
Checking of Anaesthetic
Equipment
Description
Anaesthetic practice involves the extensive daily use of equipment. Routine
checking of this equipment is essential in the safe delivery of anaesthetic care.
This session provides an overview of the principles of checking the anaesthetic
equipment used in current common practice, in accordance with the
recommendations of the Association of Anaesthetists in Great Britain and
Ireland.

Session introduction
Learning objectives:
• Describe the tests performed in checking the
anaesthetic equipment.
• Identify potential equipment malfunctions in
anaesthetic practice.
• Recognize the design modifications of modern
anaesthetic equipment to prevent such
malfunction.

introduction
• Anaesthetic practice
involves the extensive,
daily use of equipment.
Routine checking of this
equipment is essential
for the safe delivery of
anaesthetic care.
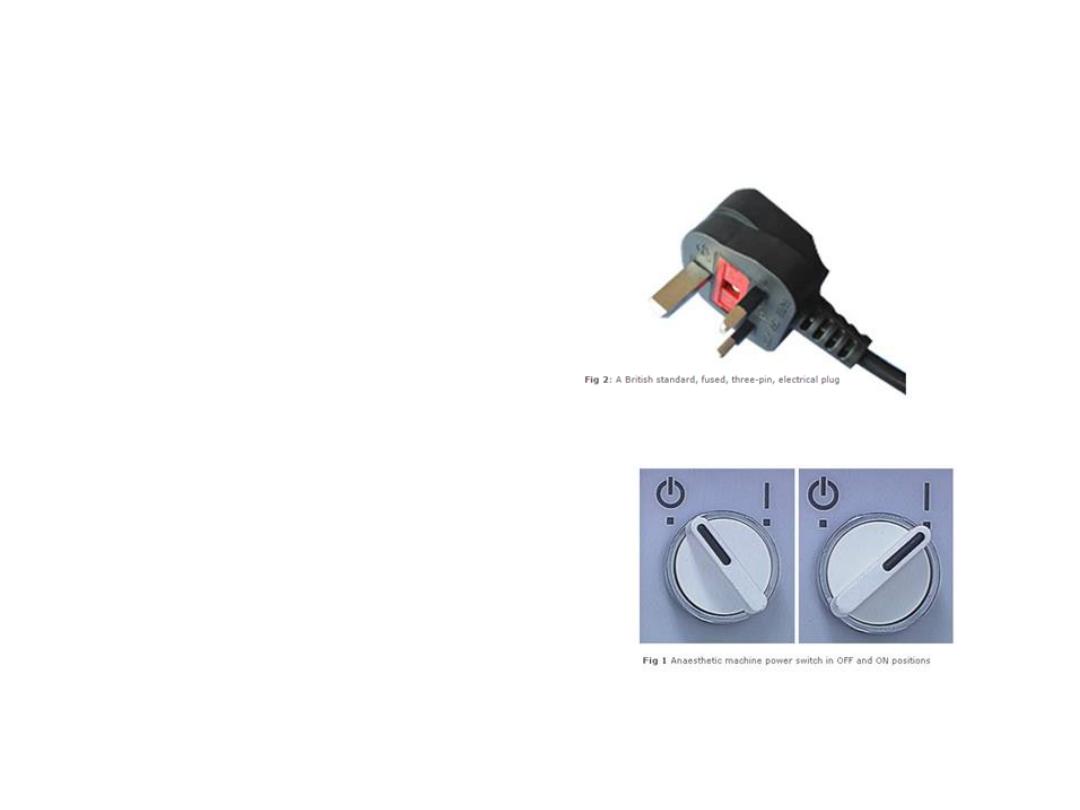
The anaesthetic machine
• The majority of modern
anaesthetic machines are
electrically powered. So the
first thing to do is to ensure
that your anaesthetic
machine is connected to the
mains and that the power is
switched on at the wall
socket.
• Some anaesthetic machine
designs have an on/off
switch. If your machine has
one, switched it on.

Monitoring equipment
• Monitoring equipment
should be functioning
within appropriate alarm
parameters.
• Standards monitors:
• Non – invasive blood
pressure
• Gas monitoring and
capnography
• Oxygen analyzer
• Pules oximeter

None – invasive blood pressure
In order to obtain an
accurate reading, an
appropriately sized blood
pressure cuff should be
used.
A guide to the correct
width of the cuff:
• 3cm: infant
• 6cm: child
• 9cm: small adult
• 12cm: standard adult cuff
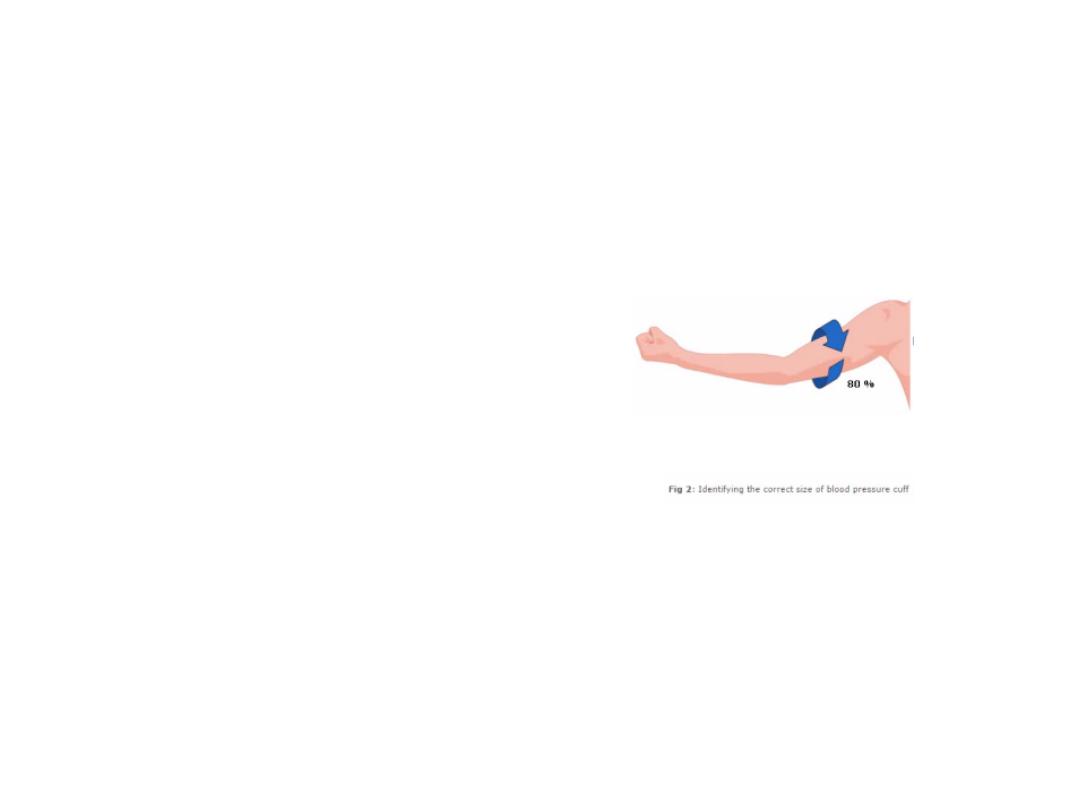
None – invasive blood pressure
• To identify the correct size of the
cuff, estimate the circumference
of the upper arm at mid point
between shoulder and elbow. The
bladder inside the cuff should
encircle at least 80% of the arm
circumference. The width of the
cuff should be 20% more than the
diameter of the arm. The cuff
should be placed so that the
midline of the bladder is over the
arterial pulsation. Also, adjust the
frequency of measurements
according to the clinical condition
of the patient and the type of
surgery. This is usually done every
3 or 5min.

