
1
Medicine
Endocrine
http://goo.gl/rjRf4F
I
LOKA
©
http://www.muhadharaty.com/medicine-endocrine
I

2
Content
Topics:
Page:
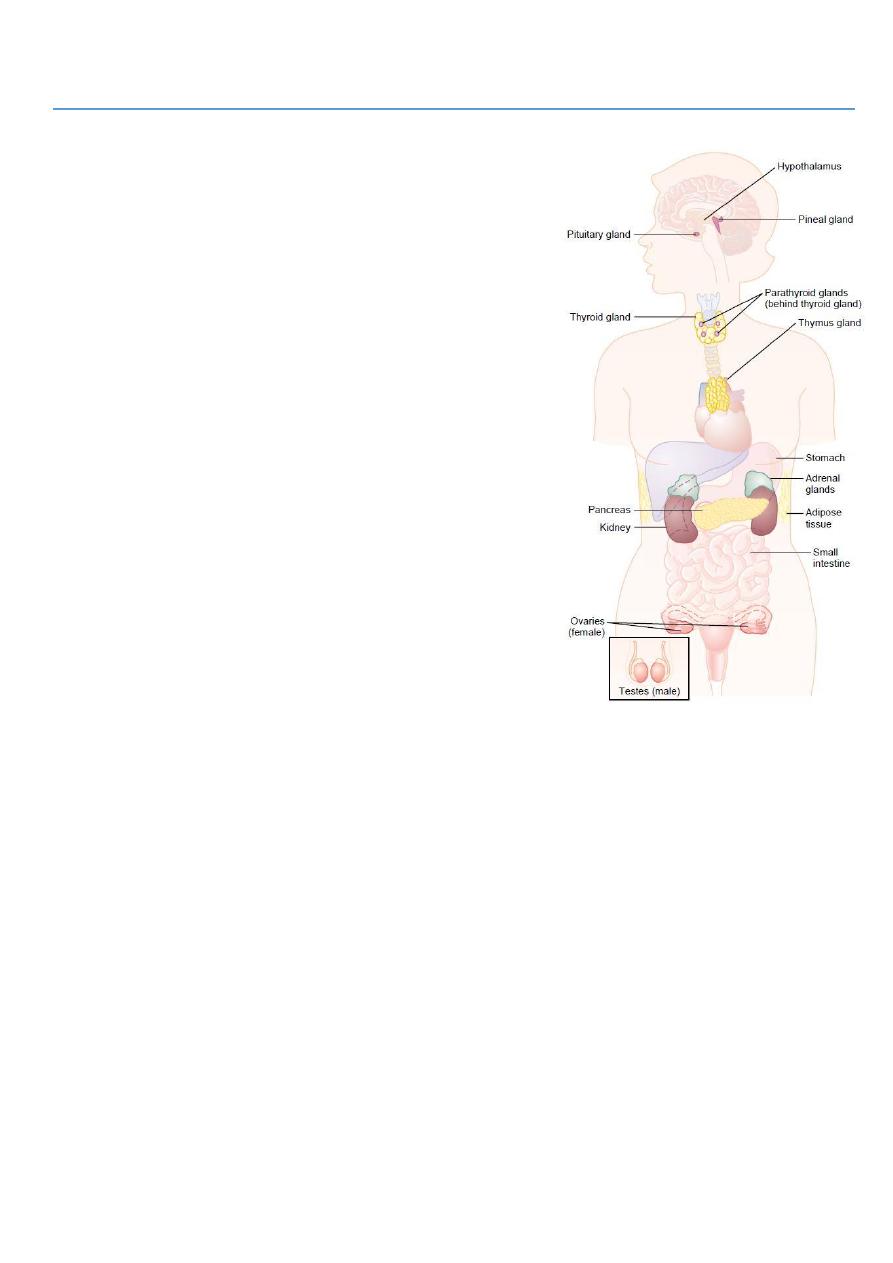
General endocrine
3
Thyroid gland
7
Parathyroid gland
11
Pancreas
13
Pituitary and adrenals
15
3
Part1:
General endocrine
#Types of diseases of endocrine glands:
Increase secretion of hormones or increase
peripheral sensitivity to hormones.
Decrease secretion of hormones or increase
peripheral resistance to hormones.
Non-functioning tumor lead to pressure effect to
surrounding structure and may lead to decrease
secretion of hormones.
#Important points in history taking:
Past history:
o Tuberculosis and HIV infection are associated
with adrenal insufficiency.
Drug history:
o Excessive corticosteroid exposure causes
cushingoid features.
o Dopamine antagonist drugs such as haloperidol
and domperidone cause hyperprolactinaemia.
Family history:
o Thyroid disease and diabetes mellitus may run in
families.
o Multiple endocrine neoplasia syndromes are rare autosomal dominant conditions
characterized by hyperplasia, adenoma formation and malignant change in multiple
endocrine glands.
#General endocrine examination:
Demeanour, mental state:
o Restless and agitated (hyperthyroidism).
o Slow and lethargic (hypothyroidism).
General appearance:
o Central obesity (Cushing’s syndrome)
Face:
o Features of Cushing’s syndrome, Addison’s disease, and Acromegaly.
o Inspect the face and eyes for a 'spot' endocrine diagnosis.
Eyes:
o Look for features of thyroid disease.
o Assess visual acuity and perform fundoscopy in patients with diabetes mellitus.
o Assess visual acuities and fields in patients with suspected pituitary tumors.

4
o Bitemporal hemianopia (due to compression of the optic chiasm by pituitary
tumor)
o Optic atrophy (longstanding optic pathway compression)
o Exophthalmos and Ophthalmoplegia.
Mouth:
o Overgrowth of the chin and tongue (acromegaly)
o Buccal pigmentation (Addison's disease).
Neck:
o Examine the neck for goiter. If present, record its size, surface and consistency.
Hand:
o Tremor and palmar sweating (hyperthyroidism)
o Soft-tissue overgrowth (acromegaly)
o Large, sweaty, fleshy (acromegaly)
o Dysmorphism is abnormal metacarpal length (pseudohypoparathyroidism)
o Skin crease pigmentation (Addison's disease)
o Wasting of the thenar muscles due to carpal tunnel syndrome (hypothyroidism,
acromegaly).
o Palmar erythema.
