
Medicine – Questions
GIT
Q1: what are the causes of acute pancreatitis?
A. Common (90% of cases):
1. Gallstones.
2. Idiopathic.
3. Alcohol.
4. Post-ERCP.
B. Rare:
1. Post-surgical (abdominal, cardiopulmonary bypass).
2. Trauma.
3. Drugs (azathioprine/mercaptopurine, thiazide diuretics, sodium valproate).
4. Metabolic (hypercalcaemia, hypertriglyceridaemia).
5. Pancreas divisum (p. 894).
6. Sphincter of Oddi dysfunction.
7. Infection (mumps, Coxsackie virus).
8. Hereditary.
9. Renal failure.
10.Organ transplantation (kidney, liver).
11.Severe hypothermia.
12.Petrochemical exposure.
Q2: What are the poor prognostic factors of pancreatitis?
Glasgow criteria for prognosis in acute pancreatitis*
- Age > 55 yrs.
- PO2 < 8 kPa (60 mmHg).
- White blood cell count (WBC) > 15 x 109/L.
- Albumin < 32 g.lL (3.2 g’dL).
- Serum calcium < 2 mmoUL (8 mg/dL) (corrected).
- Glucose > 10 mmol/L (180 mg/dL).
- Urea > 16 mmoL’L (45 mg’dL) (after rehydration).
- Alanine aminotransferase (ALT) > 200 U/L.
- Lactate dehydrogenase (LDH) > 600 U/L.
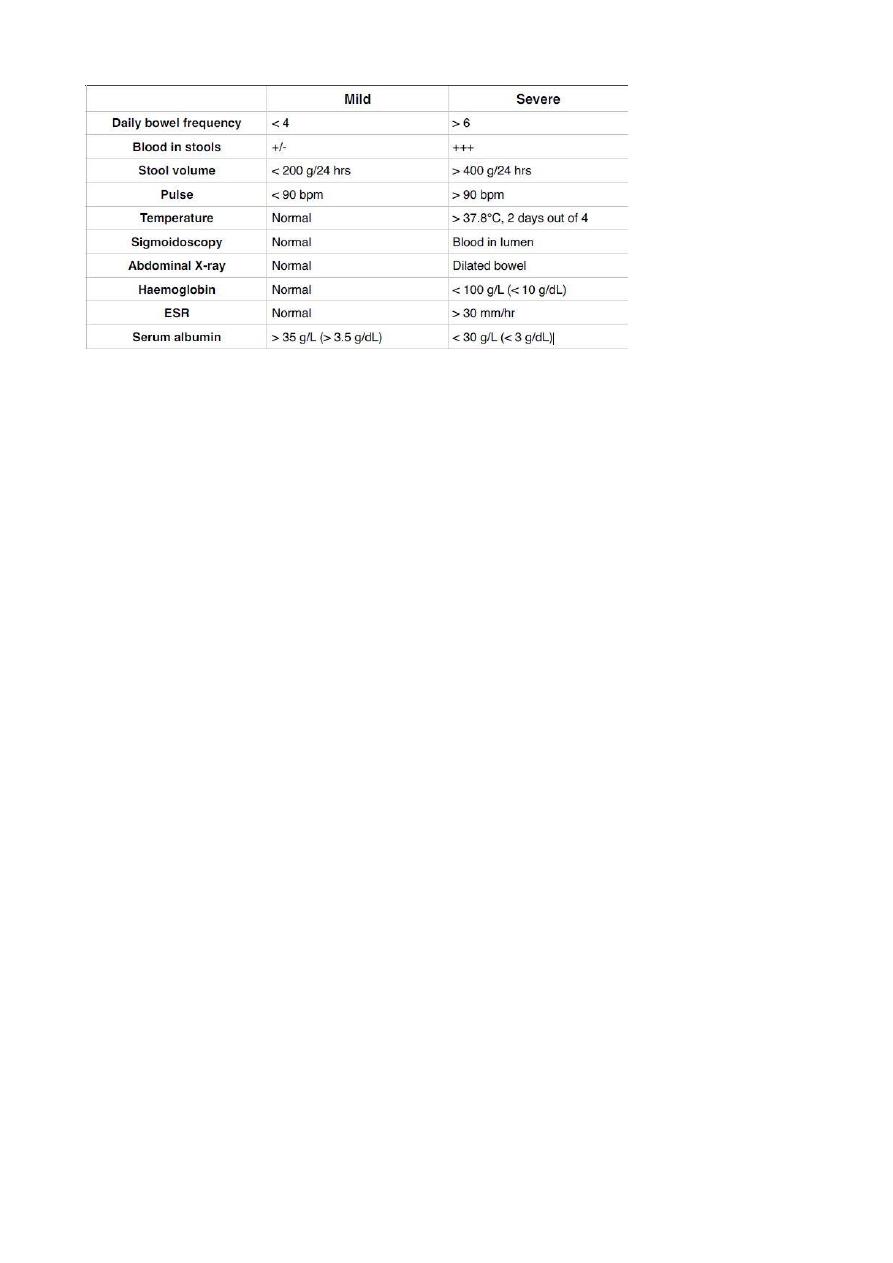
Q3: How you can assess the severity of inflammatory bowel disease?
Q4: What are the investigations done in malabsorption diseases?
- duodenal or jejinal biopsy
- antibodies screening: antigliadin, anti-endomysial antibodies
- hematological and biochemistery
- barium follow through
Q5: What is the management of ascites?
1. Sodium and water restriction; Restriction of sodium intake to 100 mmol/day (‘no
added salt diet’) is usually adequate. Drugs containing large amounts of sodium, and
those promoting sodium retention such as non-steroidal anti-inflammatory drugs
(NSAIDs), must be avoided.
2. Diuretic drugs; Spironolactone (100-400 mg/day) is the drug of choice. Some also
require powerful loop diuretics, e.g. furosemide. Patients who do not respond to
doses of 400 mg spironolactone and 160 mg furosemide are considered to have
refractory ascites.
3. Paracentesis; 3-5 litres daily is safe, provided the circulation is supported by giving
intravenous colloid such as human albumin (6-8 g per litre of ascites removed) or
another plasma expander.
4. Peritoneo-venous (LeVeen) shunt; Is a long tube with a non-return valve running
subcutaneously from the peritoneum to the internal jugular vein in the neck, which
allows ascitic fluid to pass directly into the systemic circulation.
5. Transjugular intrahepatic portosystemic stent shunt (TIPSS)
Q6: Write about management of upper GI bleeding:
A. Intravenous access;
B. Initial clinical assessment;
C. Blood tests;
D. Resuscitation;
E. Oxygen;
F. Endoscopy;
G. Monitoring;
H. Surgical operation;
Q7: What are the clinical features of malabsorption?
typical features: steatorrhea, abdominal distention, weight loss, delayed growth
atypical features: tiredness, folate, IDA, oral ulcers
extra-intestinal features: depression, arthralgia, osteoporosis, osteomalasia
association: type 1 DM, autoimmune thyroid diseases, dermatitis herpetiforms
Q8: Write about investigations and management of peptic ulcer:
Investigations:
1. Endoscopy: is the preferred investigation. Gastric ulcers must always be biopsied.
2. Barium studies: DU appears as a well-demarcated crater, most often seen in the
bulb. Benign GU also appears as a discrete crater with radiating mucosal folds
originating from the ulcer margin. Ulcers >3 cm in size or associ. with a mass are
more often malignant.
3. Tests for Detection of H. pylori infection (Serology, Urea breath tests, Faecal antigen test,
Histology, Rapid urease tests, Microbiological culture)
Management:
• First-line therapy is a proton pump inhibitor (12-hourly), clarithromycin 500 mg 12-
hourly, and amoxicillin 1 g 12-hourly or metronidazole 400 mg 12-hourly, for 10 days.
• Second-line therapy is a proton pump inhibitor (12-hourly), bismuth 120 mg 6-hourly,
metronidazole 400 mg 12-hourly, and tetracycline 500 mg 6-hourly, for 10 days.
• General measures; Cigarette smoking, aspirin and NSAIDs should be avoided
• Short-term management; after H pylori eradication ,followed by continuous acid
suppre. drugs ( H2 RB or PPI) for 4-6 wks.
• Maintenance treatment; GU need 8-12 wks to complete healing, with repeated
endoscopy and biopsy.
• Surgical treatment;
- Emergency; Perforation, Haemorrhage.
- Elective; Complications, e.g. gastric outflow obstruction. Recurrent ulcer following
gastric surgery.
Q9: How to manage cirrhosis?
• Treatment of any known cause.
• The maintenance of nutrition.
• Treatment of the complications of cirrhosis.
• Liver transplantation
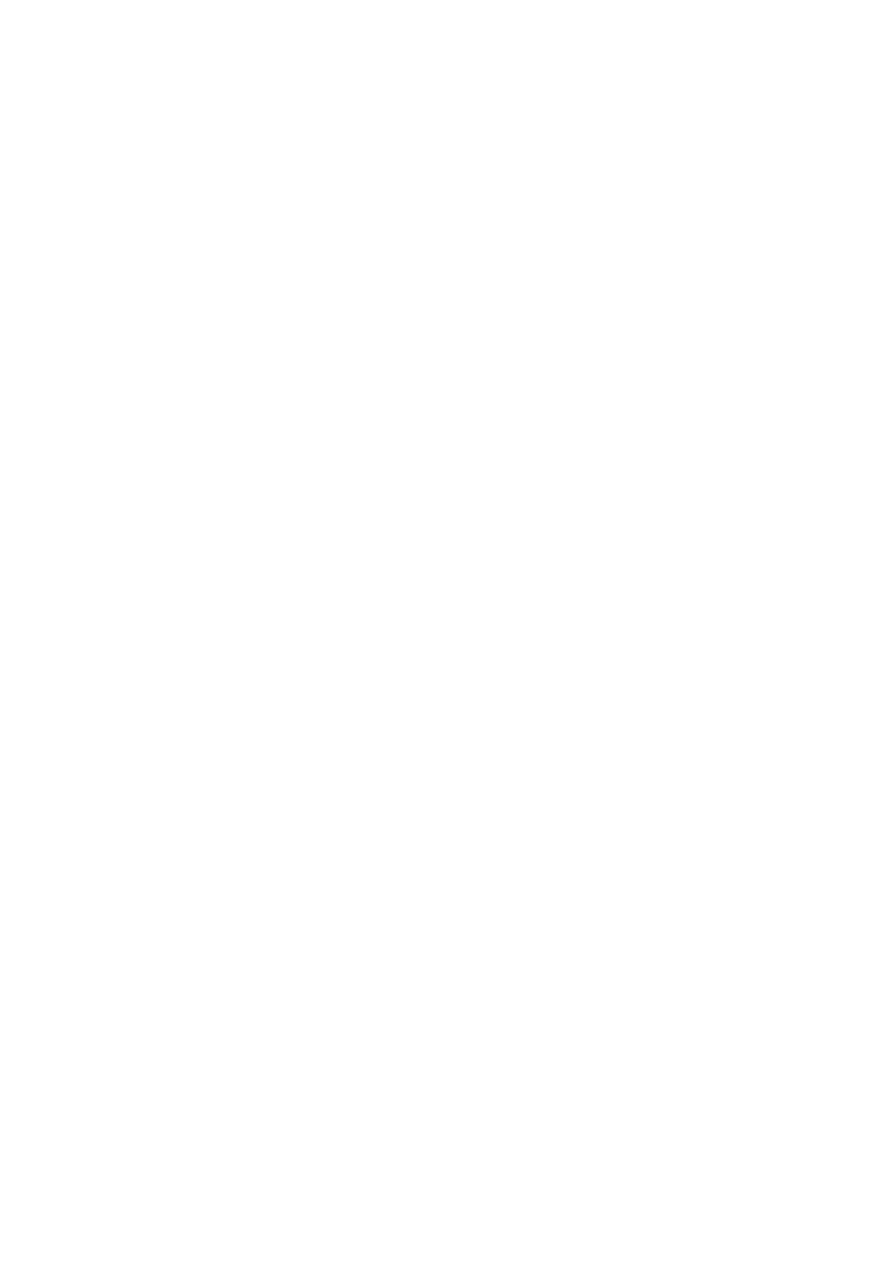
Q10: What are the extra-intestinal features of inflammatory bowel syndrome?
Q11: What are the complications of acute hepatitis?
1. Cholestatic hepatitis.
2. Acute liver failure.
3. Chronic hepatitis.
4. Aplastic anemia.
5. Relapsing hepatitis.
Renal
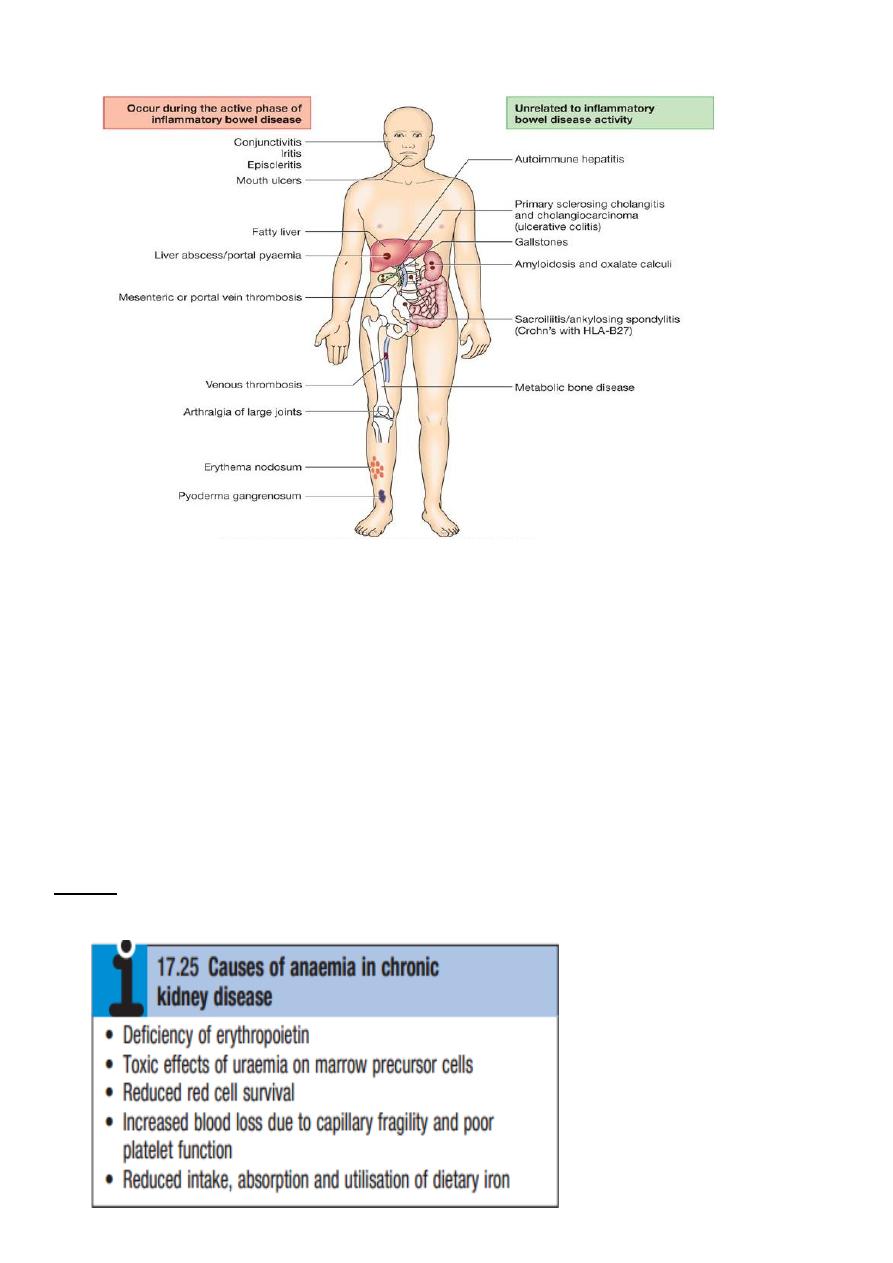
Q1: What are the causes of anemia in chronic renal failure?
Q2: Write about CVS involvement in chronic renal failure:
The risk of cardiovascular disease is substantially increased in patients with CKD stage 3 or
worse (GFR <60 mL/min/1.73 m2) and those with proteinuria or microalbuminuria.
Q3: How to manage chronic renal failure?
1-Antihypertensive therapy: Various targets have been suggested, such as 130/80 mmHg
for uncomplicated CKD, and 25/75 mmHg for CKD complicated by significant proteinuria of
more than 1 g/day (PCR >100 mg/mmol or ACR >70 mg/mmol).
2-Reduction of proteinuria: Angiotensinconverting enzyme (ACE) inhibitors and angiotensin
II receptor blockers (ARBs) reduce proteinuria and retard the progression of CKD .
3-Dietary and lifestyle interventions : All patients with stage 4 and 5 CKD should be given
dietetic advice aimed at preventing excessive consumption of protein, ensuring adequate
calorific intake and limiting potas sium and phosphate intake. Severe protein restriction is
not recommended. All patients should be advised to stop smoking. Exercise and weight loss
may also reduce proteinuria and have beneficial effects on cardiovascular risk profile.
4-Lipid-lowering therapy
5-Treatment of anaemia
6-Maintaining fluid and electrolyte balance
7-Renal bone disease
Q4: What are the indications of dialysis?
1- metabolic acidosis not response to treatment
2- pulmonary edema or hypertension not response to treatment
3- neurological symptoms
4- blood urea (100-150) or raid increase in blood urea
5- hypokalemia with hypokalemic tetany
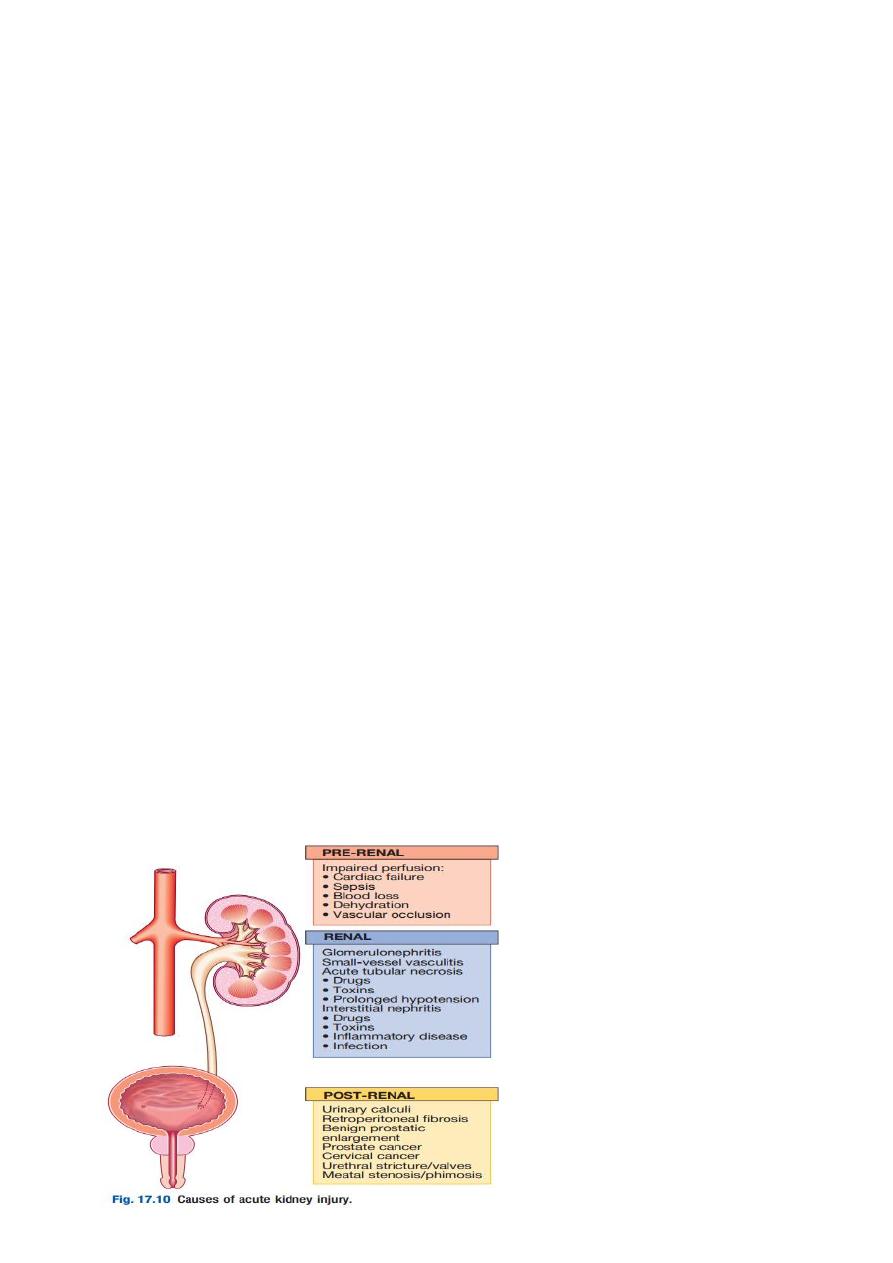
Q5: What are the pre-renal causes of acute renal failure?