Medical gas supply
pipeline supply
When checking medical gas supply,
you must identify and check the gas
pipeline. These are color coded:
•
White: oxygen
•
Blue: nitrous oxide
•
Black: medical air
•
Yellow: suction
•
Pink: scavenging
A tug test is done to confirm that
each pipeline is correctly inserted and
engaged into the appropriate gas supply
terminal. Inadequately inserted sockets
can appear to stay attached to the
terminal even when hanging vertically. In
this case, their would be no gas flow.
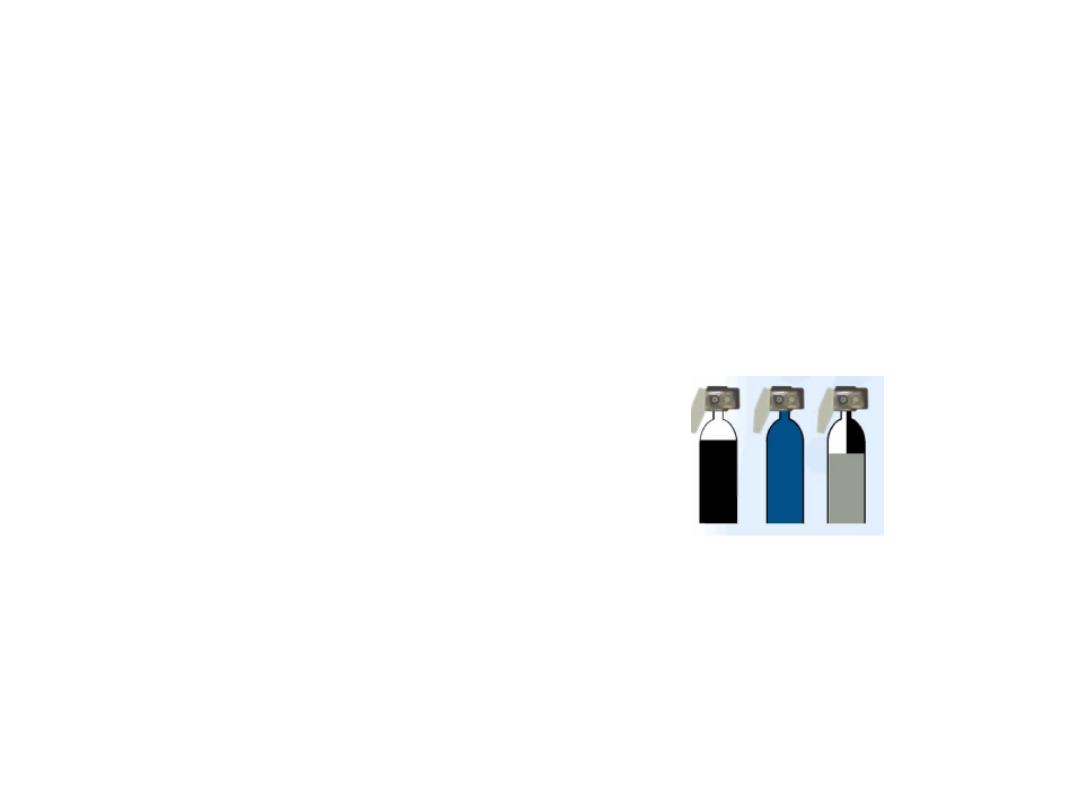
Medical gas supply
reserve gas cylinders
Reserve gas cylinders
should be available to ensure a
continuous supply of medical
gases, even in cases of central
gas supply failure.
Normally, oxygen, nitrous
oxide and air cylinders are
attached to the anaesthetic
machine as a reserve supply.
Carbone dioxide cylinders
should not normally present
on the anaesthetic machine
due to risk of administering
high concentration of CO2.