Breast:
o Gynecomastia (Klinefelter's syndrome), galactorrhoea.
Chest:
o Look for a thoracic kyphosis, which may be a sign of osteoporotic vertebral
collapse.
Abdomen:
o Purple striae (Cushing's syndrome)
o Palpable, nodular liver, which is sometimes massively enlarged (Carcinoid
syndrome)
External genitalia:
o Inspect the amount of pubic hair and make a pubertal staging of all adolescents
using Tanner grading.
o In men, record testicular size and consistency.
o In women, look for virilising features.
Legs:
o Pretibial myxedema (Graves 'disease)
o Proximal muscle wasting or weakness (Cushing's syndrome and hyperthyroidism)
o Delayed tendon reflexes (hypothyroidism)
o Signs of diabetic neuropathy, ischemia, ulcers (diabetes mellitus)
o Pretibial myxedema, Necrobiosis lipoidica.
Skin surface:
o Abnormal pallor (hypopituitarism)
o Vitiligo, skin or scar pigmentation (Addison's disease)
o Plethora (Cushing's or carcinoid syndrome)
o thin, fragile skin with bruising after trivial trauma (Cushing's syndrome)
o Acanthosis nigricans in axilla and groin (obesity, diabetes mellitus)

5
Body hair:
o Is the body hair normal in quality and amount?
o Hirsutism in females (polycystic ovary syndrome)
o Loss of hair in the axillae and groins (hypopituitarism)
Bone:
o Osteoporosis (hyperthyroidism, Cushing’s syndrome, hypogonadism {loss of height,
thoracic kyphosis})
Pulse:
o Assess the pulse rate, rhythm and volume.
o Tachycardia and atrial fibrillation (thyrotoxicosis)
Blood pressure:
o Hypertension (Cushing's syndrome, Phaeochromocytoma, Conn's syndrome)
o Postural hypotension (adrenal insufficiency)
Measure the height and weight and calculate the body mass index:
o Use a stadiometer in children and adolescents.
o If the patient is obese, is the adiposity centrally distributed, e.g. Cushing's
syndrome or GH deficiency.
Urine: Test the urine for glucose, ketones, protein and nitrite.
Psychological:
o Formal psychological evaluation may be appropriate in selected patients (Cushing's
syndrome, hyperparathyroidism).
#Common clinical features in endocrine disease:
Weight gain: Hypothyroidism, polycystic ovary syndrome (PCOS), Cushing’s syndrome.
Weight loss: Hyperthyroidism, diabetes mellitus, adrenal insufficiency.
Short stature: Constitutional, non-endocrine systemic disease (e.g. coeliac disease),
growth hormone deficiency.
Delayed puberty: Constitutional, non-endocrine systemic disease, hypothyroidism,
hypopituitarism, primary gonadal failure.
Menstrual disturbance: PCOS, hyperprolactinaemia, thyroid dysfunction.
Diffuse neck swelling: Simple goiter, Graves’ disease, Hashimoto’s thyroiditis.
Excessive thirst: Diabetes mellitus or insipidus, hyperparathyroidism, Conn’s syndrome.
Hirsutism: Idiopathic, PCOS, Cushing’s syndrome, congenital adrenal hyperplasia.
Funny turns: Hypoglycemia, Phaeochromocytoma, neuroendocrine tumor.
Sweating: Hyperthyroidism, hypogonadism, acromegaly, Phaeochromocytoma.
Flushing: Hypogonadism (especially menopause), carcinoid syndrome.
Resistant hypertension: Conn’s syndrome, Cushing’s syndrome, Phaeochromocytoma,
acromegaly, renal artery stenosis.
Erectile dysfunction: Primary or secondary hypogonadism, diabetes mellitus, non-
endocrine systemic disease, medication-induced (e.g. beta-blockers, opiates).
Muscle weakness: Cushing’s syndrome, hyperthyroidism, hyperparathyroidism,
osteomalacia.
Bone fragility and fractures: Hypogonadism, hyperthyroidism, Cushing’s syndrome.

6
Altered facial appearance: Hypothyroidism, Cushing’s syndrome, acromegaly, PCOS.
#Common presenting symptoms are:
Appetite and/or weight change: in hyper/hypothyroidism, diabetes mellitus, Cushing’s
syndrome.
Polydipsia (excessive thirst) and/or polyuria (passing >3 litres urine/day): in diabetes
mellitus, diabetes insipidus or hyperparathyroidism.
Change in facial/body hair growth and distribution: in hypogonadism,
hypopituitarism, adrenal insufficiency, androgen excess.
Hirsutism: is the excessive growth of thick terminal hair in an androgen-dependent
distribution (upper lip, chin, chest, back, lower abdomen, thighs) in women.
Change in skin and mucosal pigmentation and character:
o Coarse dry skin in hypothyroidism.
o Excessive pigmentation and/or vitiligo (areas of depigmented skin) in Addison’s
disease.
o Soft-tissue overgrowth and skin tags in acromegaly.
o Acanthosis nigricans (velvety thickening and pigmentation of the major flexures,
especially the axillae and groins) in obesity, and type 2 diabetes.
Increased sweating: in acromegaly and phaeochromocytoma.
Temperature intolerance: in hyperthyroidism (heat) and hypothyroidism (cold)
Change in sexual function:
o erectile dysfunction or loss of libido in hypogonadism
o gynaecomastia (breast tissue enlargement in men)
o galactorrhoea (breast milk production in men, or in women out with pregnancy or
breastfeeding) in pituitary adenomas producing hyperprolactinaemia
o primary or secondary amenorrhoea in pituitary or hypothalamic disease
Tiredness: can be a non-specific feature of diabetes mellitus, hypothyroidism or
Addison’s disease.
#Symptoms of gonadal diseases:
Klinefelter's syndrome (47XYY) Look for soft, finely wrinkled, hairless facial skin and
gynecomastia and examine the genitalia (pubic hair is often reduced/absent and the
testes <3 ml in volume).
Polycystic ovary syndrome cause Hirsutism.
Virilisation is temporal recession of the scalp hair, deepening of the voice, breast
atrophy, increased muscle bulk and clitoromegaly.
