E.C.G
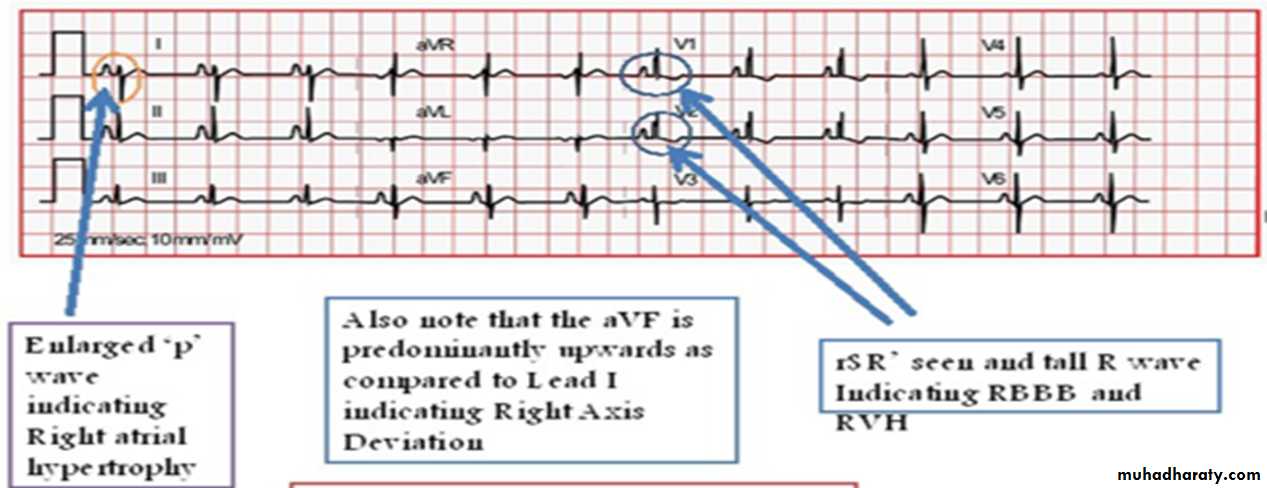
Right axis deviation of +90 to +180 degrees and mild right ventricular hypertrophy (RVH) or right bundle branch block (RBBB) with an rsR' pattern in V1 are typical findings
2-X-ray Studies
Cardiomegaly with enlargement of the RA and right ventricle (RV) may be present.
A prominent pulmonary artery (PA) segment and increased pulmonary vascular markings are seen when the shunt is significant


3-Echocardiography
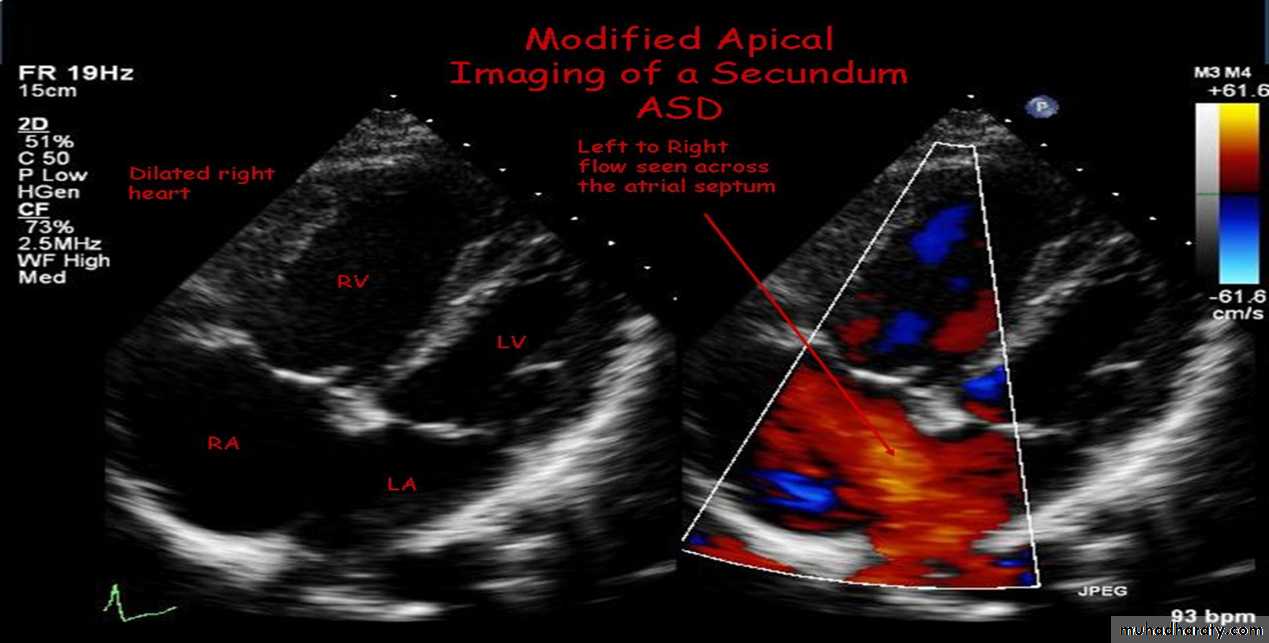
The location and size of the atrial defect are readily appreciated by two-dimensional scanning . The shunt is confirmed by pulsed and color flow Doppler .
NATURAL HISTORY :
With ASD less than 3 mm in size diagnosed before 3 months of age, spontaneous closure occurs in 100% of patients at 1½ years of age. Spontaneous closure occurs in more than 80% of the time in patients with defects between 3 and 8 mm before 1½ years of age. An ASD with a diameter greater than 8 mm rarely closes spontaneously.Most children with an ASD remain active and asymptomatic. Rarely, congestive heart failure (CHF) can develop in infancy
If a large defect is untreated, CHF and pulmonary hypertension develop in adults who are in their 20s and 30s.
With or without surgery, atrial arrhythmias (flutter or fibrillation) may occur in adults.
Infective endocarditis does not occur in patients with isolated ASDs.
Cerebrovascular accident, resulting from paradoxical embolization through an ASD, is a rare complication.
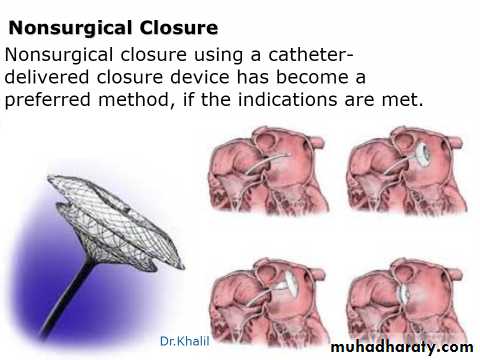
MANAGEMENT:
Medical
Exercise restriction is unnecessary.
Prophylaxis for infective endocarditis is not indicated unless the patient has mitral valve prolapse or primum ASD.
In infants with CHF, medical management is recommended because of its high success rate and the possibility of spontaneous closure of the defect.
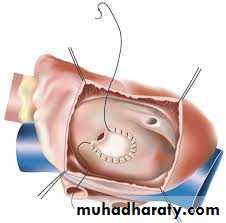
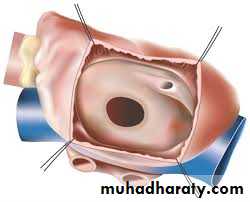
Surgical Closure.
It is done if device closure is not appropriate.