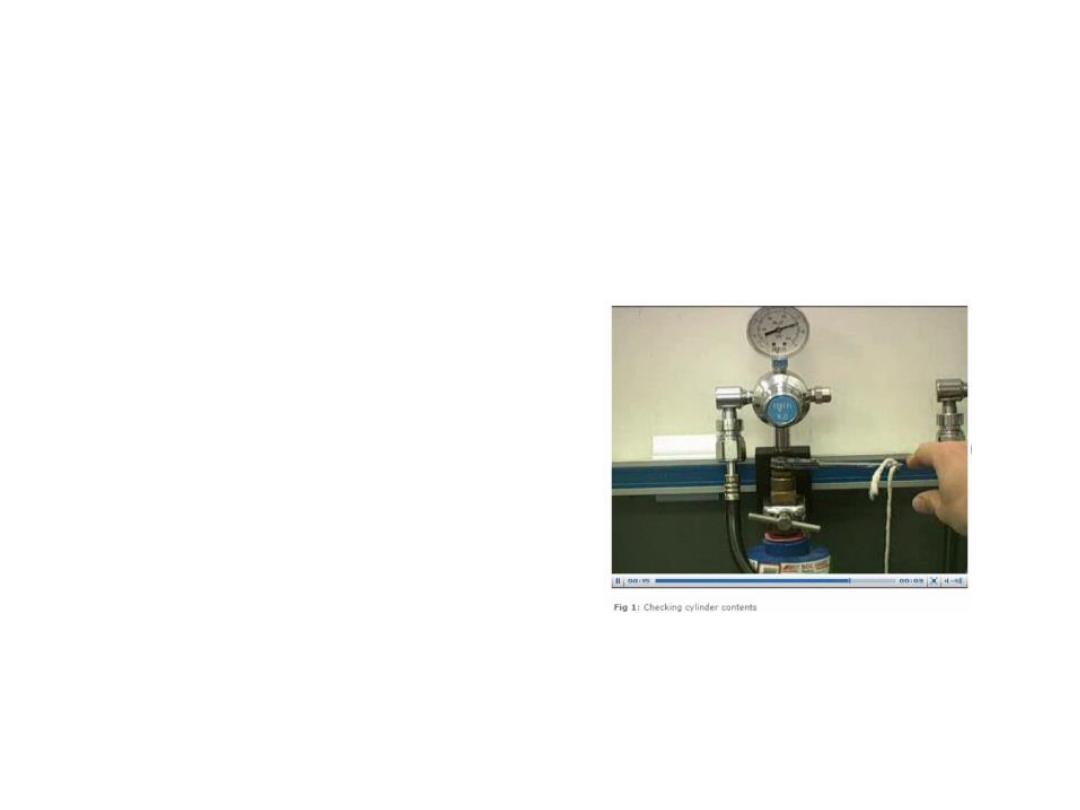
Seating, connecting and checking
reserve cylinders
The reserve oxygen,
nitrous oxide and medical
air cylinder will need to be
securely seated onto the
anaesthetic machine. They
should then be connected
and their contents checked.
After you have checked
the contents of these
cylinders, turn them off.
A blanking plug should be
fitted to any empty cylinder
yoke.
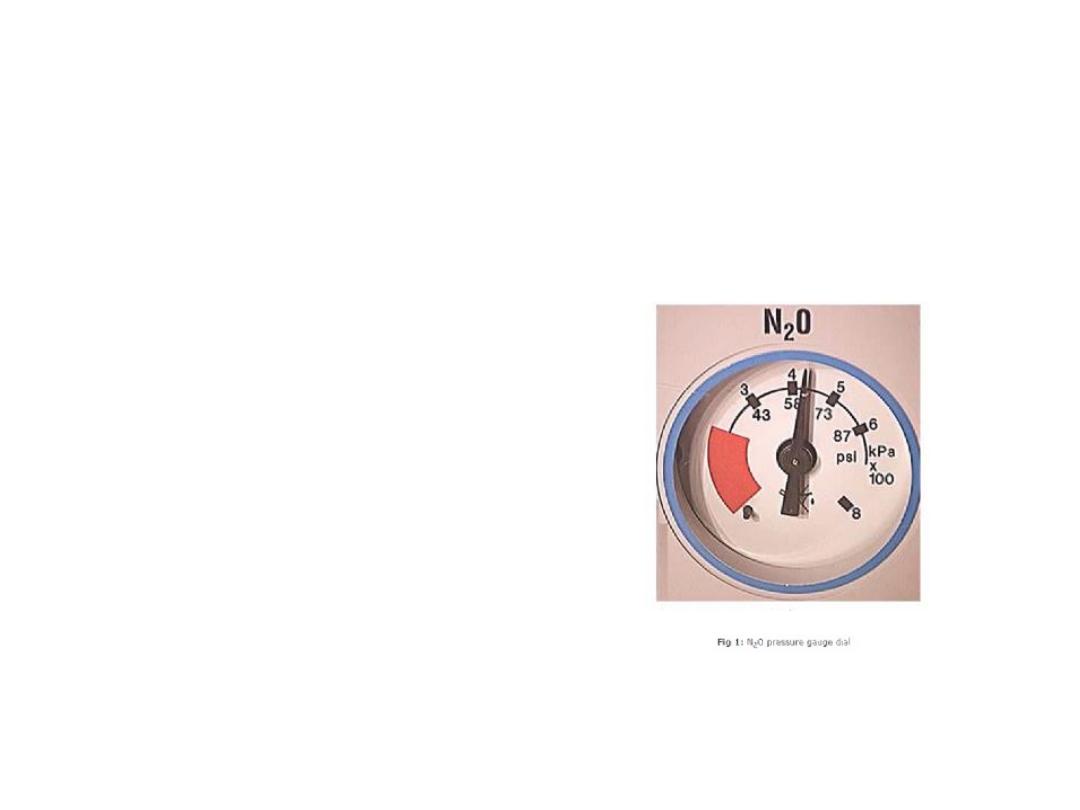
Checking pressure gauges
After you have ensured that each
pipeline is correctly inserted into the
appropriate gas supply terminal,
check the gauges pressure on the
anaesthetic machine.
The pressure gauges of pipelines
connected to the anaesthetic
machine should indicate 499 –
500KPa.