Testosterone-secreting tumor women with a short history of severe hirsutism.
#Symptoms of carcinoid syndrome:
Flushing, diarrhea, bronchospasm due to liver secretion of vasoactive chemicals.
Bending, exercise, even palpation of the enlarged liver may induce typical skin
flushing.
Permanent facial telangiectasia occurs after many years of carcinoid flushing.
7
Part2:
Thyroid gland
#History of patient with thyroid gland diseases:
Presenting complaint, ask about:
o Recent weight loss/gain, appetite change, diarrhea or constipation.
o Irritability, difficulty sleeping, hyperactivity or excessive fatigue.
o Heat or cold intolerance.
o Tremor, palpitation or excessive sweating.
o Skin or hair changes (excessive dryness or sweating, coarse dry hair or alopecia).
o Eye symptoms: diplopia, pain, irritation or 'grittiness'.
Past drug, family and social history, ask about:
o Drug therapy (amiodarone and lithium are associated with hypothyroidism),
antithyroid drugs.
o Family history of thyroid or autoimmune disease.
o Living in areas of iodine deficiency, e.g. the Andes, Himalayas, Central Africa, can
cause goitre and, rarely, hypothyroidism.
#Examination of patient with thyroid gland diseases:
1- General:
Look for:
o Signs of weight loss or gain.
o Agitation, restlessness or apathy and lethargy.
o The facial appearance and expression.
Examine:
o Hands
o Pulse and blood pressure (BP)
o Arms and legs for: skin abnormalities, muscle power and the deep tendon reflexes.
o The eyes for:
Exophthalmos, diplopia, conjunctival edema or conjunctivitis, corneal ulceration.
Lid retraction: this is present if the sclera is visible above the iris.
8
Lid lag: ask the patient to follow your index finger as you move it from the upper
to the lower part of his visual field. Delay between the descent of the upper
eyelid in relation to that of the eyeball is lid lag.
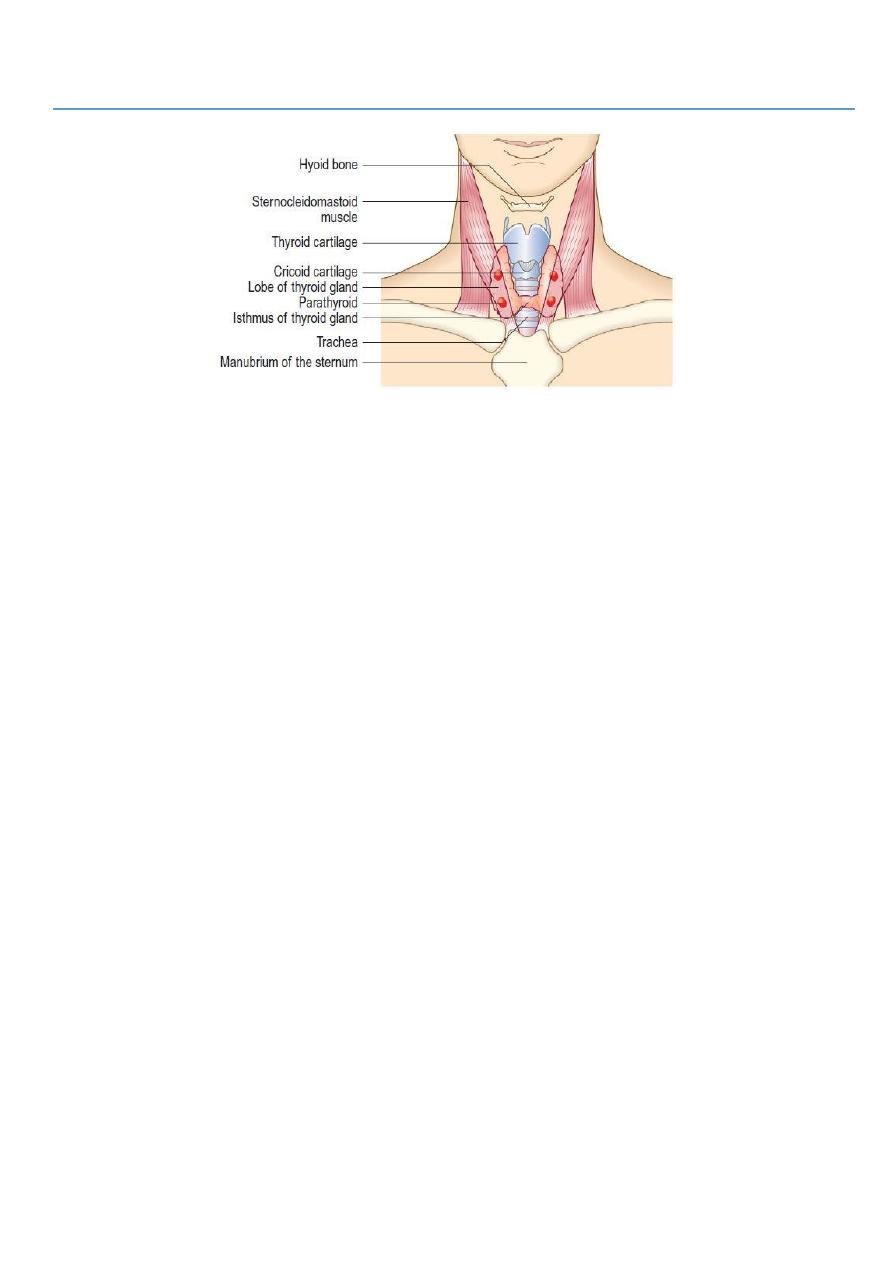
2- Thyroid:
Inspect the neck from the front: Give the patient a glass of water and ask him to take a
sip. Look for a swelling while he swallows.
Ask the patient to sit with the neck muscles relaxed and stand behind him. Place your
hands gently on the front of the neck, with your index fingers just touching. Ask him to
swallow a sip of water and feel the gland as it moves upwards. Some patients find neck
palpation uncomfortable, so be alert for any signs of distress.
Note the size, shape and consistency of any goiter and feel for any thrill.
Measure any discrete nodules with callipers.