Q6: What are the clinical features of nephrotic syndrome? and how to manage it?
1-proteinuria of 3.5 g per 1.73 m2 per 24 h (in practice, 3.0 to 3.5 g per 24 h),
2-hypoalbuminemia,
3-edema
4-hyperlipidemia,
5-lipiduria
6-hypercoagulability
The treatment of nephrotic syndrome involves :
(1) specific treatment of the underlying morphologic entity and, when possible, causative
disease;
(2) general measures to control proteinuria if remission is not achieved through
immunosuppressive therapy and other specific
measures;
(3) general measures to control nephrotic complications.
Q7: How to manage diabetic nephropathy?
Therapy is aimed at retarding the progression of nephropathy through control of blood
sugar, systemic blood pressure, and glomerular capillary pressure. Glycemic control is
achieved through regulation of diet and administration of oral hypoglycemic agents and
insulin. ACE inhibitors and ARBs are the drugs of choice as they control both systemic
hypertension and intraglomerular hypertension
Diabetic nephropathy is the most common cause of ESRD requiring renal replacement
therapy.
Renal transplantation, with or without pancreas transplantation, is the preferred mode of
renal replacement therapy in patients who are otherwise medically suitable.
Q8: Which glomerular diseases associated with low serum complements?
1-Post-infection glomerulonephritis
2-Subacute bacterial infection-especially endocarditis
3-SLE
4-Cryoglobulinaemia
5-Mesangiocapillary glomerulonephritis-usually type II.
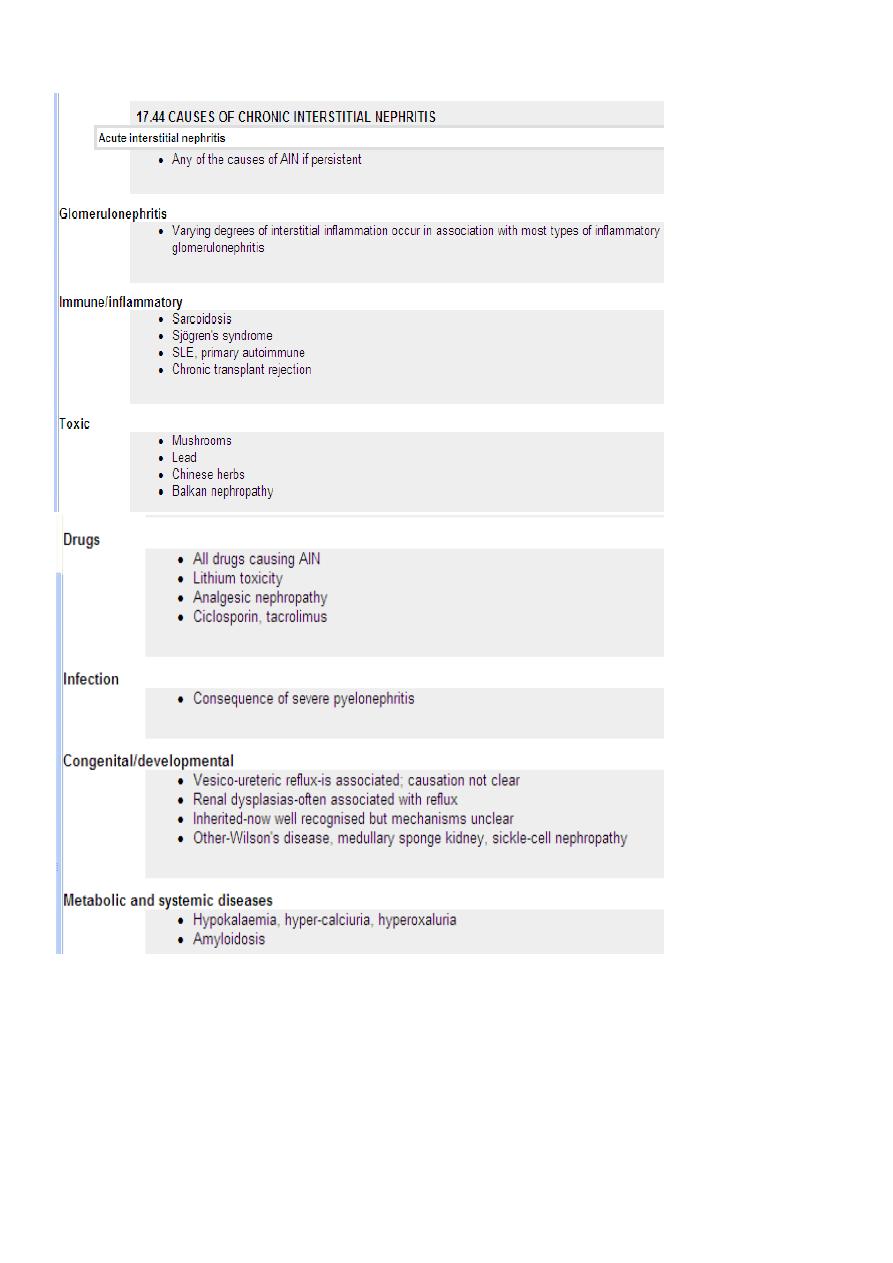
Q9: What are the causes of chronic intestinal nephritis?
CNS
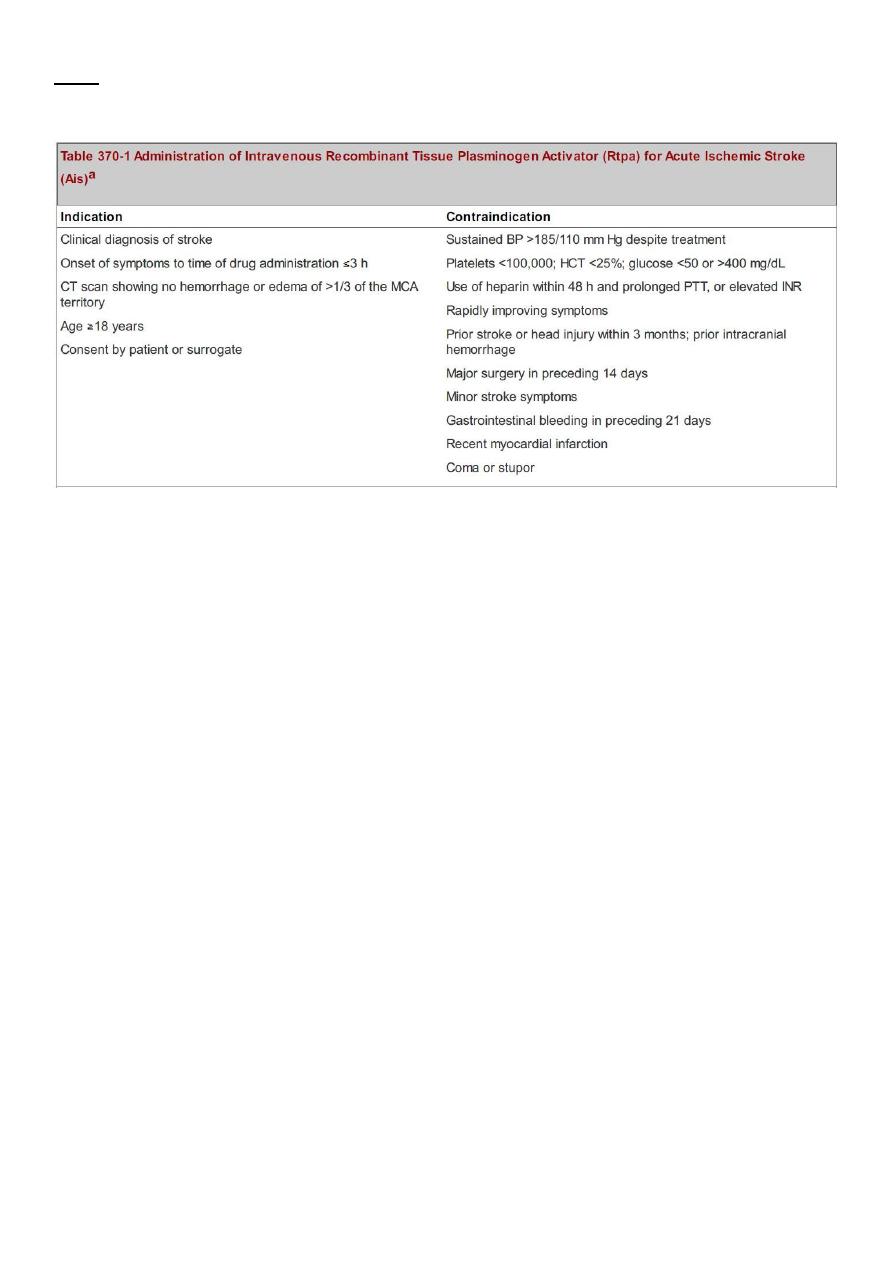
Q1: Write short note about the contraindications of thrombolysis in CVA:
Q2: What are the complications of meningitis?
-moderate or severe occurs in 25% of patient.
-decrease intellectual function.
-memory disorders.
-seizure.
-cranial N. palsy.
-hemiparesis & hemisonsory loss.
-dizziness & vertigo.
-hydrocephalus.
-cerebellar ataxia.
Urine disorders.
Q3: What are the prognostic factors of acute meningitis?
-decrease level of consciousness on admission.
-Seizures within 24 h.
-sings of increase ICP.
-extreme age.
-comorbid condition.
-delay in the initiated of treatment.
-decrease CSF glucose <40 & increase protein >3g.
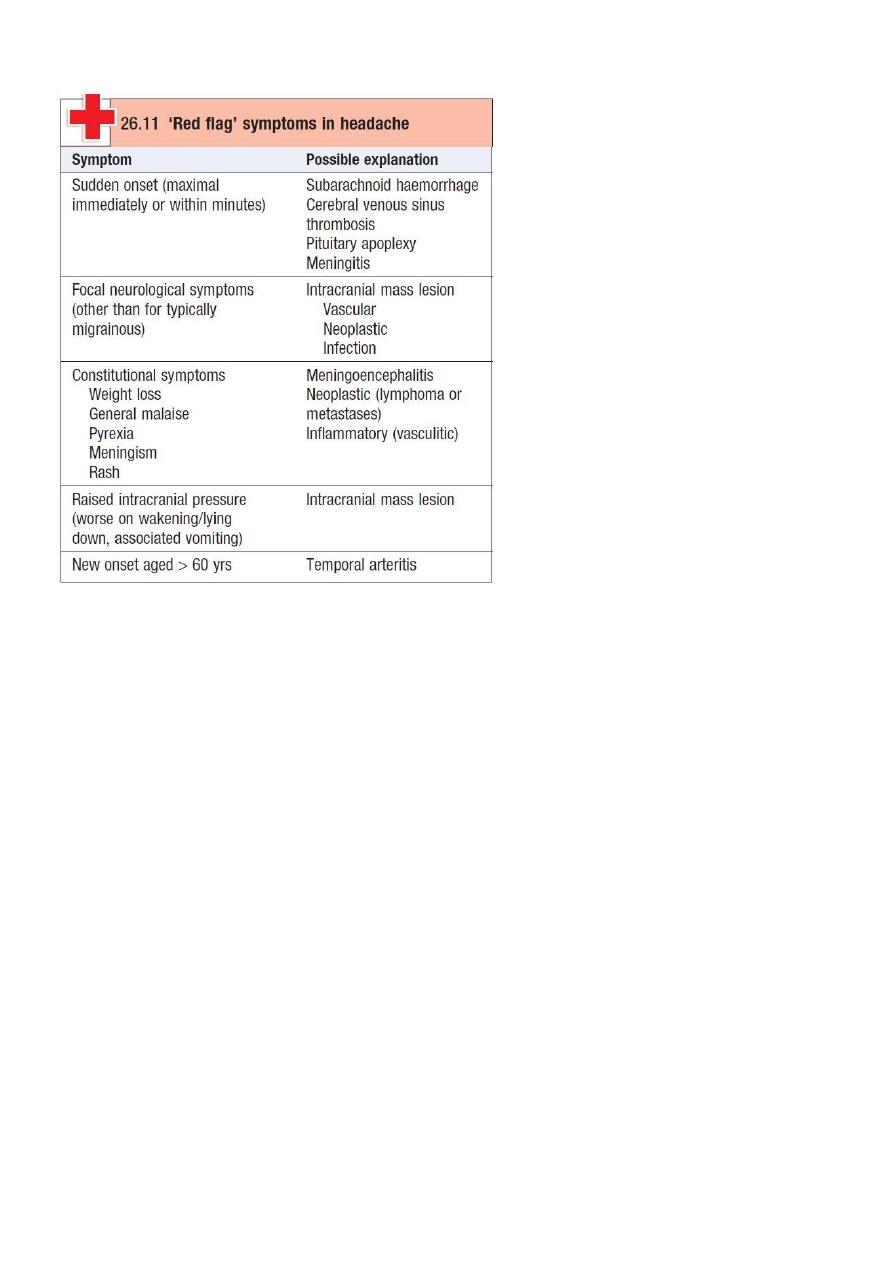
Q4: What are the alarming features of headache?
Q5: Write about drugs used in migraine:
Drugs for treatment:
1-rest in dark and quite room
2- simple analgesic (paracetamol, aspirin, NSAID)
3- ergotamine
4- sumatrptan
Prophylactic treatment:
1-Amitriptyline
2- Beta blockers (atenolol)
3- Serotonin inhibitors
4- cyproheptidine
5- methysergide
6- calcium antagonist (verapamil)
Q6: What are the features of PICA syndrome?
epsilateral cerebellar ataxia. - horner syndrome. - facial sensory loss.
nausea & vomiting. - nystagmus - vertigo.
contralateral loss pain &tempru.
dysphasia & dysartheria
excessive salivation .
Q7: How to manage SAH?
Early aneurysm repair prevent rerupture.
protecting the airway.
managing BP.
treat vasospasm.
decrease raised ICP.
bed rest in quiet room & given stool softeners.
treat seizures.
managing hyponatremia.
prevent of complication.
neurosurgical consultation.
Q8: Give the CSF findings of each type of meningitis, with management:
CSF findings
Viral meningitis
TB meningitis
Bacterial meningitis
Glucose
Normal
Low
Normal or marked
decrease
Protein
Moderate increase Moderate to marked
increase
Marked increase
WBC
< 100 cell/ul
10 – 1000 cell/ul
> 500 cell/ul
Cell differential Neutrophils and
lymphocyte
lymphocyte
Neutrophils
Pressure
Normal
variable
Elevated
Culture
negative
Positive for AFB
positive
= Treatment of bacterial meningitis:
-the goal to start Abs. therapy within 60 min. of arrival emergency room.
-Adjuctive therapy:
1- dexamethasone .
2-treat raised ICP.
= Treatment of viral meningitis
-symptomatic T.
-oral or I.V. acyclovir.
= Treatment of TB meningitis
1- combination of antibiotics.
2-steriod.
Q9: Write about clinical features and management of encephalitis:
Clinical features:
-in addition to acute febrile illness with meningitis, patient commonly has confusion,
behavioral abnormalities.
-altered level of consciousness. -seizures.
-focal neurological deficits. -cranial N. palsy.
-involuntary movement. -psychological disorders.
-hypothalamus-pituitary lesion.
Management:
-specific antiviral therapy should be initiated when appropriate.
-monitoring of vital functions.
-treat raise ICP.
-treat seizure.
-prevent & treat of complication.
-antiviral therapy.
-acyclovir.
-ganciclovir & foscarnet.
Q10: Give types and movement disorder and causes of each:
1- Tremor:
anxiety or fear.
excessive physical activity.
sleep deprivation.
sedative drug or alcohol withdrawal.
drug toxicity ( lithium, bronchodilators, sodium valproate )
co poisoning.
thyrotoxicosis.
brainstem disorders.
cerebellar disorders.
drug toxicity ( alcohol, anticonvulsants, sedatives )
wilsons disease.
2- Choria
hereditary:
static encephalopathy:
sydenhams chorea.
chorea gravidarum.
drug toxicity:
medical disorders:
cerebrovascular disorders:
structural lesions of the subthalamic nucleus.
3-Hemiballismus
due to contralateral subthalamic nucleus
4-dystonia and athetosis
cerebral palsy.
wilsons disease.
huntingtons disease.
parkinsons disease.
drugs. Levodopa and antipsychotic.
toxins. Mathanol and manganes.
ischemic.
anoxia.
Progressive supranuclear palsy.
dpoa-responsive dystonia.
psychogenic.
5-Myoclonus
physiological:
nocturnal.
hiccup.
essential M.
epileptic M.
symptomatic myoclonous:
Q11: What are the causes, features, management of Guillian barre syndrome?
Causes:
autoimmune mechanism lead to idiopathic polyneuropathy
Features:
ascending paralysis – bulbar weakness – bilateral facial weakness – respiratory difficulty
sensory symptoms – autonomic impairment – history of fever or surgical procedure
Management:
plasmapharesis – respiratory care unit – symptomatic treatment – physiotherapy
Q11: How to manage patient with Parkinson?
Anticholinergic drugs (procyclidine)
amantadine
levodopa
bromocriptine
pregolide
selegiline
Endocrine
Q1: Write short note about management of Thyrotoxic crisis:
Patients should be rehydrated and given a broad-spectrum antibiotic. Propranolol is rapidly
effective orally (80 mg 6-hourly) or intravenously (1-5 mg 6-hourly). Sodium ipodate (500
mg per day orally) will restore serum T3 levels to normal in 48-72 hours. This is a
radiographic contrast medium which not only inhibits the release of thyroid hormones, but
also reduces the conversion of T3 to T4 and is, therefore, more effective than potassium
iodide or Lugol's solution. Dexamethasone (2 mg 6-hourly) and amiodarone have similar
effects. Oral carbimazole 40-60 mg daily inhibits the synthesis of new thyroid hormone. If
the patient is unconscious or uncooperative, carbimazole can be administered rectally with