The readings of pressure gauges of
full oxygen, nitrous oxide and air
medical gas cylinders should be:
• Oxygen: 13700KPa (137bar)
• Nitrous oxide: 4400KPa (44bar)
• Medical air: 13700KPa (137bar)
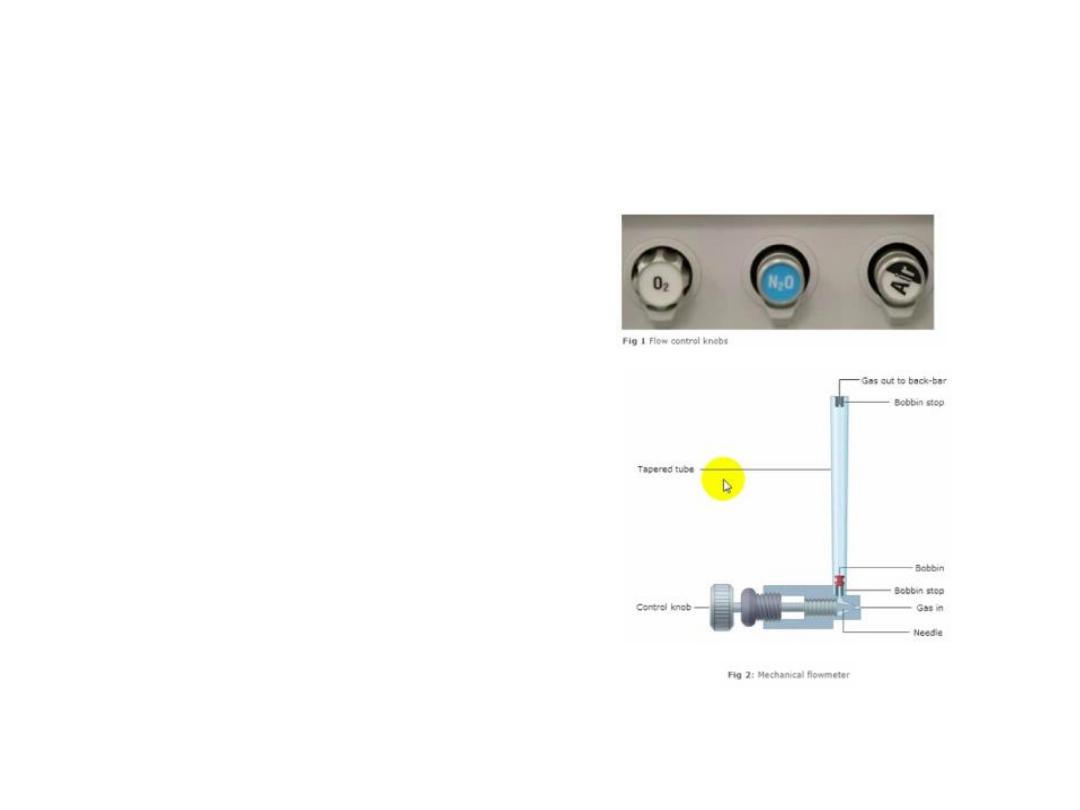
Medical gas supplies
mechanical flowmeters
• Although some
anaesthetic machine
have digital and
electronic flowmeters,
the majority have
mechanical ones.
• The bobbin should
move and rotate freely
at various flow rates.
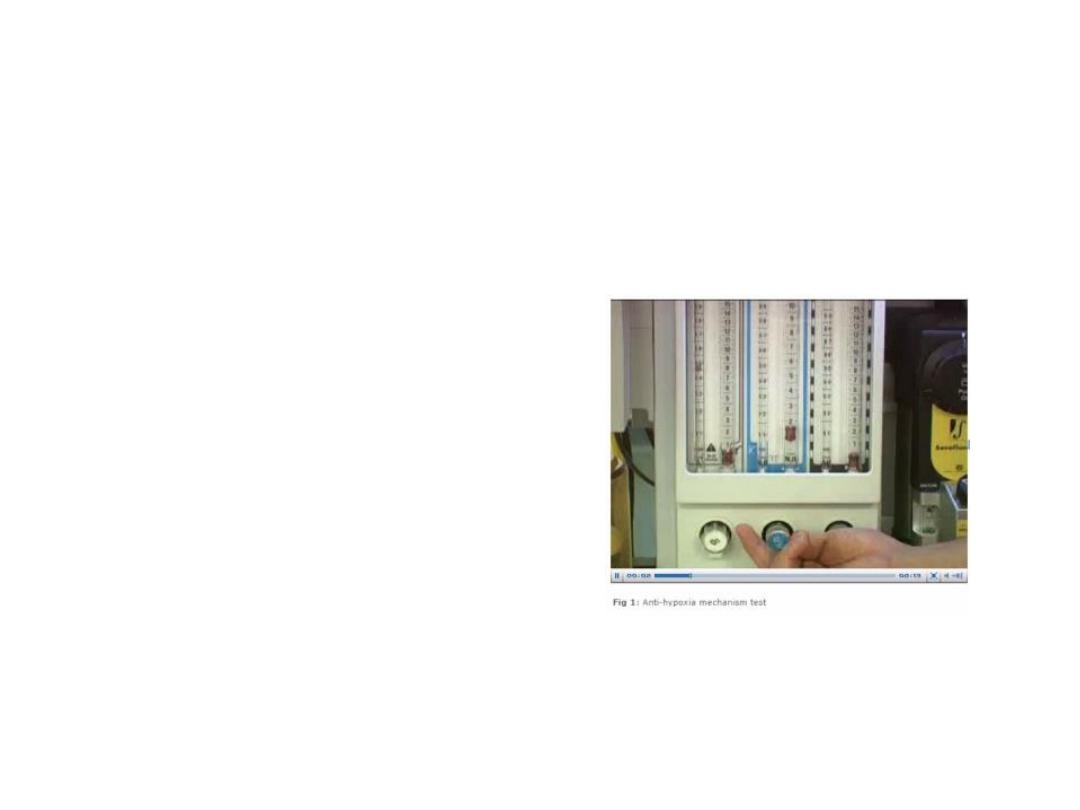
mechanical flowmeters
testing the anti - hypoxia device
• Anti – hypoxia device (the
means to prevent the delivery
of a gas mixture with an
oxygen concentration below
25%). This anti – hypoxia
device should be tested.
• Check the oxygen analyzer
function by turning on oxygen
flow. A reading approaching
100% should be displayed.
• Turn off all flow control valves.