Record the maximum neck circumference of a large goiter using a tape measure.
Auscultate with your stethoscope for a thyroid bruit. A thyroid bruit may be confused
with other sounds: bruits from the carotid artery or transmitted from the aorta are
louder along the line of the artery. Transient gentle pressure over the root of the neck
will interrupt a venous hum from the internal jugular vein.
#Findings:
Normal findings
o The normal thyroid gland is palpable in ~50% of women and 25% of men.
o Prominent skin folds may give a false impression of goiter.
o The thyroid (or a thyroglossal cyst) moves upwards on swallowing since it is
enveloped in the pre-tracheal fascia, which is attached to the cricoid cartilage.
Abnormal findings
o Shape, surface and consistency
Simple goiters are relatively symmetrical in their earlier stages but often
become nodular with time.
Graves’ disease the surface of the thyroid gland is usually smooth and diffuse;
it is irregular in uninodular or multinodular goiter.
Nodules in the substance of the gland may be large or small, and single or
multiple, and are usually benign.
Malignancy A very hard consistency.
Thyroid cancer Large, firm lymph nodes near a goiter.
Viral thyroiditis diffuse tenderness.
Localized tenderness may follow bleeding into a thyroid cyst.
o Mobility
Most goiters move upwards on swallowing.
Very large goiters may be immobile.
Invasive thyroid cancer may fix the gland to surrounding structures.
o Thyroid bruit
This may occur in hyperthyroidism.
Indicates abnormally high blood flow.
There can be an associated palpable thrill.
9
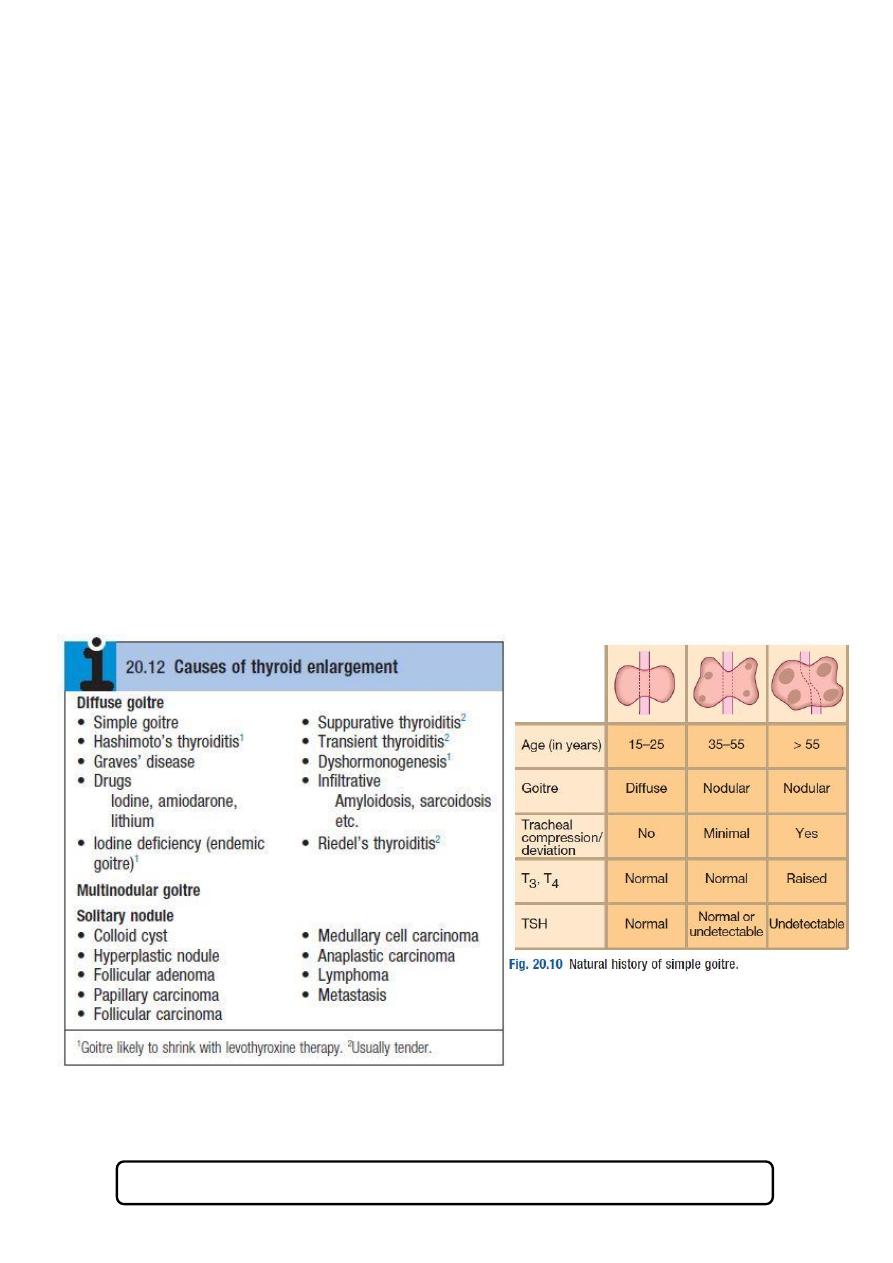
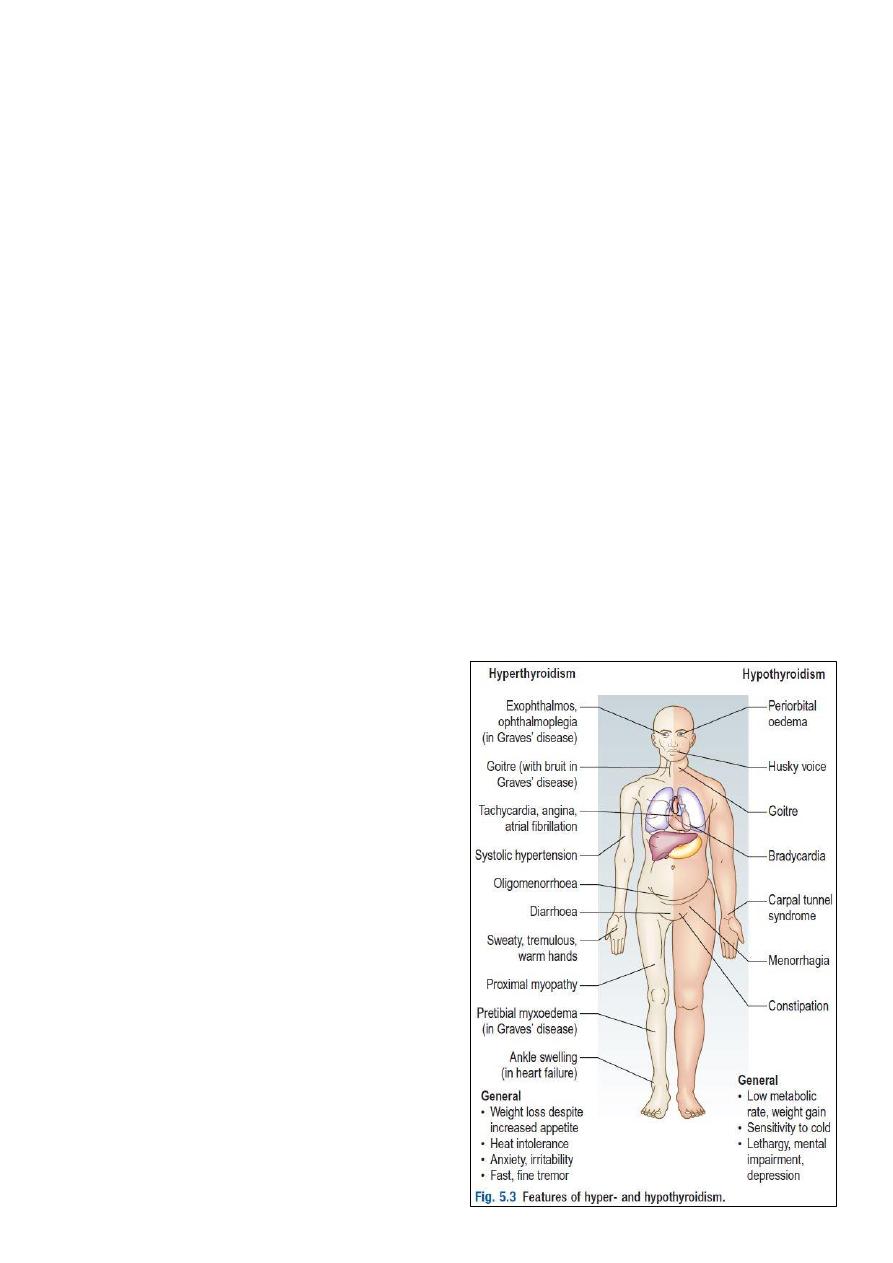
#Diseases of the thyroid gland:
Goiter is enlargement of the thyroid gland.
Hyperthyroidism (thyrotoxicosis) is a clinical state caused by increased levels of
circulating levels of the thyroid hormones, T3 and T4. Graves’ disease is the
commonest cause of hyperthyroidism.
Hypothyroidism is caused by reduced levels of thyroid hormones and is usually due to
autoimmune Hashimoto’s thyroiditis.
#Specific extra-thyroid features of Hyperthyroidism (thyrotoxicosis):
Exophthalmos (proptosis):
o It is increased protrusion of the eyeball from the orbit.
o It is caused by an inflammatory infiltration of the orbital contents (the soft tissues
and extra-ocular muscles, not the globe).
o It is usually bilateral.
Pretibial myxedema: Is a raised, discolored (usually pink or brown) indurated
