
Obstetric Questions:
#Explain the management of slow progress during the active phase of the 1
st
stage of spontaneous labor in a nulliparous lady?
1- Do general clinical examination + abdominal examination
2- Pelvic examination: assess the cervical dilatation and cervical effacement
3- Examine the fetal station, position, presentation
4- Assess the fetal condition
5- Natural methods of intervention used to promote labor include nipple stimulation,
position changes, food and fluids, herbs, homeopathy, and rupturing the membranes
6- A more medical approach may involve having an intravenous oxytocin
7- It’s important that a laboring women feel safe and relaxed. Fear or stress can interfere
with labor progress
8- Pain relief
9- Correct fetal position and presentation
#Define miscarriage, list its types and explain the management of one of them
only?
Definition: expulsion of conception products before 24 weeks of gestation
Types: complete, incomplete, missed, threatened, inventible, septic, habitual
Management of missed type: evacuation of the uterus by combination of intra-vaginal
prostaglandins and I.V oxytocin infusion, In early cases do surgery by ring forceps &
dilatation and curettage (DNC)
#What are the causes of abortion?
o Fetal diseases: malformation of zygote, defective development of the fertilized ovum,
fatal genetic problem of the fetus
o General diseases of the mother: rubella, syphilis, toxoplasma, malaria, D.M,
hypertension, renal disease, acute emotional disturbance
o Uterine abnormalities: double septate uterus, sub-mucous fibroma, uterine
retroversion and incarceration, incompetent internal os of the cervix

o Hormonal imbalance: progesterone deficiency, thyroid deficiency, hyperthyroidism
o Irritation of the uterus early in pregnancy
o Drugs: cytotoxic, lead poisoning, oxytocin, ergot, prostaglandins, quinine
o Trauma: insertion of instrument or foreign body through the cervix, surgical operation
(myomectomy), severe trauma to the uterus
o Other causes: immune responses, physical problems in the mother, maternal age,
smoking, drug use, malnutrition, excessive caffeine, exposure to radiation or toxic
materials.
#Write short note about septic abortion?
Infection during pregnancy (fever, weakness, increased pulse rate, broad like rigidity)
Management: broad spectrum antibiotics, blood culture, vaginal swap, evacuation of the
uterus by suction curettage under G.A and antibiotics cover, oxytocin, vaginal
prostaglandins
#What is the differential diagnosis for large for date?
Edema and Full bladder
Rapid fetal growth
Miscalculation (Wrong LMP)
Polyhydramnious
Multiple pregnancies
Macrosomia (diabetic mother)
Abruption placenta
Multiple uterine fibroids
#What are the complications of multiple gestations?
A. Maternal:-
Anemia, Hydramnios, Preeclampsia, Preterm labour, Postpartum hemorrhage, Cesarean
delivery.
B. Fetal:-
Malpresentation, Placenta previa, Abruptio placentae, Premature rupture of the
membranes, Prematurity, Umbilical cord prolapsed, Intrauterine growth restriction,
Congenital anomalies.

#What are the risks of multiple fetal pregnancy?
A. Abortion: Increase spontaneous abortion more than three times.
B. Malformation: Congenital malformation > single
C. Low birth weight: 1. growth restriction (estimated fetal weight less than 10th percentile
for singleton gestation), 2. preterm, 3. discordance (difference in estimated fetal weight of
greater than 20%-25% between twin A and twin B).
D. Decrease duration of gestation: 1. 57% of twins à at 35 weeks, 2. 92% of triplets à at 32
weeks, 3. all quadruplets à at 29–30 weeks
E. Preterm birth: 1. It is the most common complication of multiple pregnancies effecting
long term out come, 2. prophylactic use of Tocolytics , Bed rest, Cerclage, 3. fetal
fibronectin (at 24-28 weeks if high associated with increase risk of preterm before 32 weeks
of gestation).
F. Intrauterine fetal demise of one twin (late pregnancy), Vanishing twin (early pregnancy).
#Define internal podalic version?
maneuver to deliver the fetus by inserting a hand into the uterine cavity, grasping one or bo
th feet, and drawing them through the
cervix; rarely indicated today except for the delivery
of a second twin.
#Define fertilization, ovulation and placentation?
((The answer from Wikipedia))
Fertilization is the union of a human egg and sperm, usually occurring in the ampulla of the
uterine tube. The result of this union is the production of a zygote cell, or fertilized egg,
initiating prenatal development.
Ovulation is the release of egg from the ovaries. This event occurs when the graffain
follicles rupture and release the secondary oocyte.
Placentation refers to the formation, type and structure, or arrangement of placentas. The
function of placentation is to transfer nutrients from maternal tissue to a growing embryo.
#How to estimate fetal age?
1- By Naegele's rule
2- Fundal height
3- Quickening
4- Ultrasound
5- Fetal weight

#Define effacement, moulding and caput?
Effacement is a process by which the cervix shortens in length as it becomes included into
the lower segment of the uterus. The process of effacement may begin during the weeks
preceding the onset of labor but will be complete by the end of the latent phase.
Molding is the alteration of the fetal cranial bones to each other as a result of compressive
forces of the maternal bony pelvis.
Caput is the localized edematous area on the fetal scalp caused by pressure on the scalp by
the cervix.
#Explain management of third stage?
Controlled cord traction:
- The Placenta is delivered using one hand on umbilical cord with gentle downward traction.
- The Other hand should be on the abdomen to support the uterine fundus, this is the
active management of third stage.
- Risk factor for aggressive traction is uterine inversion , it is an obstetrical emergency!!
#What are the characteristics of normal low-risk labor?
A. No pregnancy complications that may affect labor (with adequate ANC).
B. Spontaneous onset of labor between 37-42 week of gestation.
C. Singleton fetus with cephalic presentation.
D. Estimate fetal weight > 2,500 g, < 4,000 g.
E. Adequate volume of clear amniotic fluid.
F. No abnormal intrapartum bleeding.
G. Acceptable rate of cervical dilatation (1 cm/hr in active phase).
H. Normal fetal heart rate.
#What are the risk factors for poor progress in labor?
1. Small women.
2. Big baby.
3. Malpresentation.