(Some machines that are fitted
with a gas supply master
switch will continue to deliver
a basal flow of oxygen; about
250ml/min.

Oxygen flash
oxygen bypass
• The emergency oxygen bypass
control should be checked next.
When the bypass button is
pressed, the oxygen flow without
significant decrease in the
pipeline supply pressure. It is
important to check that the
control valve shuts off when the
button is released.
• The emergency oxygen flash,
when activated, supplies pure
oxygen with flow of about 35 –
75L/min at a pressure of about
400KPa.
• As a safety feature, the button is
recessed in a housing to prevent
accidental activation.
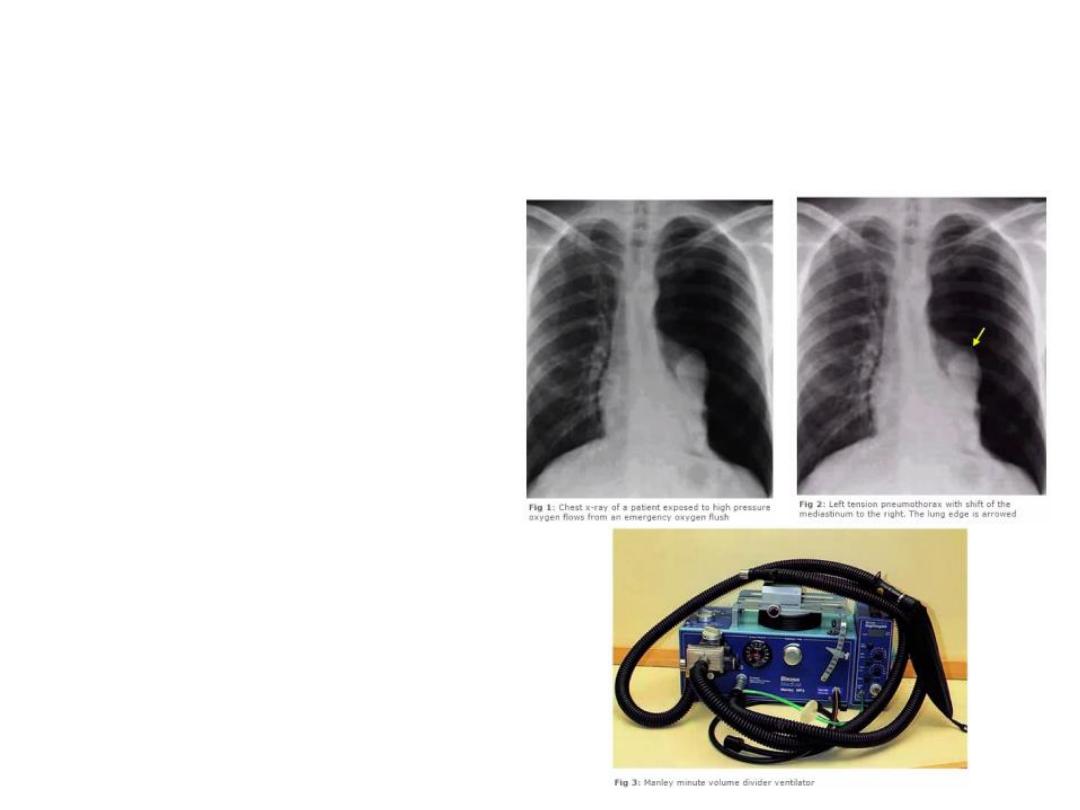
Oxygen flash
The risks to the patient of excessive
use of emergency oxygen flash:
• Put the patient at a higher risk of
barotrauma due to the high
operating pressure and flow of
the oxygen flash.
• Inappropriate use can lead to
dilution of anaesthetic gases and
possible awareness.
• Should not be activated while
using a minute volume divider
ventilator, a minute volume
divider ventilator delivers to the
patient the fresh gas flow from
the anaesthetic machine. It is
inappropriate to deliver flows in
excess of 35L/min.
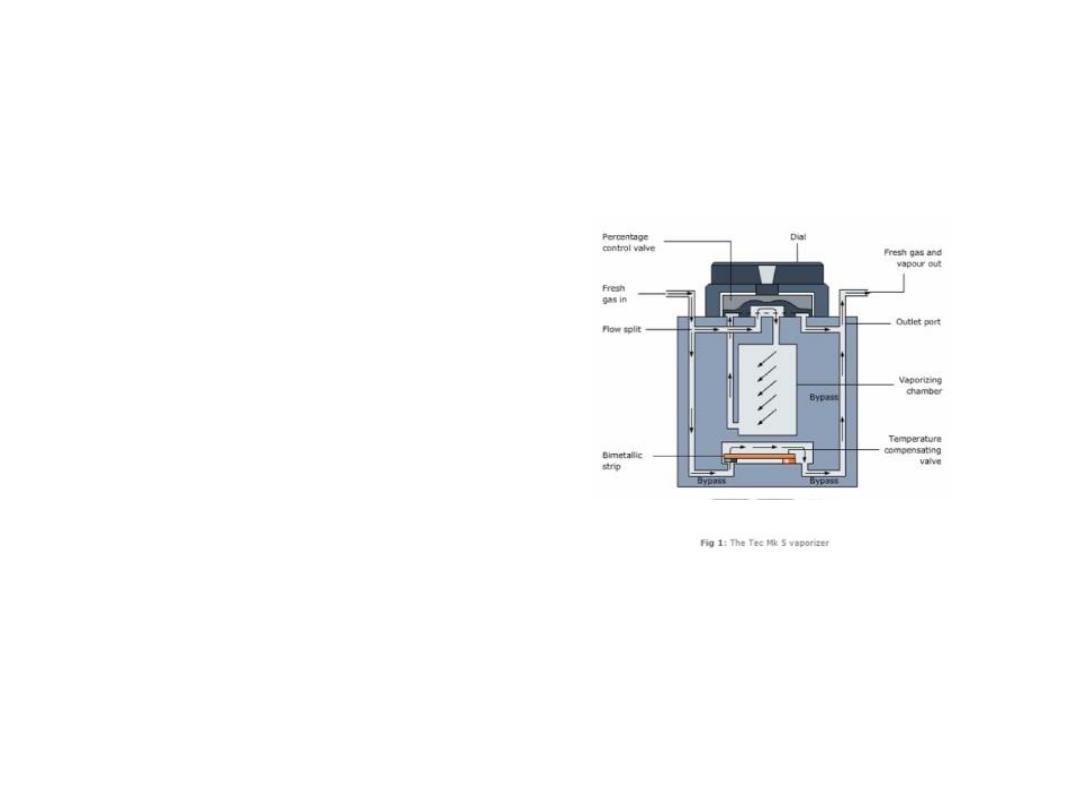
Vaporizers
anti – spill design
•
Vaporizers are filled with volatile agents.