appearance over the lower legs. It is associated with Graves’ disease, not
hypothyroidism.
Thyroid acropachy: is a periosteal hypertrophy of the distal phalanges which looks like
finger clubbing.
See this video http://www.muhadharaty.com/lecture/1198
11
#Causes of thyrotoxicosis:
Graves’ disease.
Multinodular goiter.
Solitary thyroid adenoma.
Thyroiditis.
Iodide-induced: Drugs (amiodarone), Radiographic contrast media, Iodine prophylaxis
programme.
Extrathyroidal source of thyroid hormone: Factitious thyrotoxicosis, Struma ovarii.
TSH-induced.
TSH-secreting pituitary adenoma: Choriocarcinoma and hydatidiform mole.
Follicular carcinoma ± metastases.
#Causes of hypothyroidism:
Autoimmune: Hashimoto’s thyroiditis, Spontaneous atrophic hypothyroidism, Graves’
disease with TSH receptor blocking antibodies.
Iatrogenic: Radioactive iodine ablation, Thyroidectomy, Drugs (Carbimazole,
methimazole, propylthiouracil, Amiodarone, Lithium)
Transient thyroiditis: Subacute (de Quervain’s) thyroiditis, Post-partum thyroiditis.
Iodine deficiency: in mountainous regions.
Congenital: Dyshormonogenesis, Thyroid aplasia.
Infiltrative: Amyloidosis, Riedel’s thyroiditis, sarcoidosis etc.
Secondary hypothyroidism: TSH deficiency.
#The counteracting hormones:
They are the hormones that counter act
the function of insulin.
They increase the level of glucose in
blood (energy).
They are the following thyroxin,
glucagon, hydrocortisone, adrenaline,
nor-adrenaline.
#Notes on thyroid hormones:
Functions of them: give energy to the
body + differentiation of cells.
99% of thyroid hormone are bound to
thyroxin binding globulin (TBG).
The diagnosis of hyper or hypo
thyrodisim is made by biochemical
tools.
11
Part3:
Parathyroid gland
#Symptoms of parathyroid gland diseases:
Parathyroid disease commonly asymptomatic.
Hyperparathyroidism the commonest symptoms relate to hypercalcaemia:
polyuria, polydipsia, renal stones, peptic ulceration, tender areas of bone fracture
deformity 'Brown tumors', and confusion or psychiatric symptoms.
Hypoparathyroidism hypocalcaemia may cause hyperreflexia or tetany (involuntary
muscle contraction), most commonly in the hands or feet. Paresthesia of the hands and
feet or around the mouth may occur.
Pseudohypoparathyroidism end-organ resistance to parathyroid hormone and
typically have short stature, round face and shortening of some metacarpal bones.
