OBSTETRIC ULTRASOUND
Introduction:
•
Ultrasound in obstetrics can provide good information about the fetus and its
environment.
•
With ultrasound, an early intervention or conservative management in pregnancy
can be made.
•
Latest developments in ultrasound examination is a transvaginal ultrasound
discovery - the observation of "FLOW DOPLLER" and the most sophisticated
ultrasound 3D and 4D which has a high ability to determine fetal condition.
Clinical Consideration:
How safe is ultrasonography for the fetus?
•
Safe but, cannot be completely innocuous.
•
When there is a valid medical indication, the lowest possible ultrasonic exposure
setting, casual use should be avoided.
•
Physical effect:
-
Mechanical vibration.
-
Increased tissue temperature
Should all patients be offered ultrasonography?
•
For example, 90% of fetal anomaly are born to no risk mother.
•
Detection rate 16~85%.
•
Not obligated to perform ultrasonography in low risk or no indication.
Ultrasound Technology:
•
Intermittent high-frequency sound waves are generated by applying an alternating
current to a transducer made of piezoelectric material.
•
The transducer is “connected” to the abdominal or vaginal wall by placing a
coupling agent to diminished the loss of ultrasound wave
•
A pulse sound waves passes through soft tissues until an interface between the
structures of different tissues densities is reached
•
Some of the energy is reflected or echoed back to the transducer and amplified
and displayed on a screen
•
With real-time ultrasonography , the movement including breathing, cardiac actions
and vessel pulsations can be detected
Patient Preparation:
•
Prerequisite for an abdominal ultrasound examination is a full bladder for three
important reasons:
-
Full bladder pushes the uterus out of the pelvis → removing it from acoustic
shadow of symphysis pubis.
-
Full bladder provides an acoustic windows → pelvic organs can be visualized.
-
Displacement of bowel superiorly → preventing the gas from scattering the
ultrasound beam.
•
For a vaginal ultrasound, the bladder must be empty → small amount of urine can
pushed uterus posteriorly out of the field of view of the transducer.
Clinical Applications:
•
Very early identification of intrauterine pregnancy
•
Demonstration of the size and the rate of growth of the amnionic sac and the
embryo and, at times, resorbtion or expulsion of the embryo
•
Identification of multiple fetuses including conjoined twins
•
Measurements of the fetal head, abdominal circumference, femur and other
anatomical landmarks to help identifying the duration of gestation and identifying
growth retarded fetus
•
Identifying hydrocephaly – microcephaly , or anencephaly → comparison of the
fetal head and chest or abdominal circumference
•
Detection of fetal anomalies:
-
Distension of fetal bladder
-
Ascites
-
Polycyctic kidney
-
Renal Agenesis
-
Ovarian cyst
-
Intestinal obstruction
-
Diaphragmatic hernia
-
Meningomyelocele
-
Intracranial, cardiac or limb defect
-
Demonstration of hydramnion or oligohydramnion
-
Identification of the location and size of the placenta
•
Demonstration of placental abnormalities :
-
Hydatidiform mole
-
Molar degeneration
-
Chorioangioma
•
Identification of uterine tumors or anomalous development
•
Detection of foreign body → IUD, blood clot or retained placental fragments
Obstetric Sonography (1st trimester):
•
Establishment of an intrauterine pregnancy
•
Identification of the number of gestation
•
Detection of embryonic and fetal viability
•
Evaluation of complicated early pregnancy :
-
Retrochorionic hemorrhage
-
Anembryonic pregnancy
-
Incomplete or complete abortion
-
Molar pregnancy
•
Early dating of the pregnancy :
-
Gestational sac diameter
-
Crown-rump length
-
Biparietal diameter
•
Evaluation of the uterus and adnexae
•
Transabdominal ultrasound: Gestational sac usually established by:
-
5 weeks of amenorrhea
-
HCG 1800 – 3600 mIU / ml
•
Transvaginal ultrasound: Gestational sac usually established by:
-
4 weeks of amenorhea
-
Serum level of HCG 800 mIU/ml
•
Absence of an intrauterine gestational sac in conjuction with HCG value → ectopic
pregnancy ??