They must always be kept upright as a
precaution against spillage. Tilting can result
in accidental delivery of dangerously high
concentrations of anaesthetic vapor. With
early vaporizer designs, critical accident
would occur when the vaporizer was
inadvertently tipped upside down, causing
the liquid anaesthetic agent to enter the
bypass channel.
•
Modern vaporizers, such as Tec MK 5, are
designed to reduce the risk of the agent
spilling into the bypass channel.
•
IN spite of this, it is recommended that the
vaporizer is purged with a fresh gas flow of
5L/min for 30 min, with percentage dial set
at 5% in case of accidental tilting.
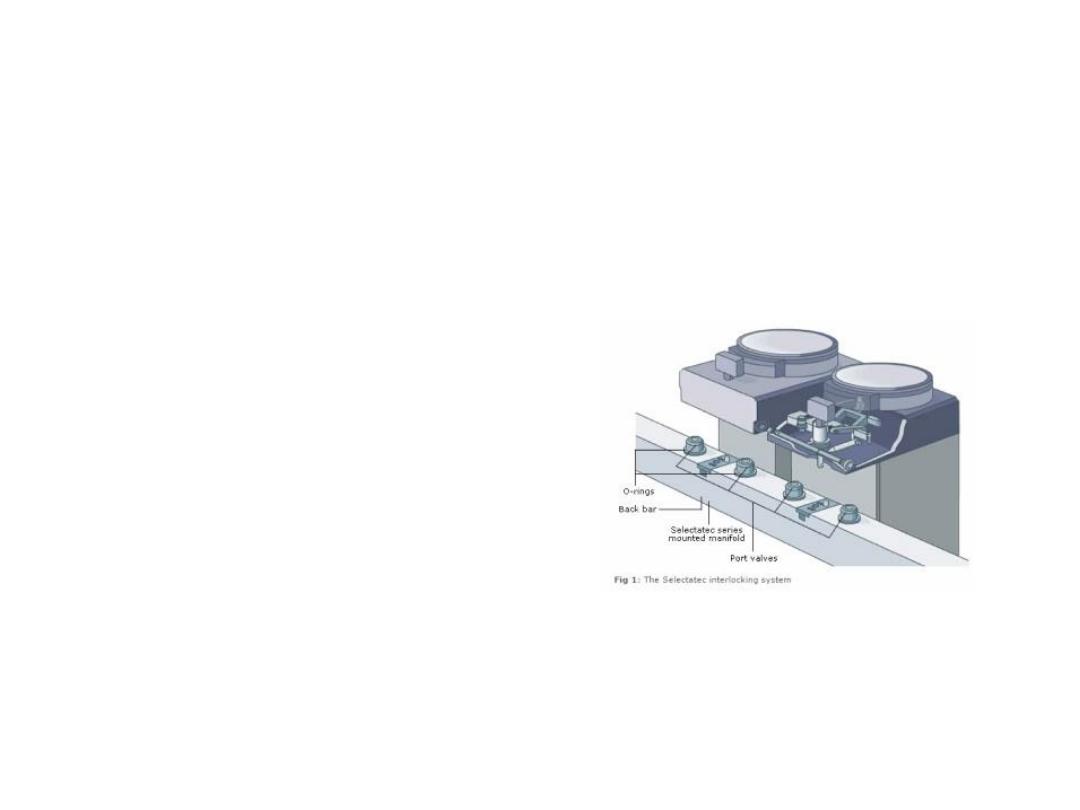
Vaporizers
the risk of leaks
The commonest causes of leaks
due to vaporizers are:
1. Incorrectly engaged
vaporizers on the back bar
2. Loss of one of the O – rings
on the mounts where the
vaporizer is positioned. As the
vaporizers are changed, the O –
rings can accidently adhere to the
vaporizer, so causing a leak when
another vaporizer is positioned.
a leak can lead to a delivery of
incorrect proportions of
anaesthetic gases.

Vaporizers maintenance
As vaporizers are used to deliver the
vapor of the volatile agents, it is
important to make sure that:
1. The vaporizing chambers are
adequately filled and that the filling
port(S) is/are tightly closed.
2. The vaporizers are correctly fitted
with a fully engaged back bar locking
mechanism.
3. The control knobs rotate fully
throughout their full range.
•
The consequences of any leakage of
volatile agents can be serious. It is
therefore essential that a leak test is
carried out whenever a vaporizer is
used or changed.

Leak testing
To test for leak:
1. Turn off the vaporizers
2. Set a flow of oxygen of 5L/min
3. Temporarily occlude the
common gas outlet of the
anaesthetic machine
4. Check for leak
5. There is no leak if the flow
meter bobbin (if present) dips
6. turn on the vaporizer and repeat
this test
7. There should be no leak of liquid
from the filling port
8. After testing, ensure that the
vaporizers and flowmeters are
turned off.
