1
Fifth stage
Pediatrics
Lec-
Dr.Athl
10/11/2016
Prematurity
Premature (preterm) baby:
• Birth before 37 completed weeks gestation.
• 8% of all births.
• Most problems seen with infants born <32 completed weeks.
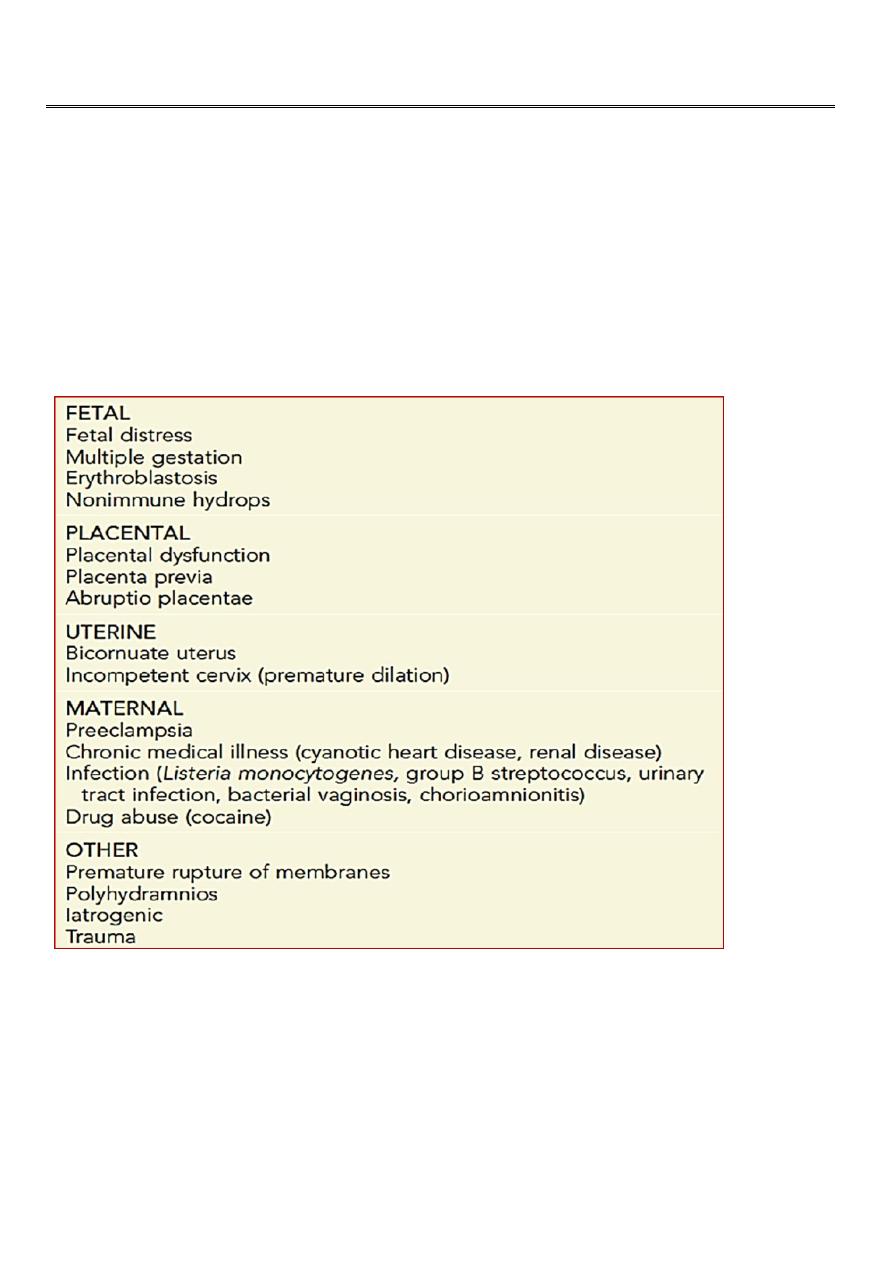
Predisposing Factors :
2
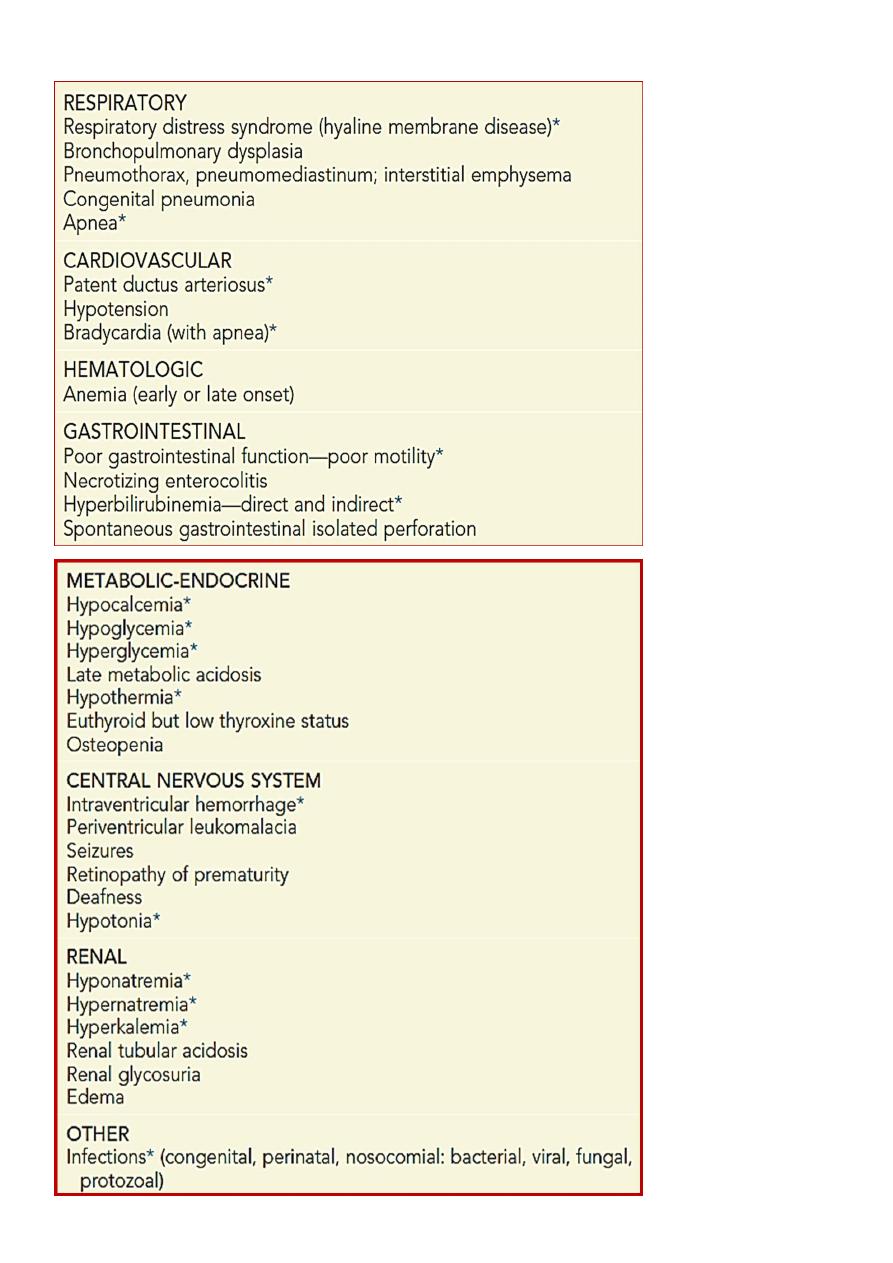
Complications Of Prematurity:

3
Signs Of Prematurity :
1. Thin gelatinous
and dark red in color.
skin
2. Poorly developed
tissue, no palpable breast tissue or it is flat and less than
breast
1cm in diameter.
3. The
is soft, no cartilage and there is slow or no recoil.
ear auricle
4.
Genitalia:
• Male: the testes are not descended in the scrotum and no creases on the
scrotum.
• Female: labia majora are not covering completely labia minora.
5.
are absent or only seen on the anterior 2/3 of the sole
Plantar creases
4
Low birth weight (LBW) and Intrauterine Growth Restriction (IUGR) :
Low birth weight (LBW) infants, defined as infants having birth weights of less than 2500 g,
represent a large component of the neonatal and infant mortality rates.
IUGR is the most common cause of LBW in developing countries, whereas prematurity is the
cause in developed countries.
Very low birth weight (VLBW) infants, weighing less than 1500 g at birth, represent about
1% of all births but account for 50% of neonatal deaths.
IUGR is present when fetal growth stops and, over time, declines to less than the 5th
percentile of growth for gestational age or when growth proceeds slowly, but absolute size
remains less than the 5
th
percentile.
Maternal factors associated with a LBW caused by premature birth or IUGR include:
• Previous LBW birth
• Low socioeconomic status
• Low level of maternal education
• No antenatal care
• Maternal age younger than 16 years or older than 35 years
• Short interval between pregnancies
• Cigarette smoking, alcohol and illicit drug use
• Physical (excessive standing or walking) or psychological (poor social support)
• Stresses, unmarried status, low pre-pregnancy weight (<45kg), poor weight gain
during pregnancy (<10 lb), and African American race.