good effect, but no preparation is available for parenteral use. After 10-14 days the patient
can usually be maintained on carbimazole alone.
Q2: What is the management of myxedema coma?
Myxoedema coma is a medical emergency and treatment must begin before biochemical
confirmation of the diagnosis. Thyroxine is not usually available for parenteral use so
triiodothyronine is given as an intravenous bolus of 20 μg followed by 20 μg 8-hourly until
there is sustained clinical improvement. In survivors there is a rise in body temperature
within 24 hours and, after 48-72 hours, it is usually possible to substitute oral thyroxine in a
dose of 50 μg per day. Unless it is apparent that the patient has primary hypothyroidism,
e.g. thyroidectomy scar or goitre, the thyroid failure should be assumed to be secondary to
hypothalamic or pituitary disease and treatment given with hydrocortisone 100 mg i.m. 8-
hourly, pending the results of T4, TSH and cortisol concentration. Other measures include
slow rewarming, cautious use of intravenous fluids, broad-spectrum antibiotics and high-
flow oxygen. Occasionally, assisted ventilation may be necessary.
Q3: What are the clinical features of Cushing syndrome?
• Fat redistribution (dorsocervical and supraclavicular fat pads, centripetal obesity, weight
gain)
• Menstrual irregularities
• Thin skin/plethora
• Moon facies
• Increased appetite
• Hypertension
• Altered mentation (poor concentration, decreased memory, euphoria)
• Diabetes mellitus/glucose intolerance, Striae , Hirsutism ,Proximal muscle weakness,
Psychological disturbances (emotional lability, depression, mania, psychosis), Decreased
libido/impotence.
• Acne , Osteoporosis/pathologic fractures , Virilization (in women), Easy bruisability, Poor
wound healing, Edema, Increased infections and Cataracts.
Q4: What are the clinical features of acute adrenal crisis? and how to manage it?
Circulatory shock with severe hypotension, Hyponatraemia, hyperkalaemia and, in some
instances, hypoglycaemia and hypercalcaemia, Muscle cramps, nausea, vomiting, diarrhoea
and unexplained fever may be present.
Management
1- Glucocorticoid replacement;
Cortisol (hydrocortisone) is the drug of choice, given by mouth, 15 mg on waking and 5 mg
at ∼1800 hrs.
An adrenal crisis; intravenous hydrocortisone succinate 100 mg and intravenous fluid
(normal saline and 10% dextrose for hypoglycaemia). Parenteral hydrocortisone should be