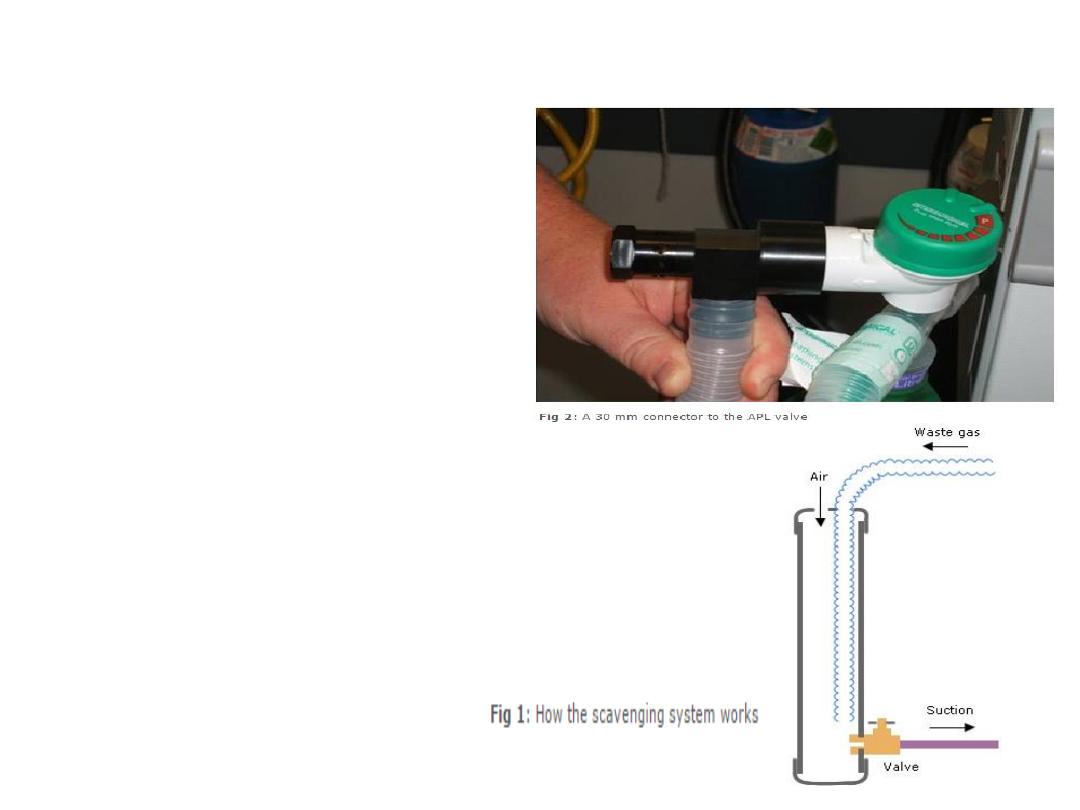
Scavenging
•
In order to reduce the risk of
pollution in the operating theatre,
the scavenging system, should be
used to ensure safe disposal of
anaesthetic waste gases.
•
So, ensure that it is switched on and
functioning. You should be able to
hear and feel the suction of the
disposal system.
•
The collecting and transfer
component of the scavenging system
should be attached to the
appropriate exhaust port of the
breathing system, ventilator or
anaesthetic workstation. A 30 mm
connector is used as a safety measure
in order to prevent accidental
misconnection to other ports of the
breathing system.

Suction equipment
Functioning suction equipment is essential for
safe conduct of anaesthesia. This allows
secretions or vomitus to be suctioned away from
the upper airway.
To test the suction system:
1.
Ensure that the vacuum probe is firmly
engaged with its outlet and that all
connection are secure
2.
Switch on the suction and occlude the
suction tubing. This is to test for the rapid
development of an adequate negative
pressure
3.
A suction unit should take no longer than
10S to generate a vacuum of 500mmHg
with a displacement of air of 25L/min
Ensure that the patient trolley, bed or operating
table can be tilted head – down rapidly.

Ancillary equipment
Airway management
equipment should be checked
next to ensure that each item
of ancillary equipment
required is available and
functioning correctly.
Ancillary equipment include:
1. Laryngoscopes
2. Intubation aids
3. Face masks, laryngeal
masks, airways, tracheal
tubes and connectors
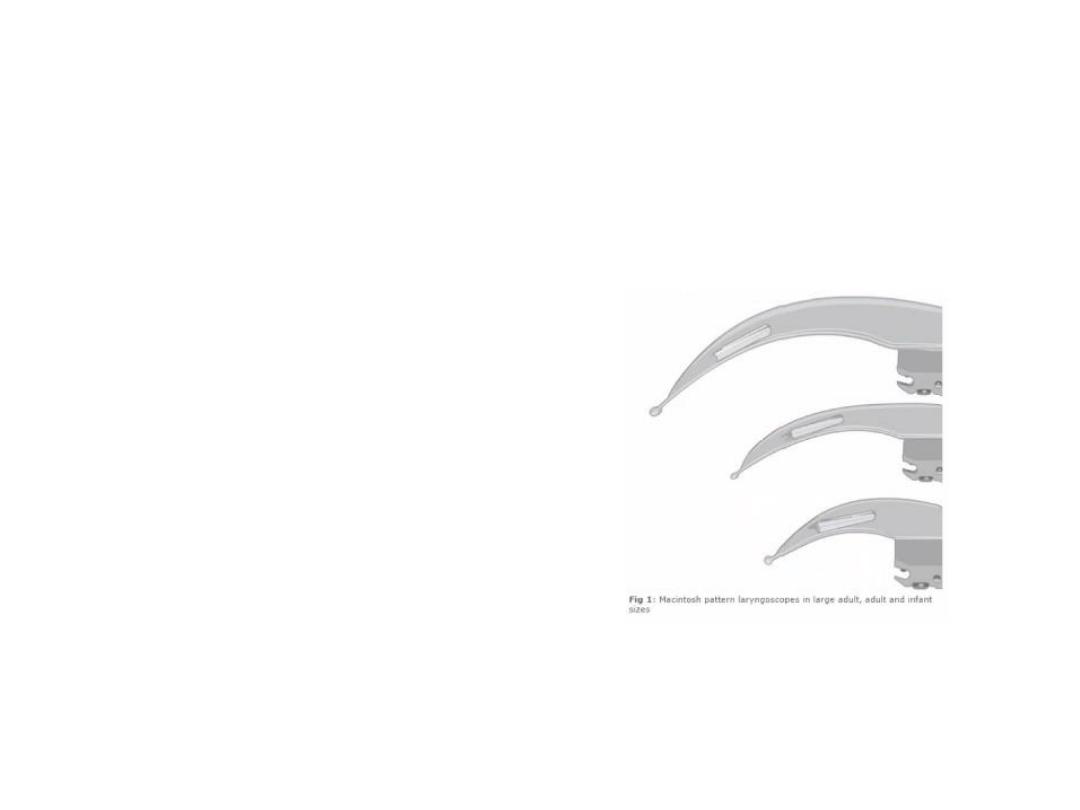
laryngoscopes
• Laryngoscopes should
be available in different
sizes. The bulbs must be
checked to ensure their
function.