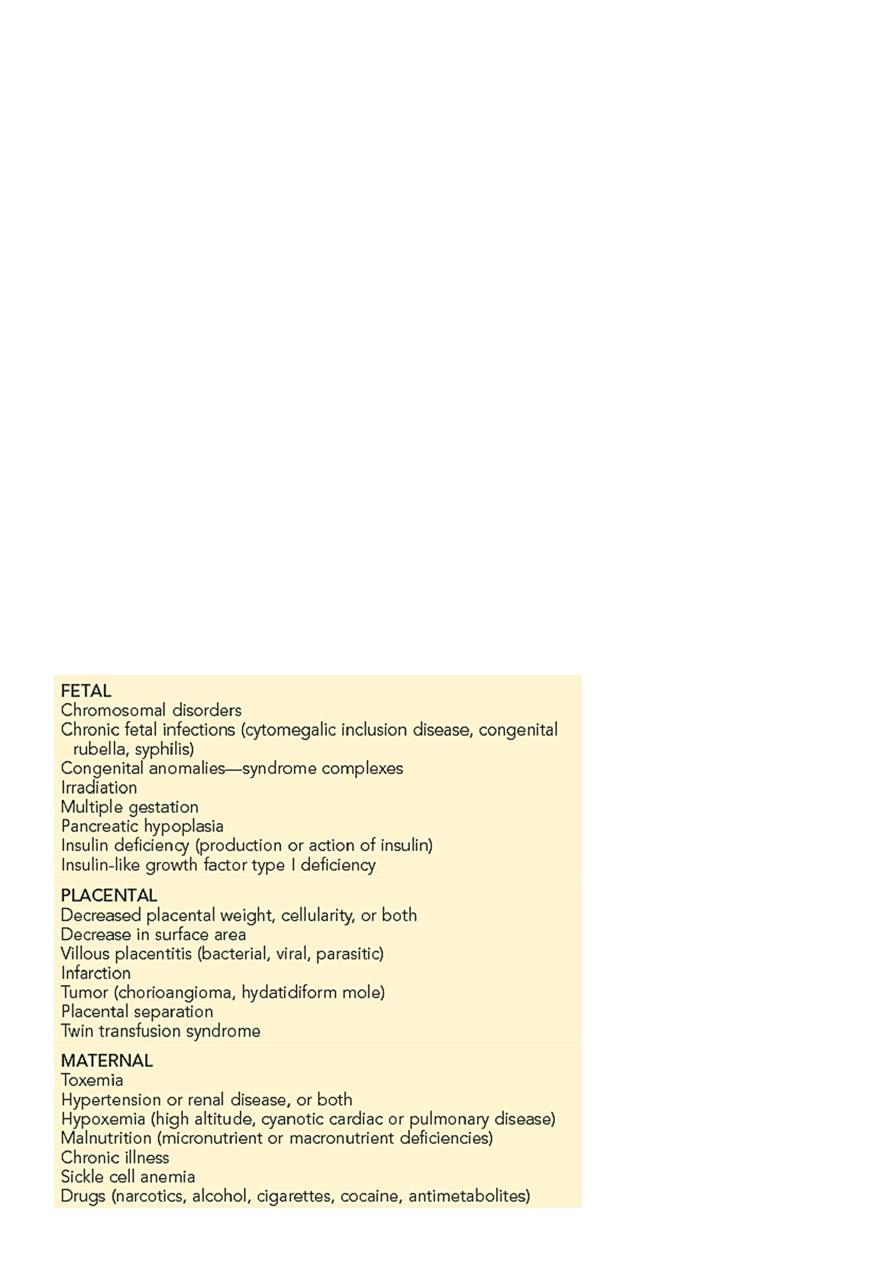
Factors Often Associated with Intrauterine Growth Restriction :
5
:
Problems of IUGR and SGA
1) Intrauterine fetal demise
2) Temperature instability
3) Perinatal asphyxia
4) Hypoglycemia
5) Polycythemia -hyperviscosity
6) Reduced oxygen consumption/ hypothermia
7) Dysmorphology
8)Pulmonary hemorrhage
Symmetric IUGR ((head circumference, length, and weight equally affected) often has an
earlier onset and is associated with diseases that seriously affect fetal cell number, such as
conditions with chromosomal, genetic, malformation, teratogenic, infectious, or severe
maternal hypertensive etiologies.
Asymmetric IUGR (with relative sparing of head growth) is often of late onset, and is
associated with poor maternal nutrition or with late onset or exacerbation of maternal
vascular disease (preeclampsia, chronic hypertension).
NURSERY CARE:
At birth, the measures needed to clear the airway, initiate breathing, care for the umbilical
cord and eyes, and administer vitamin K are the same for immature infants as for those of
normal weight and maturity. Special care is required to maintain a patent airway.
Additional considerations are the need for
1. thermal control and monitoring of the heart rate and respiration.
2. Oxygen therapy
3. Special attention to the details of fluid requirements and nutrition.
4. Safeguards against infection.
5. Routine procedures that disturb these infants may result in hypoxia.
6. The need for regular and active participation by the parents in the infant’s care in the
nursery, the need to instruct the mother in at-home care of her infant, and the
question of prognosis for later growth and development require special
consideration.
Large for Gestational Age Infants :
Infants with birth weight > the 90th percentile for gestational age are called large for
gestational age (LGA). Neonatal mortality rates decrease with increasing birth weight until
approximately 4,000 g, after which they increase. Maternal diabetes and obesity are
predisposing factors.

6
LGA infants, regardless of their gestational age, have a higher incidence of:
•
, such as cervical and brachial plexus injuries, phrenic nerve damage
Birth injuries
with paralysis of the diaphragm, fractured clavicles, cephalohematomas,
subdural hematomas, and ecchymoses of the head and face.
•
Hypoglycemia.
•
Polycythemia.
•
, particularly CHD.
Congenital anomalies
•
Intellectual and developmental retardation.