continued (100 mg I.M. 6-hourly) until gastrointestinal symptoms abate before starting oral
therapy.
2- Mineralocorticoid replacement;
fludrocortisone from being metabolised by 11β-HSD2 and thereby confers a longer half-life
and access to mineralocorticoid receptors. The usual dose is 0.05-0.1 mg daily
In adrenal crisis, however, rapid replacement of sodium deficiency is more important than
administration of fludrocortisone. Intravenous saline should be infused as required to
normalise haemodynamic indices
Q5: Write short note about features and management of DM?
SYMPTOMS OF HYPERGLYCAEMIA
• Thirst, dry mouth
• Polyuria
• Nocturia
• Tiredness, fatigue
• Recent change in weight
• Blurring of vision
• Pruritus vulvae, balanitis (genital candidiasis)
• Nausea, headache
• Hyperphagia; predilection for sweet foods
• Mood change, irritability, difficulty in concentrating, apathy
Management
1-Educating patients
2- oral hypoglycemic drugs
3- insulin
Q6: How to manage DKA?
1- Fluid replacement
2- Administration of short-acting (soluble) insulin
3- Potassium replacement
4- Bicarbonate
5- Administration of antibiotics if infection is present
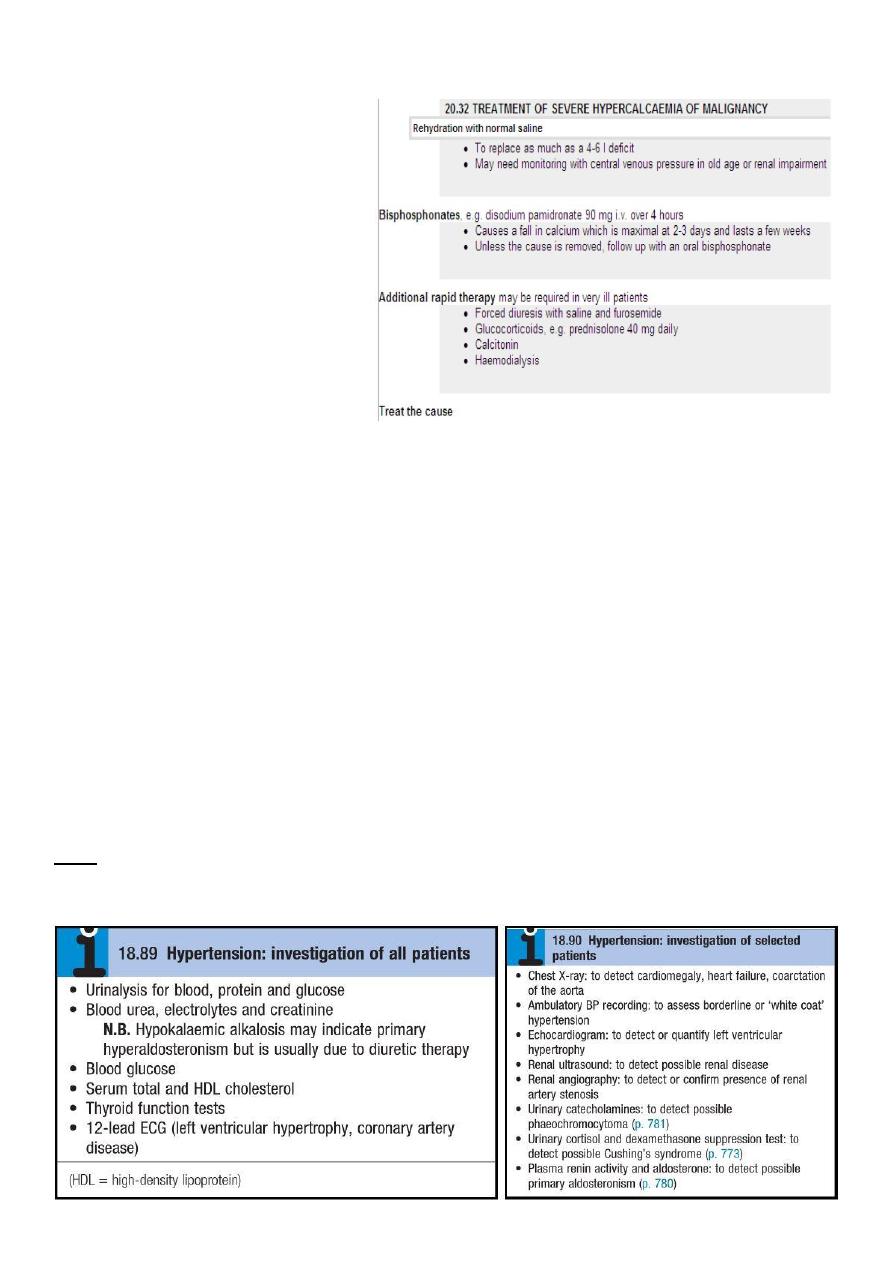
Q7: Write the management of hypocalcaemia and hypercalcaemia:
Management of hypercalcaemia
Management of hypocalcaemia
To control tetany, alkalosis can be reversed acutely if arterial PCO 2is increased by
rebreathing expired air in a paper bag or administering 5% CO 2in oxygen. Injection of 20 ml
of a 10% solution of calcium gluconate slowly into a vein will raise the serum calcium
concentration immediately. An intramuscular injection of 10 ml may also be given to obtain
a more prolonged effect. In severe cases of alkalotic tetany, intravenous calcium gluconate
often relieves the spasm, while specific treatment of the alkalosis, which will vary with the
cause, is being applied. Intravenous magnesium is required to correct the hypocalcaemia
associated with hypomagnesaemia.
Persistent hypoparathyroidism and pseudohypo-parathyroidism are treated with oral
calcium salts and vitamin D analogues, either 1α-hydroxycholecalciferol (alfacalcidol) or
1,25-dihydroxycholecalciferol (calcitriol). This therapy needs careful monitoring because of
the risks of iatrogenic hypercalcaemia, hypercalciuria and nephrocalcinosis.
CVS
Q1: What are the investigations you should do for hypertensive patient?
Q2: What are the drugs used in management of hypertension (with examples)?
1- Thiazide and other diuretics:
A daily dose of 2.5 mg bendroflumethiazide or 0.5 mg cyclopenthiazide is appropriate.
2- Beta-adrenoceptor antagonists (β-blockers):
Metoprolol (100-200 mg daily), atenolol (50-100 mg daily) and bisoprolol (5-10 mg
daily) are cardioselective.
3- Labetalol and carvedilol:
Labetalol (200 mg-2.4 g daily in divided doses) and carvedilol (6.25-25 mg 12-hourly)
4- Angiotensin-converting enzyme (ACE) inhibitors:
These drugs (e.g. enalapril 20 mg daily, ramipril 5-10 mg daily or lisinopril 10-40 mg
daily)
5- Angiotensin receptor blockers:
These drugs (e.g. losartan 50-100 mg daily, valsartan 40-160 mg daily)
6- Calcium antagonists:
The dihydropyridines (e.g. amlodipine 5-10 mg daily, nifedipine 30-90 mg daily) are
effective
7- Other drugs:
A variety of vasodilators are used to treat hypertension. These include the α-1
adrenoceptor antagonists (α-blockers), such as prazosin (0.5-20 mg daily in divided
doses), indoramin (25-100 mg 12-hourly) and doxazosin (1-16 mg daily), and drugs
that act directly on vascular smooth muscle, such as hydralazine (25-100 mg 12-
hourly) and minoxidil (10-50 mg daily). Side-effects include first-dose and postural
hypotension, headache, tachycardia and fluid retention. Minoxidil also causes
increased facial hair and is therefore unsuitable for female patients.
Centrally acting drugs, such as methyldopa (initial dose 250 mg 8-hourly) and
clonidine (0.05-0.1 mg 8-hourly), are effective antihypertensive drugs but cause
fatigue and are usually poorly tolerated.
Q3: How to approach to hypertensive patient?
APPROACH TO NEWLY DIAGNOSED HYPERTENSION:
• Hypertension occasionally causes headache but most patients remain asymptomatic.
Accordingly, the diagnosis is usually made at routine examination or when a
complication arises. A blood pressure check is advisable every 5 years in adults.
• The objectives of the initial evaluation of a patient with high blood pressure readings
are:
1. to obtain accurate and representative measurements of blood pressure.
2. to identify contributory factors and any underlying cause (secondary
hypertension).
3. to assess other risk factors and quantify cardiovascular risk.
4. to detect any complications (target organ damage) that are already present.
5. to identify comorbidity that may influence the choice of antihypertensive therapy.
Q4: Write about causes and management of atrial fibrillation:
Causes:
Congestive heart failure, Cardiomyopathy, Valvular disease, Cardiac surgery, Hypertension,
Myocardial infarction, Pericarditis, Coronary heart disease, Cardiac tumors, Atrial septal
defect, Mitral stenosis, Endocarditis, Alcohol intoxication or withdrawal, Drugs: cocaine.
amphetamines. catteine. theophylline, Pulmonary embolism, Hypoxia, Cerebrovascular
accident, Defibrillation, Electrolyte abnormalities, Trauma, Pneumonia, Sepsis,
Hyperthyroidism.
Management:
Rate control
Rhythm control
Cardioversion
Thrombolytics
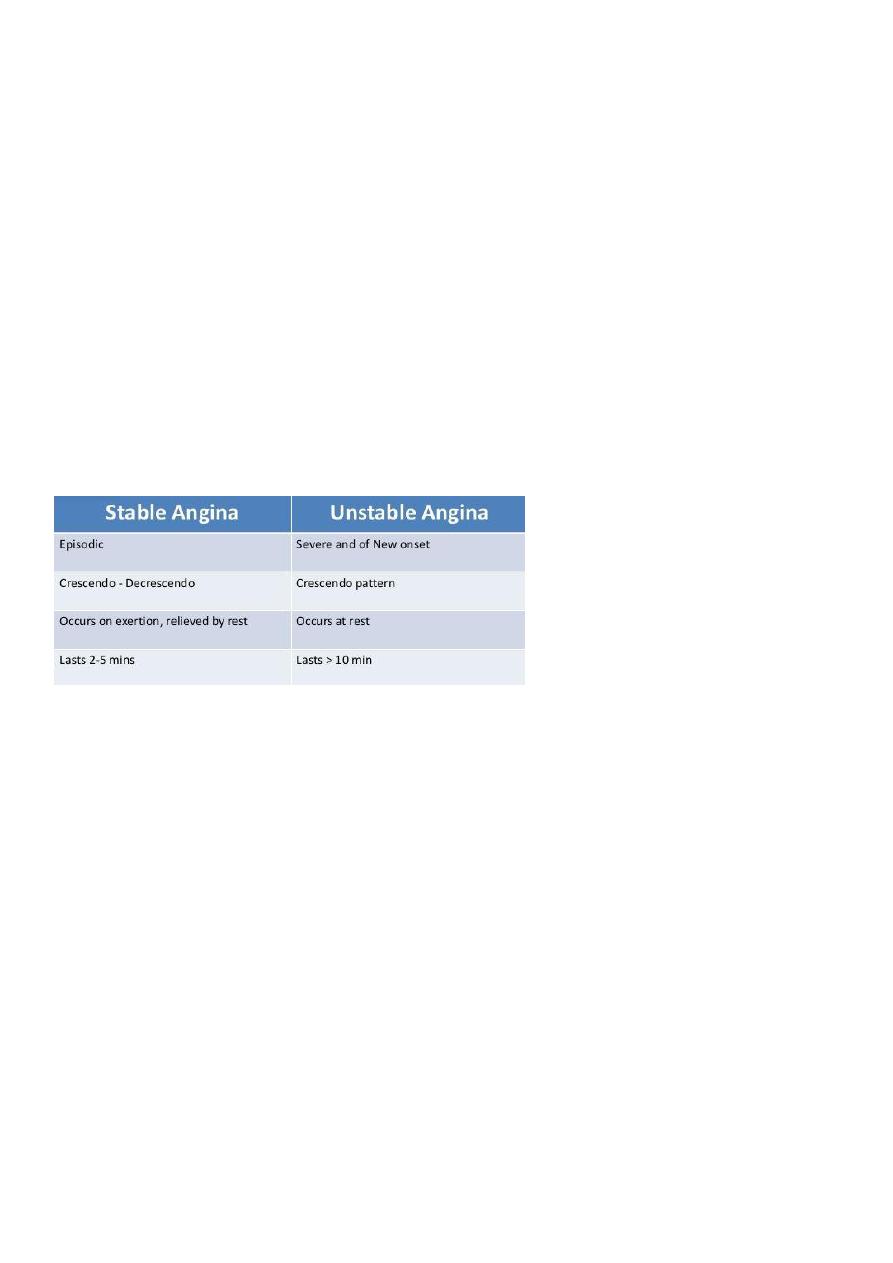
Q5: Compare between stable and unusable angina:
Q6: What are the immediate and late management of MI?
Early management:
• The patient’s history and 12-lead ECG are the primary methods used to determine
initially the diagnosis of MI.
• The ECG is examined for the presence of ST segment elevations of 1 mV or greater
in contiguous leads.
1. Administer aspirin, 160 to 325 mg chewed.
2. After recording the initial 12-lead ECG, place the patient on a cardiac monitor
and obtain serial ECGs.
3. Give oxygen by nasal cannula.
4. Administer sublingual nitroglycerin (unless the systolic blood pressure is less
than 90 mm Hg or the heart rate is less than 50 or greater than 100 beats/
minute).
5. Provide adequate analgesia with morphine sulfate. Provide adequate analgesia
with morphine sulfate.
Late management:
Thrombolytic Therapy:
Primary Percutaneous Transluminal Coronary Angioplasty (PTCA):