•
Using the M-mode, fetal heart motion can usually established by 7 weeks of gestation
•
Early dating of pregnancy:
-
4 – 6 weeks : use of GS diameter
-
8 – 10 weeks : use of CRL (most acurate dating of early pregnancy)
-
10 – 12 weeks : use of BPD
Nuchal Translucency:
•
The maximum thickness of the subcutaneus translucent area between the skin and
the soft tissues overlying the posterior aspect of the cervical spine in sagital scan
plane.
•
A thickness > 3 mm ( sagital plane ) :
-
90% trisomy 18 and 13
-
80% trisomy 21
-
5% normal.
•
This is a view (picture in the power point) obtained through the lower portion of the
fetal head. The skull is represented by a thick white line which surrounds the
developing brain. The yellow square illustrates the area in the fetal head where the
nuchal skin fold is identified. The nuchal skin fold is the thickness of the skin in the
neck region. If the thickness is increased, it could indicate a high-risk for Down
syndrome, or other chromosomal abnormalities. The inset illustrates the location of
the nuchal skin fold.
Uterus and Adnexia:
•
Cervical incompetence:
-
Funeling of the internal os ( dilatation )
-
Cervical length < 3 cm
-
Bulging membranes ( with or without prolaps of the cord or fetal parts )
•
Adnexial mass:
-
Physiological: Diameter corpus luteum at pregnancy about 2 cm
•
30 weeks of gestational age: length of cervix more than 3 cm
Obstetric Sonography (2nd & 3rd trimester):
•
Fetal viability, number and presentation.
•
Amount of amniotic fluid.
•
Placental localization.
•
Establishment of fetal age and growth by fetal biometry including:
-
BPD ~ biparietal diameter
-
FL ~ femur length
-
AC ~ Abdominal circumference
•
Evaluation of fetal anatomic structures:
-
Cerebral lateral ventricles
-
Spine
-
Four chamber view of the heart
-
Stomach-bowel,abdominal wall at the area of the umbilical cord insertion
-
Bladder and kidney
-