Intubation aids
Several types of intubation aids may be
required: intubation forceps, bougies, stylets,
Magill forceps, etc.
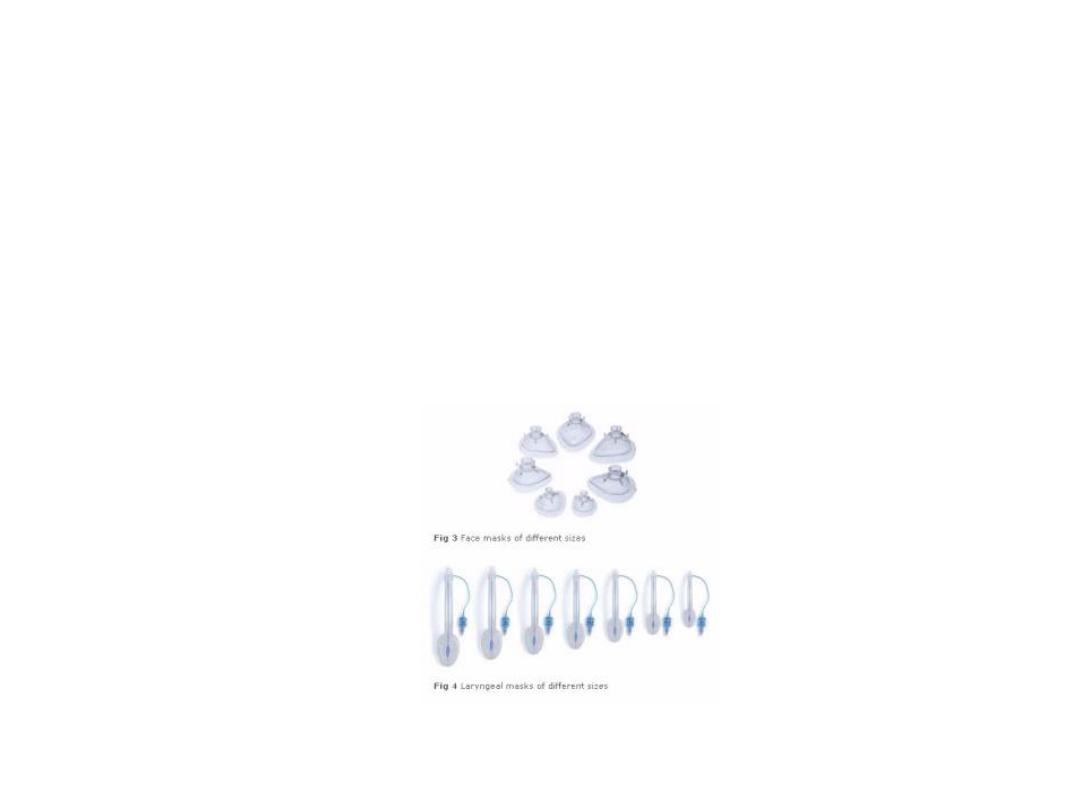
Airways equipment
Make sure that all face masks, laryngeal masks,
airways, tracheal tubes and connectors are
patent.
Single use device
In order to reduce the risk of cross - infection between patients, it is recommended that single
– use equipment is used when possible.
Single – use equipment will be marked with the symbol:
It is recommended that when single – use equipment is used, the packing should not be removed
until the point of use. This helps in infection control, identification and safety.
It must be emphasized that any equipment any equipment that is designated single - use must
be used for one patient only, and not re – used.

Back-Up Systems
Some modern anaesthetic machines may default to little or no flow in the event of failure.
In such situations, it is essential that an alternative oxygen supply and means of ventilation,
such as a self-inflating bag, circuit and oxygen cylinder, must be available, and checked as
functioning correctly with an adequate supply of oxygen.
Alternative methods of maintaining anaesthesia in this situation should be available such as
syringe pumps to administer total intravenous anaesthesia.
Record Keeping
Each anaesthetic machine should have a log
book in which check records are documented.
The following checks should be accurately and
systematically recorded:
1.
Regular servicing of anaesthetic machine
2.
Weekly oxygen failure alarm checks
3.
Daily pre – session checks
The anaesthetist should clearly document in the
patients anaesthetic record that:
1.
The anaesthetic machine check has been
performed
2.
Appropriate monitoring is in place and
functional
3.
The integrity, patency and safety of the
whole breathing system has been assured
Such documentation of the routine checking and
regular servicing of anaesthetic machines, and
patient breathing systems should be sufficient to
permit routine auditing to be carried out a future
time.

Session key points
•
Routine checking of equipment is essential in the safe delivery of anaesthetic care
•
Ensure that you have turned on anaesthetic machine after connecting it to the
mains supply
•
Check the gas supply; both piped gases and cylinders
•
Make sure that the monitoring equipment is working adequately
•
Ensure that various components of the anaesthetic machine are functioning
correctly – flowmeters, vaporizers, oxygen emergency flash, scavenging system
and suction system. Also check for leaks
•
Check the breathing system and its components
•
Ensure the availability of different airway management devices
•
When possible, use single – use devices
•
In cases of anaesthetic machine failure, have available means of ventilation and
administration of oxygen
•

Session summary
Learning objectives:
. Describe the tests performed in checking the
anaesthetic equipment
. Identify potential equipment malfunctions in
anaesthetic practice
. Recognize the design modifications of modern
anaesthetic equipment to prevent such
malfunction