#History of patient with parathyroid gland diseases:
Recent thyroid or neck surgery or irradiation.
Polyuria, polydipsia or renal stones.
Fractures.
Abdominal pain or constipation.
Muscle cramps.
Confusion or psychiatric symptoms.
#Examination of patient with parathyroid gland diseases:
Look at the neck for scars of previous surgery.
Assess mental state.
Take the BP and assess the state of hydration.
Look at the hands. Ask the patient to make a fist and assess the length of the
metacarpals.
Test for muscle weakness and hyperreflexia.
Test for latent tetany: place a BP cuff on the upper arm and inflate above systolic
pressure for 3 minutes. In the hand, carpal muscle contraction produces a typical
picture with the thumb adducted, the proximal interphalangeal and distal
interphalangeal joints extended and the metacarpophalangeal joints flexed ('main d'
accoucheur' (hand of the obstetrician) or Trousseau's sign).
Look for evidence of recent fractures and bone tenderness.
Use a slit lamp to look for corneal calcification.
Perform urinalysis.

12
#Abnormal findings:
Parathyroid tumors are very rarely palpable.
Hyperparathyroidism may cause altered mental state, dehydration, proximal muscle
weakness, fractures and bony tenderness.
Long-standing hypercalcaemia may cause corneal calcification (band keratopathy).
Moderate/severe hypocalcaemia cause hyperreflexia and a positive Trousseau’s
sign.
Pseudohypoparathyroidism the metacarpals of the ring and little fingers are
shortened.
13
Part4:
Pancreas
#Examination of patient with diabetes mellitus:
Note: Careful examination of the eyes, cardiovascular, neurological and renal systems, and
feet is essential.
Look for evidence of weight loss and dehydration.
Smell the patient's breathe for the sweet smell of ketones (diabetic ketoacidosis).
Examine the skin:
o Look for signs of infection and rashes.
o Look for xanthelasma and xanthomata.
o Examine insulin injection sites for evidence of lipohypertrophy (which may cause
unpredictable insulin release), lipoatrophy (rare) or signs of infection (very rare).
Measure pulse and BP and examine the cardiovascular and peripheral vascular
systems.
Examine the respiratory and gastrointestinal systems.
Examine the central nervous system.
Test visual acuity and examine the eyes and optic fundi.
Perform urinalysis.
#Abnormal findings:
Ketoacidosis cause dehydration and
Kussmaul's respiration (hyperventilation with
a deep, sighing respiratory pattern).
Bacterial skin infections e.g. cellulitis,
boils, abscesses and fungal infections.
Acanthosis nigricans occurs in
hyperinsulinism and is seen frequently in
patients with insulin-resistant type 2
diabetes.
Necrobiosis lipoidica (a yellow indurated
or ulcerated area surrounded by a red
margin), due to collagen degeneration, may
occur on the shins of some type 1 diabetic
patients and often causes chronic ulceration.
Xanthelasmata and Xanthomata indicate significant hyperlipidemia.
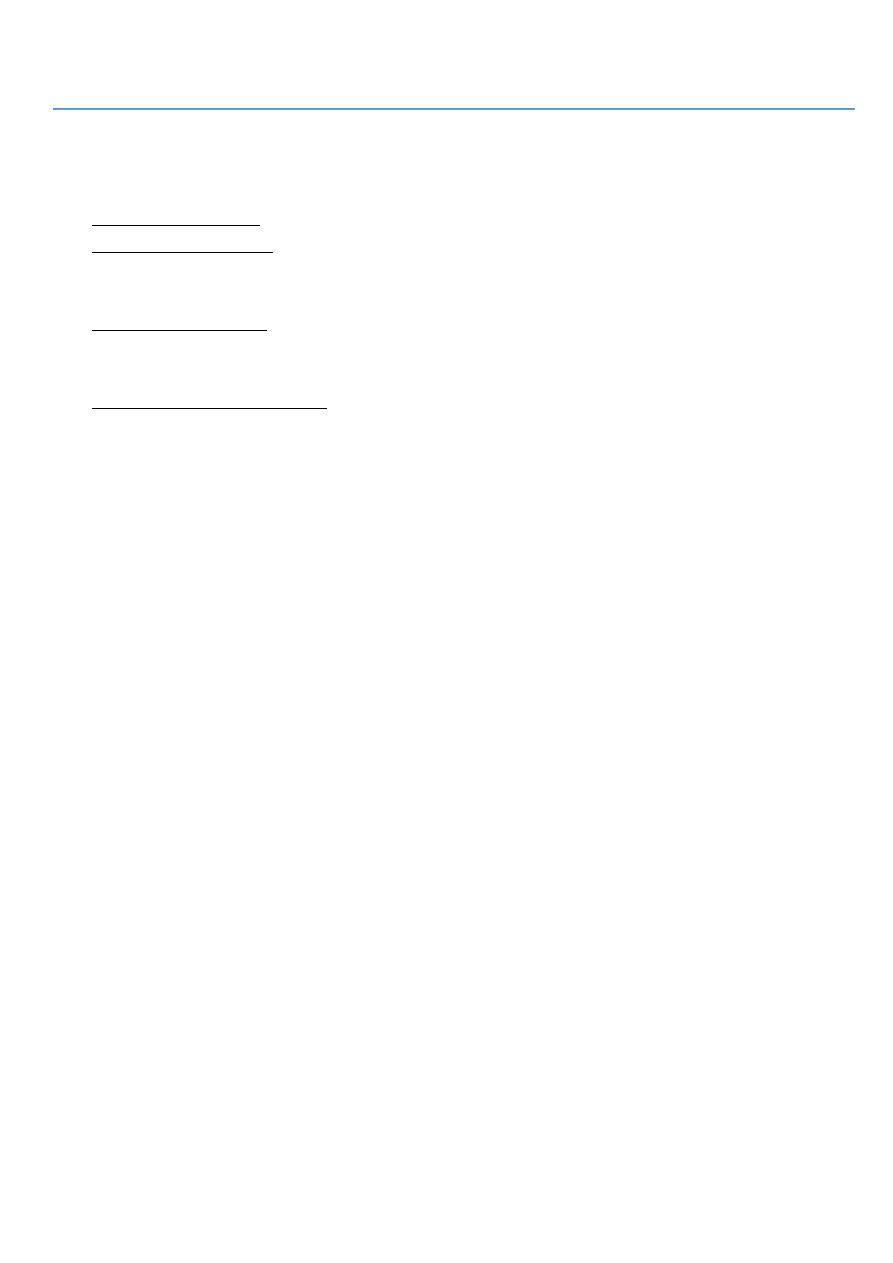
Microvascular, neuropathic and macrovascular complications of hyperglycemia can
occur in patients with any type of diabetes mellitus, and may be present at diagnosis in
patients with slow-onset type 2 disease.