Limbs and umbilical cord.
•
Evaluation of the cervix and adnexae.
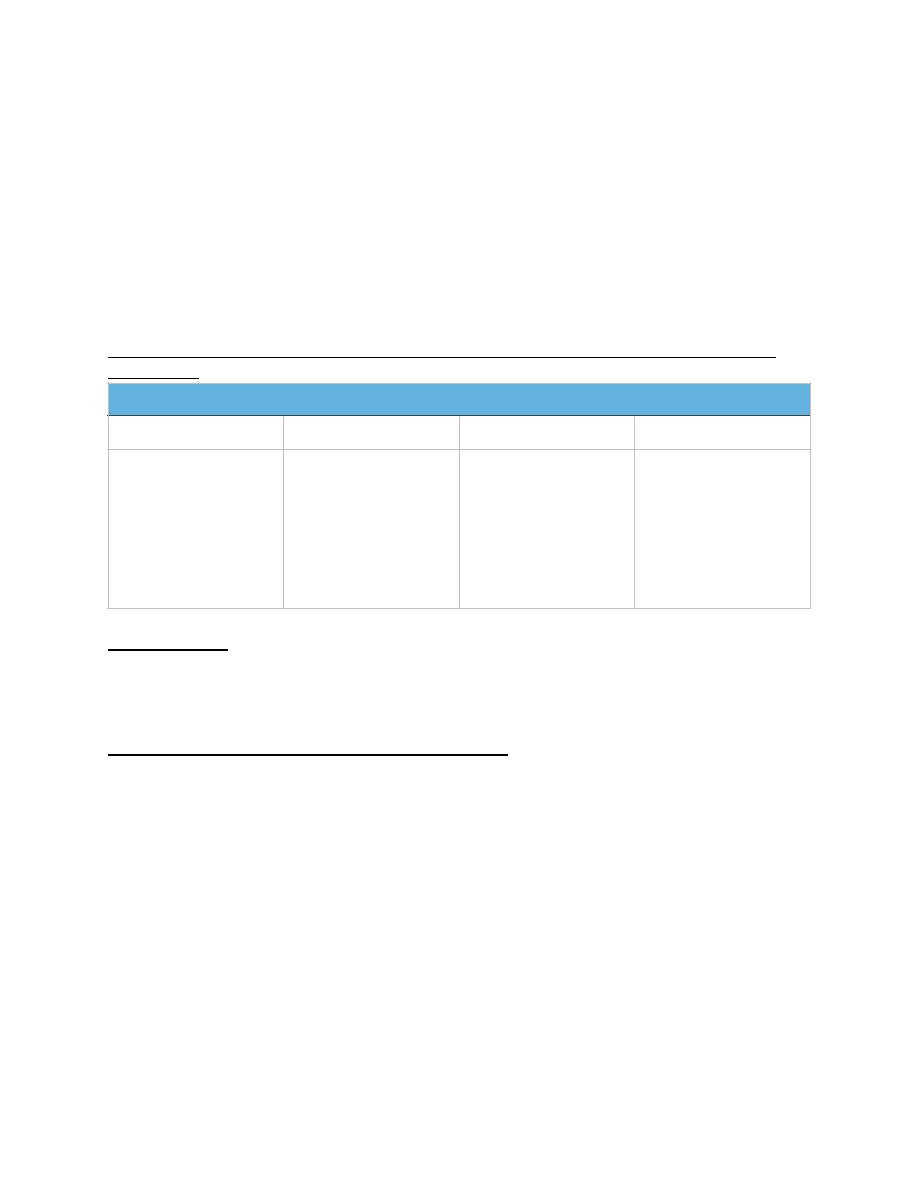
Preferred fetal dimension for estimation of gestational age at various stage of
pregnancy
Fetal viability:
1. Fetal cardiac activity
2. Fetal movement
3. Breathing movement
Sonographic assessment of the amniotic fluid:
•
Normal : at 2nd and 3rd trimester vertical pocket about 2 cm
•
AFI ( amniotic fluid index ) : sum of the depth of the largest pocket of fluid in the
four quadrants of abdomen
•
AFI < 5 cm : strongly asociated with oligohidramnions postmaturity
•
BPD, FL and AC the most important parameters for determination of gestational
age
•
Determination of gestational age should be performed prior to 26 weeks gestational
age
•
3rd trimester determination of gestational age does not accurately reflect
gestational age
•
BPD at a standard reference level measurement. When the shape is not oval the
BPD measurement is not accurate
Week’s Gestation
7 – 10
10 - 14
15 - 28
29
Crown-rump length
Crown-rump length
Biparietal Diameter
Femur Length
Humerus Length
Biparietal Diameter
Femur Length
Humerus Length
Head
Circumference
Binocular distance
Femur Length
Humerus Length
Binocular distance
Biparietal Diameter
Other long bones
Head
Circumference
Doppler in obstetric ultrasound:
Basic principles:
•
The volume flow in the Uas increases with advancing gestation. The high vascular
impedance detected in the first trimester gradually decreases. It is attributed to
growth of placental unit and increase in the number of the functioning vascular
channels.
Uses of Doppler:
1. Plays a vital role in the diagnosis of fetal cardiac defects.
2. Assessment of the hemodynamic responses to fetal hypoxia and anemia.
3. Diagnosis of other non-cardiac malformations.
UMBILICAL ARTERY FLOW:
•
Characteristic saw-tooth appearance of arterial flow in one direction and
continuous umbilical venous blood flow in the other.