Intensive and intermediate care management:
• Prophylactic antidysrhythmics during the first 24 hours of hospitalization are not
recommended.
• IV nitroglycerin is continued for 24 to 48 hours.
• Daily aspirin is continued on an indefinite basis.
• Clopidogrel: IV beta blocker therapy should be administered within the initial hours
of the evolving infarction, followed by oral therapy provided there are no
contraindications.
• Beta blockers are one of the few pharmacological agents.
• That have been shown to reduce morbidity and mortality in the patient with an MI.
• They reduce oxygen demand by decreasing the heart rate and contractility.
• They also increase coronary artery filling by prolonging diastole.
• Calcium channel blockers may be given to patients in whom beta blocker therapy is
ineffective or contraindicated.
• Angiotensin-converting enzyme (ACE) inhibitors are administered to patients with
anterior wall MI and to patients who have an MI with heart failure in the absence of
significant hypotension.
• ACE inhibitors help prevent ventricular remodeling (dilation) and preserve ejection
fraction.
• Heparin is given to patients undergoing percutaneous or surgical revascularization
and for those receiving thrombolytic therapy with alteplase.
• Low–molecular-weight heparin should be used for patients with non–Q-wave MI
Q7: What are the clinical features of aortic regurgitation?
Peripheral Signs:
1. Quincke’s sign: capillary pulsation in nail beds.
2. Corrigan’s sign: water hammer pulse Large-volume or 'collapsing' pulse.
3. Bisferiens pulse (AS/AR > AR).
4. De Musset’s sign: systolic head bobbing or Head nodding with pulse: de
Musset's sign
5. Mueller’s sign: systolic pulsation of uvula
6. Low diastolic and increased pulse pressure
7. Durosier’s sign: femoral retrograde bruits
8. Traube’s sign: pistol shot femorals
9. Hill’s sign: BP Lower extremity >BP Upper extremity by:
- > 20 mm Hg - mild AR.
- > 40 mm Hg – moderate AR.
- > 60 mm Hg – severe AR.
Q8: What are the clinical features of mitral stenosis?
• Palpation:
- Small volume pulse