Glycosuria suggests hyperglycemia and, if accompanied by ketonuria (and
Kussmaul's respiration) indicates ketoacidosis.
Proteinuria occurs in diabetic nephropathy.
Detection of nitrite ± hematuria suggests (often occult) urinary infection.
#Diabetic foot:
Important
14
Diabetic patients have a 15% lifetime risk of foot ulcers, which are highly susceptible to
infection. Early recognition of the 'at-risk' diabetic foot is essential. There are two main
presentations:
Neuropathic: where neuropathy predominates but the major arterial supply is intact.
Neuro-ischemic: where reduced arterial supply produces ischemia and exacerbates
neuropathy.
Infection complicates both presentations.
#Examination of diabetic foot:
Inspection:
o Look for hair loss and nail dystrophy.
o Examine the skin (including the interdigital clefts) for excessive callus, infections
and ulcers.
o Ask the patient to stand and assess the foot arch.
o Look for deformation of the joints of the feet.
Palpation:
o Feel the temperature of the feet.
o Examine the dorsalis pedis and posterior tibial pulses. If absent, arrange Doppler
studies to evaluate ankle brachial pressure index.
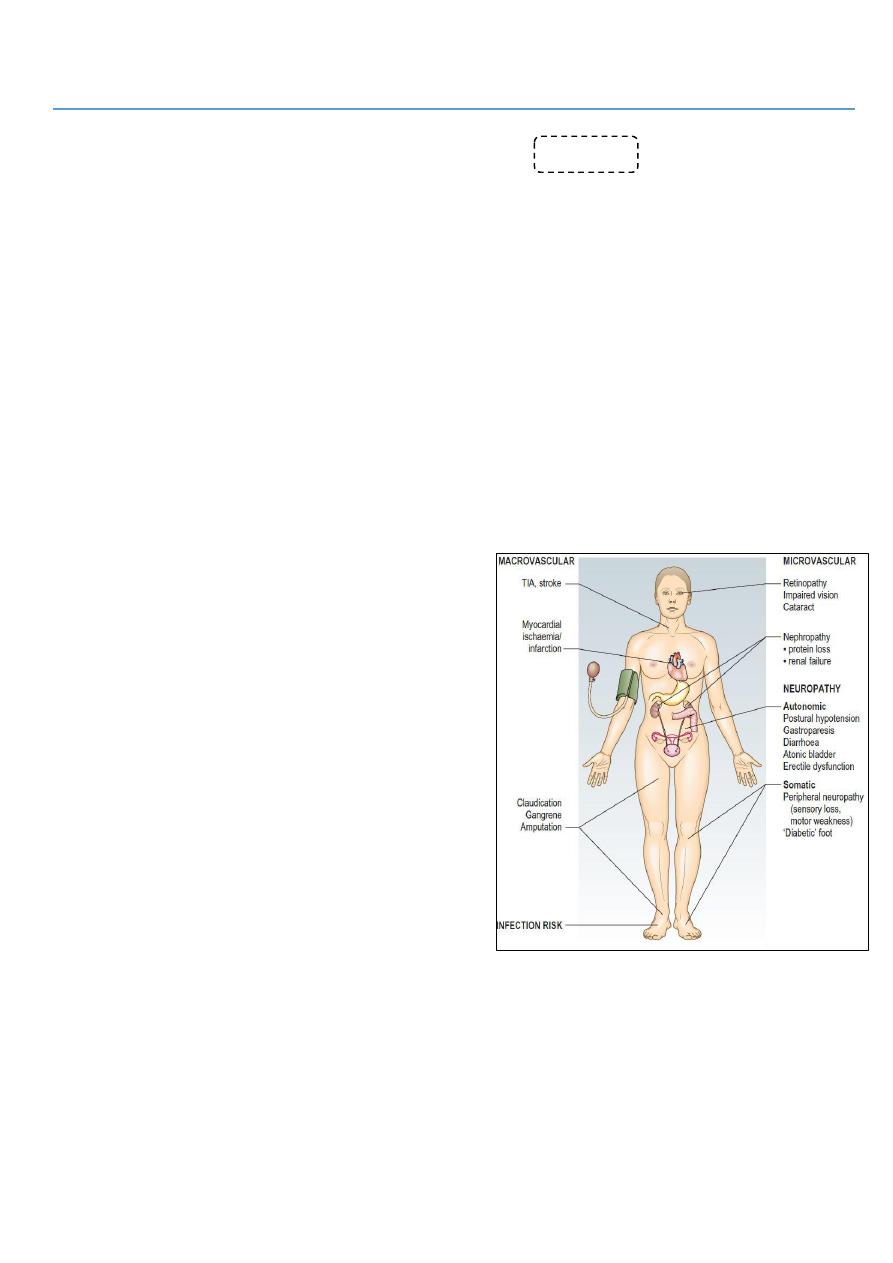
Test for peripheral neuropathy: use a nylon monofilament which buckles at a force of
10 g to apply a standard, reproducible stimulus. Avoid areas of untreated callus.
#Abnormal findings:
Hair loss and nail dystrophy occur with ischemia, causing nutritional changes.
There may be skin fissures or tinea infection (‘athlete’s foot’).
The foot arch may be excessive in neuropathy or collapsed (rocker-bottom sole).
Both conditions cause abnormal pressures and increase risk of plantar ulceration.
Warm feet occur in neuropathy and cold feet in ischemia.
Sensory neuropathy is present if the patient cannot feel the monofilament in any of the
sites. This means loss of protective pain sensation and is a good predictor of future
ulceration.