- Tapping apex-palpable S1
- +/- palpable opening snap (OS)
- RV lift
- Palpable S2
• ECG:
- LAE, AFIB, RVH, RAD
• Auscultation:
- Loud S1- as loud as S2 in aortic area
- A2 to OS interval inversely proportional to severity
- Diastolic rumble: length proportional to severity
- In severe MS with low flow- S1, OS & rumble may be inaudible
Q9: What are the clinical features of infective endocarditis? how to manage it?
• Fever, chills, weakness, lethargy, weight loss, flu-like illness (not always present).
• Longstanding IE (rarely seen now with earlier diagnosis): splinter haemorrhages,
Janeway lesions, Osler nodes, Roth spots.
• Murmurs are present in 90% of patients with left sided IE.
• In IVDU right sided IE usually affect the tricuspid valve & occasionally the pulmonary
valve, instead of systemic issues pulmonary embolism is the most important
complication which can evolve into:
- Pulmonary infarction
- Pulmonary abscess
- Bilateral pneumothoraces
- Pleural effusion
- Empyema
• The severity of valvular destruction depends on virulence of infecting organism &
infection duration.
• Heart failure can be the initial presentation.
Management:
• Adjusted according to MCS.
• Vancomycin is used in pts with intracardiac prosthetic material or suspected MRSA.
• Benzylpenicillin is the first choice for Streptococcus or Enterococcus penicillinsusceptible
strains.
• For vanc-resistant MRSA: teicoplanin, lipopeptide daptomycin or oxazilidones
(linezolid) is recommended
• Antimicrobial therapy can only offer curative treatment in ~50%.
• The other 50% require surgery.
Q10: Write about etiology and management of acute pericarditis:
Etiology:
• Infectious:

- Viral.
- Bacterial.
- TB.
• Noninfectious:
- Post MI (acute and Dresslers).
- Uremia.
- Neoplastic disease.
- Post radiation.
- Drug-induced.
- Connective tissue diseases/autoimmune.
- Traumatic.
Treatment:
• ASA or NSAIDs.
- Avoid NSAID in MI.
• Colchicine.
• Steroids - avoid.
- May increase reoccurance.
• TB – Rx TB+steroids.
• Purulent – drainage of fluid + antibiotics.
• Neoplastic- drainage.
• Uremic - dialysis.
Respiratory
Q1: What are the indications for admitting TB patient to hospital?
Most patients can be treated at home. Admission to a hospital unit with appropriate
isolation facilities should be considered where there is uncertainty about the diagnosis,
intolerance of medication, questionable treatment adherence, adverse social
conditions or a sig-nificant risk of MDR-TB (culture-positive after 2 months on
treatment, or contact with known MDR-TB).
Q2: What are the indications for corticosteroids and surgery in TB?
• Corticosteroids reduce inflammation and limit tissue damage, and are currently
recommended when treating pericardial or meningeal disease, and in children with
endobronchial disease. They may confer benefit in TB of the ureter, pleural effusions
and extensive pulmonary disease, and can suppress hypersensitivity drug reac-tions.
• Surgery should be considered in cases compli-cated by massive haemoptysis,
loculated empyema, constrictive pericarditis, lymph node suppuration, and spinal disease
with cord compression, but usually only after a full course of antituberculosis
treatment.
Q3: What is the third step in the management of asthma?
Step 3: add – on therapy:
1. A further increase in the dose of inhaled CS may benefit some patients but in
general, add – on therapy should be considered beyond an inhaled CS dose
of 800 Mg/day BDP (or equivalent).
2. Long-acting B2- agonist, such as salmeterol and formoterol. (fixed
combination inhalers of ICS and LABAs have been developed).
3. Leukotriene receptor antagonists (e.g. Montelukast 10 mg daily).
4. Theophylline may useful.
Q4: What are the indications of corticosteroids in asthma?
1. Progressive worsening of symptoms and PEF day by day.
2. Fall of PEF below 60% of the patient personal best recording.
3. Onset or worsening of sleep disturbance by asthma.
4. Persistence of morning symptoms until midday.
5. Progressively diminishing response to an inhaled bronchodilator.
6. Symptoms sever enough to require treatment with nebulised or injected
bronchodilator.
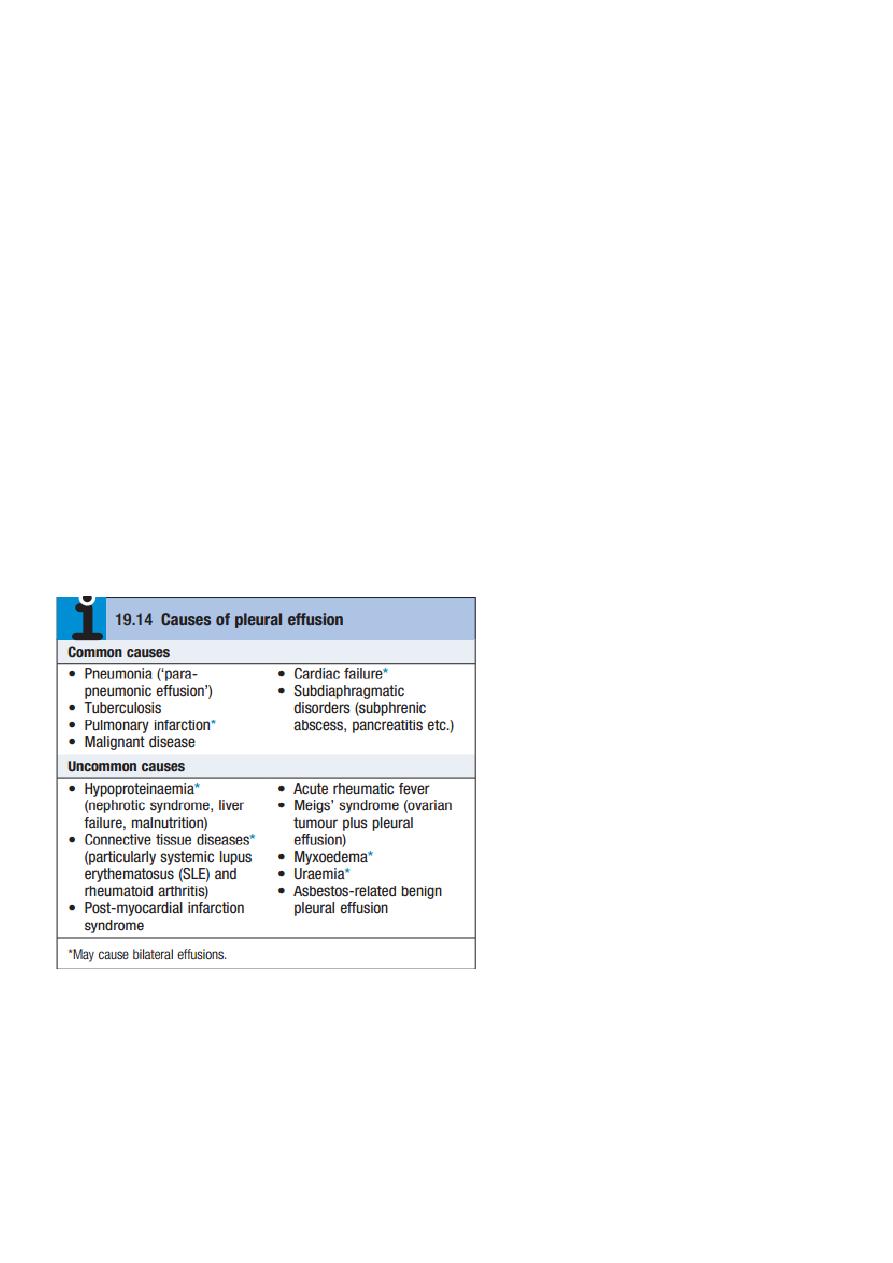
Q5: What are the main causes of pleural effusion?
Q6: Write about immediate assessment of acute severe asthma.
1. Acute severe asthma:
a) PEF 33-50% predicted (< 2001/min).
b) R.R ≥ 25/min.
c) H.R ≥ 110/min.
d) Inability to complete sentence in one breath.

2. Life – threatening features:
a) PEF 33-50% predicted (< 100 1/min).
b) SpO2 < 92% or PaO2 < 8 kpa (60 mm Hg).
c) Normal PaCo2.
d) chest.
e) Cyanosis.
f) Feeble respiratory effort.
g) Bradycardia.
h) Hypotension.
i) Exhaustion.
j) Confusion and coma.
3. Near-fatal asthma:
a) (raised PaCo2 and/ or requiring mechanical Ventilation with raised
inflation pressures).
b) O2: High conc. to maintain O2 saturation above 92% .Increase PaCo2 is
not indicator to reduce O2 conc. but is a warning sign of a severe or life
threatening attack.
c) High doses of inhaled bronchodilator.
d) Systemic CS.: oral pred. 30-60 mg or I.V hydrocortisone 200 mg.
e) I.V fluid.
Q7: How to manage patient with acute severe asthma?
A. Initial assessment:-
1. Acute severe asthma:
a) PEF 33-50% predicted (< 2001/min).
b) R.R ≥ 25/min.
c) H.R ≥ 110/min.
d) Inability to complete sentence in one breath.
2. Life – threatening features:
a) PEF 33-50% predicted (< 100 1/min).
b) SpO2 < 92% or PaO2 < 8 kpa (60 mm Hg).
c) Normal PaCo2.
d) chest.
e) Cyanosis.
f) Feeble respiratory effort.
g) Bradycardia.
h) Hypotension.
i) Exhaustion.
j) Confusion and coma.
3. Near-fatal asthma:
a) (raised PaCo2 and/ or requiring mechanical Ventilation with raised inflation pressures).
b) O2: High conc. to maintain O2 saturation above 92% .Increase PaCo2 is not indicator to
reduce O2 conc. but is a warning sign of a severe or life threatening attack.

c) High doses of inhaled bronchodilator.
d) Systemic CS.: oral pred. 30-60 mg or I.V hydrocortisone 200 mg.
e) I.V fluid.
B. Subsequent management: if patients fail to improve,add I.V magnesium, I.V
aminophyline, I.V leukotriene receptor antagonists.
C. Monitoring of treatment:
1. PEF recorded every 15-30 minutes then every 4-6 h.
2. Pulse oximetry should ensure that SaO2 remains > 92%.
3. Repeat arterial blood gases are necessary if:
a) Initial PaCo2 measurements were normal or raised.
b) The PaO2 was < 8 Kpa (60 mmHg), or
c) The patient deteriorates.
Q8: What are the risk factors of COPD?
Q9: How to manage patient with acute exacerbation of COPD?
Oxygen therapy:
• In patients with an exacerbation of severe COPD, high concentrations of oxygen may
cause respiratory depression and worsening acidosis. Controlled oxygen at 24% or 28%
should be used with the aim of maintaining a PaO2 more than 8 Kpa ( 60 mmHg)
(or an SO2 more than 90%) without worsening acidosis.
Bronchodilators:
• Nebulised short-acting β2- agonists combined with an anticholinergic agent should be
administered. Provided patients are properly supervised it is usually safe to drive
nebulisers with oxygen, but if concern exists regarding oxygen sensitivity nebulisers
may be driven by compressed air and supplemental oxygen delivered by nasal
cannula.
Corticosteroids:

• Oral prednisolone reduces symptoms and improves lung function. Currently doses of
30 mg for 10 days are recommended but shorter courses may be acceptable.
Prophylaxis against osteoporosis should be considered in patients who receive
repeated courses of steroids.
Antibiotic therapy:
• The role of bacteria in exacerbations remains controversial and there is little evidence
for the routine administration of antibiotics. They are currently recommended for
patients reporting an increase in sputum purulence, sputum volume or breathlessness.
In most cases simple regimens are advised such as an aminopenicillin or a macrolide.
Co-amoxiclav is only required in regions where β-lactamase-producing organisms are
known to be common.
Non-invasive ventilation:
• If, despite the above measures, the patient remains tachypnoeic and acidotic ( PH
less than 7.35) then NIV should be commenced. Several studies have shown that its
use is associated with reduced requirements for mechanical ventilation and reductions
in mortality. It is not useful in patients who cannot protect their airway. Mechanical
ventilation may be contemplated in those with a reversible cause for deterioration (e.g.
pneumonia), or when no prior history of respiratory failure has been noted.
Additional therapy:
• There has been a vogue for using an infusion of intravenous aminophylline but
evidence for benefit is limited and attention must be paid to the risk of inducing
arrhythmias and drug interactions. The use of the respiratory stimulant doxapram has
been largely superseded by the development of NIV, but it may be useful for a limited
period in selected patients with a low respiratory rate. Diuretics should be
administered if peripheral oedema has developed.
Q10: What are the risk factors of pneumonia?
1. Cigarette smoking 2. Upper respiratory tract infections 3. Alcohol 4. Corticosteroid
therapy 5. Old age 6. Recent influenza infection 7. Pre-existing lung disease 8. HIV 9. Indoor
air pollution
Q11: Write about diagnosis and management of pneumonia
1-Sputum 2-Serology 3-Cold agglutinins 4-Blood culture 5- Tracheal aspirate 6- CXR
Management: Rest and avoid smoking, Oxygen, Fluid balance, Antibiotic treatment.
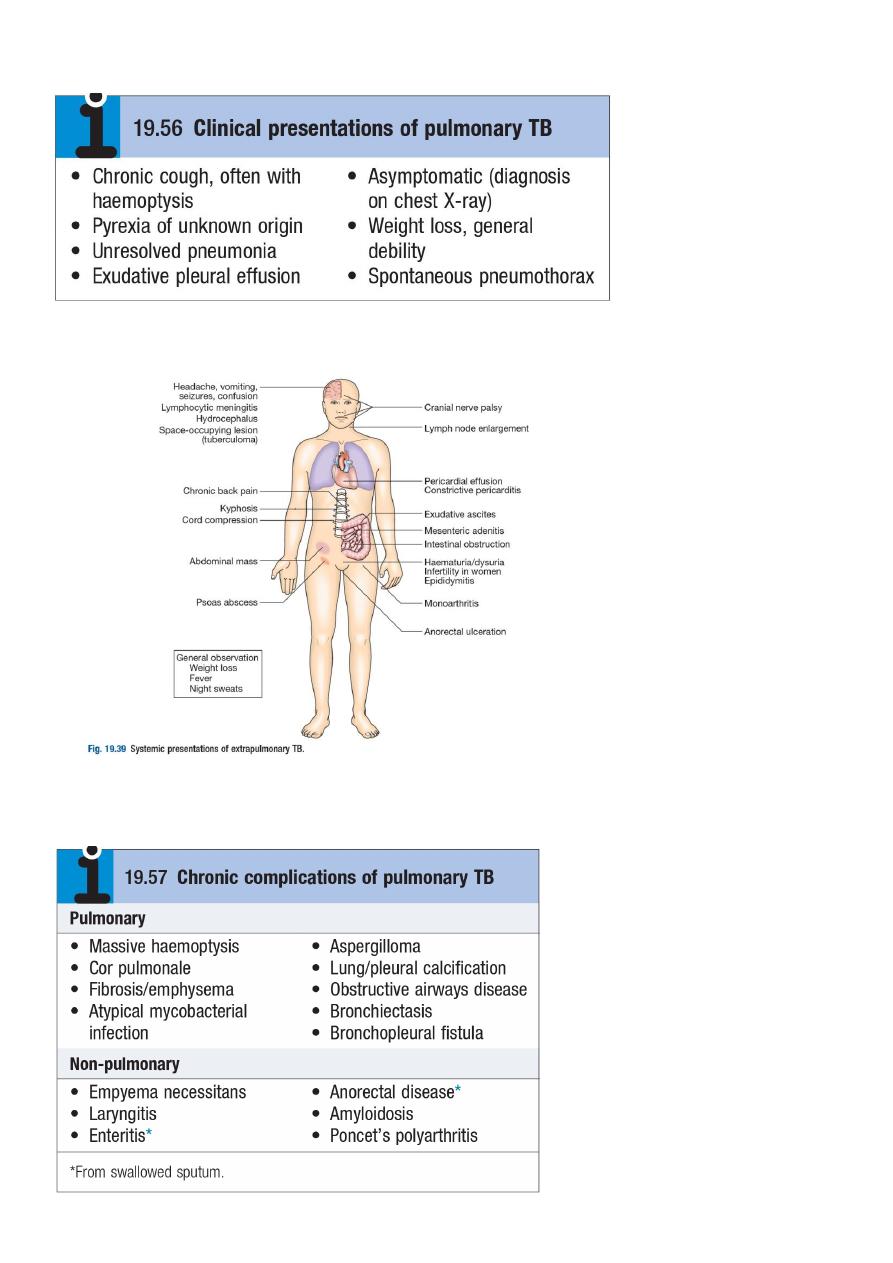
Q12: What are the clinical presentation of pulmonary TB?
Q13: What are the systemic presentation of extrapulmonary TB?
Q14: Write about chronic complications of pulmonary TB