Charcot’s arthropathy is disorganized foot architecture, acute inflammation, fracture
and bone thinning, usually in a patient with neuropathy but relatively good vascular
supply to the lower limb. It presents acutely as a hot, red, swollen foot often
impossible to distinguish clinically from infection.
#Risk assessment of diabetic foot:
Low no risk factors (no sensation loss,
peripheral vascular disease or other risk factors).
Moderate one risk factor present.
High previous ulceration or amputation, or
more than one risk factor present.
Active ulceration, spreading infection, critical
ischemia, unexplained red, hot, swollen foot.

15
Part5:
Pituitary and adrenals
#Pituitary diseases:
Acromegaly pituitary tumors secrete excess growth hormone (before puberty it is
called gigantism).
Anterior hypopituitarism is due to compression of the pituitary by a
macroadenoma, infarction after childbirth (Sheehan’s syndrome), severe head trauma,
cranial radiotherapy.
#Growth hormone (G.H) change diseases:
Decrease G.H secretion before puberty Dwarfism treated by giving G.H
injection for 6 weeks or more if the child less than 10 years old.
Decrease G.H secretion after puberty Lethargy.
Increase G.H secretion before puberty Gigantism.
Increase G.H secretion after puberty Acromegaly (Acro means periphery).
Presenting features of acromegaly:
o Early: Shoes, cloths, rings become smaller / bone pain / large periphery like nose,
forehead, lips, tongue, limbs, heart.
o Late: Pale, dizzy due to hypo-pituitarism which occur due to pressure effect of
macro-adenoma that secret G.H.
#History of patient with acromegaly:
Ask about the most common symptoms: headache and excessive sweating.
Has the patient (or more often a relative or friend) noticed changes in his facial
features?
Photographs taken years earlier can be helpful to identify changes and the onset of the
condition.
Has the patient noticed an increase in shoe, ring or glove size?
#Examination of patient with acromegaly:
Look at the face for coarsening of features, thick greasy skin, enlargement of the
nose, prognathism (protrusion of the mandible) and separation of the lower teeth.
Examine the hands and feet look for soft-tissue enlargement and complications
arising from this, e.g. tight-fitting rings or shoes, carpal tunnel syndrome.
Assess the visual fields expansion of the tumor can cause pressure on the optic
chiasm, resulting in visual field defects, especially bitemporal hemianopia.
Check the BP and perform urinalysis Hypertension and diabetes mellitus are
common associations.
#Examination of patient with Hypopituitarism:
Extreme skin pallor a combination of mild anemia and melanocyte-stimulating
hormone deficiency.
Absent axillary hair.
Reduced/absent secondary sexual hair caused by gonadotrophin deficiency.
T
esticular atrophy.

16
Examine the eyes for
o Visual field defects (most often bitemporal hemianopia).
o Optic atrophy or cranial nerve defects (III, IV and VI) caused by a tumor
compressing the optic chiasm, optic nerve or cavernous sinus.
#Non- functioning tumor in pituitary gland:
Lead to pressure effect on the pituitary gland.
So decrease the secretion of some hormones start from least important to most
important First is LH + FSH G.H TSH ACTH.
Start treatment by replacement the most important hormone at first which is ACTH
then TSH then LH + FSH and if needed you can replace G.H.
Don't give thyroxin unless there is adequate level of hydrocortisone in the body
because if you give thyroxin with absence of cortisol there will be crisis. If you not
sure about the level of cortisol you can give both thyroxin + hydrocortisone.
Lead to pressure effect on optic chiasma lead to Bitemporal hemiplegia.
#Adrenal gland diseases:
Increase medulla hormones secretion (adrenals) Phaeochromocytoma.
Increase cortex hormone secretion (cortisol) Cushing's syndrome.
Decrease cortex hormone secretion (cortisol) Primary Addison's disease.
Increase cortex hormone secretion (aldosterone) Conn's syndrome also called
primary hyperaldosteronisim, features:
o Hypertension refractory to treatment, or in young patient.
o Hypokalemic alkalosis (because the renal tubules will excrete hydrogen and
absorb sodium).
Cushing's syndrome caused by excess exogenous or endogenous corticosteroid
exposure like: iatrogenic, ACTH-secreting pituitary microadenoma, primary adrenal
tumor, ectopic ACTH secretion.
Addison’s disease due to inadequate secretion of cortisol, usually secondary to
autoimmune destruction of the adrenal cortex.
#Function of cortisol:
Maintain vascular changes in posture changes and other condition (hypo/hyper
tension).
Maintain sugar level in the blood.
#Secondary Addison's disease:
Decrease in the ACTH or adrenal hormone, due to extra-adrenal cause like tumor in
the pituitary gland and other diseases.
Lead to postural hypotension.
Hypoglycemic attack (palpitation, confusion, convulsion, coma, others).
Hepatic failure.
Lethargy and other non-specific features.
17
Decrease in aldosterone (hypotension, hyperkalemic alkalosis)
In primary Addison's disease there is color change but in secondary there is no color
change in the patient the cause of color changes is there is pro-hormone which
divided into two component, one of them is ACTH and the other is melanocyte
stimulating hormone which change the color of the body into darker color.
#Examination of patient with Cushing's syndrome:
Look at the face and general
appearance for central obesity
and a round face.
Examine the skin for thinning,
hyperpigmentation, acne,
hirsutism, bruising, striae
(especially abdominal) and signs of
infection or poor wound healing.
Examine the legs for evidence
of proximal muscle weakness and
edema.
Examine the eyes for cataracts,
and hypertensive changes.
Check the BP.
Perform urinalysis.
#Examination of patient with Addison’s disease:
Look for signs of weight loss.
Examine the entire skin surface for
o Abnormal or excessive pigmentation: this is most prominent in sun-exposed areas
or epithelia subject to trauma or pressure – skin creases, buccal mucosa and recent
scars.
o Excess pigmentation is produced by melanocyte-stimulating hormone in primary
adrenal insufficiency. It is most striking in white Europeans.
o Vitiligo (depigmentation of areas of skin) occurs in 10–20% of Addison's disease
cases.
Check the BP and test for postural hypotension Hypotension and postural
hypotension result from reduced mineralocorticoid effects.