Q15: What are the non-metastatic extrapulmonary manifestations of lung cancer?
1-Endocrine;
• Inappropriate antidiuretic hormone (ADH) secretion causing hyponatraemia.
• Ectopic adrenocorticotrophic hormone (ACTH) secretion.
• Hypercalcaemia due to secretion of parathyroid hormone (PTH)-related peptides.
• Carcinoid syndrome.
• Gynaecomastia.
2-Neurological
• Polyneuropathy
• Myelopathy
• Cerebellar degeneration
• Myasthenia (Lambert-Eaton syndrome)
3-Other
• Digital clubbing
• Hypertrophic pulmonary osteoarthropathy
• Nephrotic syndrome
• Polymyositis and dermatomyositis
• Eosinophilia
Q16: Write about pathophysiology of asthma:
the cardinal pathophysiological features of asthma: A- Airflow limitation. B- Airway hyper-
reactivity.
C- Airway inflammation. "Eosinophils, Lymphocytes, mast cells, neutrophils lead to odema,
Smooth m. hypertrophy and hyperplasia, thickening of basement membrane, mucous
plugging and epithelial damage".
Q17: What are the indications of antibiotics and steroids in COPD?
Steroid recommended in patients with severe disease (FEV1less than 50%) who
report two or more exacerbations requiring antibiotics or oral steroids per year.
Antibiotics recommended for patients reporting an increase in sputum purulence, sputum volume
or breathlessness.

Cases
Case1: female has flapping tremor with confusion and jaundice, ascites, and sings of chronic
liver disease. ((the case is hepatic encephalopathy))
Case2: Male who has history of alcohol ingestion presented with signs of shock and
jaundice and signs of chronic liver disease with hematemesis and melena. ((the case is
esophageal varcies due to portal hypertension))
Case3: Adult girl presented with pan-systolic murmur at the apex with forceful sustained
apex beat and dyspnea and chest pain and small jerky pulse. ((the case is mitral
regurgitation))
Case4: Elderly presented with dyspnea, fever for 1 month, weight loss, night sweating, ESR
90, family history with same disease. ((the case is TB))
Case5: Female 40 years old presented with nausea, jaundice, anorexia, right hypochondrial
discomfort for two weeks, and she has normal values of liver function test. ((the case is ….))
Case6: Male 70 years old with chronic hypertension for 15 years, presented with ptosis of
left eye, planter reflex upward, loss of sensation and numbness of left side of the face and
right side of the body, vertigo, nausea, vomiting, dysphagia and salivation. ((the case is
stroke - PICA syndrome))
Case7: Male 25 years old presented with Troponin T and I and CK with basal crepitation and
palpitation, chest discomfort, 38 C fever, 112 pulse. ((the case is pulmonary edema from
complicated MI))
Case8: Non smoker and non drinker female 50 years old, presented with dysphagia for food
with liquids and she has long history of heartburn. ((the case is esophageal stricture))
Case9: Female 30 years old presented with painful right eye movement and vision, before
one year she had the same condition in the left eye, she had frequency and hesitancy. ((the
case is multiple sclerosis))
Case10: Female 50 years old presented with sudden severe headache, photophobia,
Kerning sign, neck stiffness, -ve CT scan, and she had history of severe hypertension. ((the
case is subarachnoid hemorrhage))
Case11: female 50 years old presented with proteinuria (2.5 g/24h), low level of
complements, periorbital edema, and hypertension. ((the case is nephritic syndrome))
Case12: old age female with spider naïve, +ve shifting dullness, and palmer erythema ((the
case is chronic liver disease like cirrhosis))
Case13: young female with –ve reflex in the left leg, +ve in upper limb, with grade II power
in the upper limb while grade I in the left leg progress over week. ((the case is Gillian barre
syndrome))
Case14: 60 years old male develop cough, fever 38.5 C, right chest pain, bronchial breathing
heard over right chest, plural rub heard over right mid-axillary line. ((the case is lobar
pneumonia))
MCQs
Q1: Which of the following is used in the diagnosis of patient with chronic diarrhea,
anemia, and villous atrophy on duodenal biopsy?
- AMA
- ANA
- ASMA
- Anti-endomysial antibodies ((true))
Q2: Poor prognostic factors in acute pancreatitis except:
- Old age
- serum amylase > 1000 ((true))
- hyperglycemia
- hypoalbuminema
Q3: all true about lacunar infarction except:
- > 3 cm ((true))
- mostly caused by hypertension
- usually presented with pure motor and sensor deficit
- involve putamen, thalamus and caudate
Q4: about migraine all true except:
- topiramte is preventive drug
- preceded by aura is the commonest type ((true))
- present with hemiplegia
Q5: What case prolong life in COPD:
- topriamate
- sildenafil
- LTOT ((true))
Q6: about HSV1 encephalitis all true except:
- Glucose decrease ((true))
- management by oral acyclovir
- >90% diagnosed by CSF tests
Q7: 20 years old male presented with fatigue, malaise, anorexia, abdominal discomfort
for 1 week then develop jaundice, bilirubin > 200 mg/dl, ALT > 1000 U/l, the diagnosis is:
- Gilbert

- Autoimmune hepatitis
- Acute viral hepatitis ((true))
Q8: Loud S1 seen in:
- MS ((true))
- AS
- ASD
- LVH
Q9: about Inflammatory bowel disease all true except:
- Colicky abdominal pain
- Tenesmus and stool with mucus
- sleep disturbance
- alternate constipation and diarrhea ((true))
Q10: Risk factors for stomach cancer all true except:
- Smoking
- H.pylori
- ZES ((true))
- Autoimmune gastritis
Q11: Severe lower GI bleeding seen in all except:
- Anal fissure ((true))
- Angiodysplaisa
- Bowel ischemia
- Diverticular disease
Q12: Risk factors for peptic ulcer all true except:
- Pernicious anemia ((true))
- H.pylori
- ZES
- NSAID
Q13: Sings of portal hypertension all true except:
- splenomegaly
- fetor hepaticus
- variceal hemorrhage
- spider telangiectasia ((true))
Q14: Proteinuria occur normally in all except:
- orthostatic ((true))
- after sleep
- after fever
- after exercise

Q15: dipstick +ve for proteinuria occur in all except:
- UTI
- TCC
- UT trauma
- Micro-albuminuria ((true))
Q16: We should do CT scan in meningitis in all except:
- Depress conscious level
- Functional neurological disorder
- suspicion of a mass
- +ve krning sign ((true))
Q17: The most important initial investigation in patient with direct hyperbilirubnemia:
- abdominal US ((true))
- abdominal CT
- ERCP
- Portal angiography
Q18: all of the following are caused by H.pylori except:
- gastric leiomyoma ((true))
- peptic ulcer
- gastric lymphoma
- gastric cancer
Q19: Hemorrhagic plural effusion except:
- CHF ((true))
- RA
- Malignancy
- Trauma
Q20: infection with L.monocytogen in meningitis:
- prophylactic to immune compromise
- prophylactic to child
- all of above ((true))
Q21: What are the clinical picture of acute pancreatitis?
- Lower GI bleeding
- respiratory distress syndrome
- renal failure
- none ((true))
Q22: Management of acute exacerbation all true except?
- 25-30 % O2
- Bronchodilator
- weight loss

- None ((true))
Q23: Eradication therapy of H.pylori show benefit in all except?
- Carcinoma ((true))
- maltoma
- gastritis
Q24: All these factors commonly precipitate angina except?
- Vivid dream ((true))
- cold exposure
- emotion
- exercise
Q25: All of these are causes of esophageal stricture except?
- Hiatus hernia ((true))
- GERD
- CA bronchus
- Esophagitis
Q26: in SAH all true except?
- 20% are multiple
- rupture occur if aneurysm > 1 cm ((true))
- rupture most common in 20 years male
Q27: the most likely diagnosis of 50 years male with persistent proteinuria (3.5 g/24 h):
- Chronic UTI
- TCC
- ATN
- FSGN ((true))
- CIN
Q28: In vestibule-basilar stroke all true except:
- coma
- vertigo
- motor aphasia ((true))
- band back
Q29: migraine is differ from cluster headache by:
- unilateral
- vomiting ((true))
- treated by atenolol
Q30: RPGN caused by:
- good pasture syndrome
- IgA nephropathy ((true))

Q31: rest tremor occur in all except:
- Parkinson
- Wilson
- anxiety ((true))
- heavy metal poisoning
Q32: about hemochromatosis all true except:
- arthropathy
- hypogonadism
- bronze diabetes
- deforrexaimne in the drug of choice ((true))
Q33: all of the following are precipating factors for hepatic encephalopathy except?
- surgery
- diuretics
- flagyle ((true))
- infection
Q34: immediate management of MI all true except:
- ECG
- SC opiate and antiemetic ((true))
- aspirin
Q35: one of the following is mucosal cause of malabsorption:
- a betalipoprotenemia
- bacteria overgrowth ((true))
- ulcerative colitis
- vacuities
Q36: H.pylori all true except:
- gram –ve spiral bacteria
- risk of ca of stomach
- curative eradication in maltoma ((true))
- risk > 90% for DU
Q37: about silicosis all true except:
- highly fibrogenic
- egg shell on CXR
- risk of ca lung ((true))
- pottery is risk factor
Q38: evidence of renal failure with streptococcal infection include the following except:
- prophylaxis with penicillin decrease incidence of renal failure
- ASO titer is high in renal failure

- seasonal variation is the same
- isolation of streptococcus from the throat could take some time after diagnosis of renal
failure
- high incidence of renal failure with non-epidemic area of streptococcal infection ((true))
Q39: definition of pneumonia include all the following except:
- pneumonia refers to inflammation of the pulmonary tissue
- bronchopneumonia is usually a generalized process involving multiple lobes of the lung
- lobar pneumonia describes pneumonia localized to one or more lobes of the lung in which
affected lobe or lobes are completely consolidated
- it is associated with consolidation of alveolar space
- pneumonitis in a general term for lung inflammation that may or may not associated with
consolidation ((true))
Q40: treatment of moderate persistent asthma include all except:
- low-dose inhaled corticosteroids
- long acting B2 agonist
- leukotriene receptor antagonist
- theophylline
- systemic steroid ((true))
Q41: about X-ray in acute asthma all true except:
- hyperinflation
- diaphragm is down to the 11
th
rib
- increased AP lateral diameter
- perihilar thickening ((true))
- most patient with asthma have normal x-ray