4. Malposition.
5. Early membrane rupture.
6. Soft tissue /pelvic malformation
#How often should patient be seen in ANC?
1. First visit in early pregnancy.
2. Then every 4 weeks until 28 weeks.
3. Then every 2 weeks until 36 weeks.
4. Then weekly until delivery.
5. For high risk patients, individualized and more visits.
#Write about ultrasound during 1st trimester?
Used in:
- Diagnose pregnancy.
- Assure accurate dating.
- Fetal number.
- Fetal viability.
- Adnexial mass.
- Screen for chromosomal anomalies; Nuchal translucency & nasal bone.
#What are the complications of pregnancy can be prevented or minimized by
good ANC?
1. Anemia due to iron or folic acid deficiency.
2. Urinary tract infections and pyelonephritis.
3. Pregnancy induced hypertension & PET.
4. Preterm labour and delivery.
5. Intrauterine growth restriction.
6. Sexually transmitted diseases.
7. Rh isoimmunization.

8. Fetal macrosomia.
9. Hypoxia or fetal death from post-term birth.
10. Breech presentation at term.
#Define malpresentation, malposition and breech presentation?
Malpresentation is any presentation other than vertex, which is the commonest
presentation.
Malposition is position other than occipito-anterior, like occipito-posterior.
When fetal buttocks or legs enter the pelvis before the head, the presentation is breech.
#What are the complications of antepartum asphyxia?
Stillbirth Mortality
Metabolic acidosis at birth Metabolic acidosis
Hypoxic renal damage
Necrotizing enterocolitis
Intracranial haemorrhage
Seizures
Cerebral palsy
#What are the causes of preterm labor?
1- Genital tract infection (bacterial vaginosis, chlamydia trachomones)
2- other infections like pyelonephritis, meningitis, pneumonia, malaria
3- placental abnormality like placenta pravia, placenta abruption
4- congenital disease of the uterus like unicornuate, biseptate uterus, cervical weakness
5- Fetal causes like fetal abnormality, increase fetal weight, congenital anomalies
6- Idiopathic
7- Iatrogenic due to medical intervention in severe bleeding, in heart diseases, fetal cause
like IUGR, fetal hypoxia
8- Social factors: maternal age, weight, race, educational level, economic, life style,
smoking, STDs, drug abuse, anemia, D.M, hypertension.
#What are the Pre-requisites for Forceps Delivery?
head engaged
presentation vertex or chin anterior

position known
cervix completely dilated
membranes ruptured
no disproportion between head & pelvis
#What are the methods of vaginal breech delivery?
1.spontaneous breech delivery,the fetus is expelled entirely spontaneously without any
traction or manipulation other than support of the newborn.
2.partial breech extraction,the fetus is delivered spontaneously as far as the umbilicus but
the remainder of the body is extracted or delivered with operator traction & assisted
maneuvers.
3.Total breech extraction,the entire body of the fetus is extracted by the obstetrician
Induction or augmentation of labor in women with a breech is controversial.
#Enumerate the contraindications of vaginal delivery in breech presentation?
1.placenta previa
2.nonreassuring fetal status
3.rupture of membranes
4.uterinr malformations
5.multiple gestation
6.recent uterine bleeding
7. prior uterine incision is a relative CI
#Define recurrent abortion and its causes? (
(The answer from Wikipedia))
Recurrent miscarriage, habitual abortion, or recurrent pregnancy loss (RPL) is a disease
distinct from infertility, defined by two or more failed pregnancies.
Causes:
Anatomical conditions (uterine malformation, cervical incompetence)
Chromosomal disorders (Translocations, Aneuploidy)
Endocrine disorders (hypothyroidism, polycystic ovary syndrome)
Thrombophilia

Immune factors (Antiphospholipid syndrome, Thyroid antibodies, Increased uterine NK
cells, Parental HLA sharing, Male-specific minor histocompatibility)
Ovarian factors (Reduced ovarian reserve, Luteal phase defect)
Lifestyle factors (smoking, alcohol, and drugs)
Infection (rubella, herpes simplex, measles, cytomegalovirus, coxsackie virus)
#Define the following?
1- Deep transverse arrest: Mechanical obstruction of labor in which the fetal head is unable
to rotate from occipitotransverse to occipitoanterior position
2- hydrops fetalis: is a serious fetal condition defined as abnormal accumulation of fluid in 2
or more fetal compartments, including ascites, pleural effusion, pericardial effusion, and
skin edema.
3- Vertex: it is the area of the fetal skull bounded by the two parietal eminences and the
anterior and posterior fontanels.
4- Pelvic inlet: it is the inlet of the pelvis that is bounded in front by the symphysis pubis, on
each side by upper margin of the pubic bone, ileopectineal line and ala of sacrum, and
posteriorly by the promontory of the sacrum.
5- Placenta previa: abnormal location of the placenta over or in close proximity to the
internal os.
#What is a biophysical profile?
A biophysical profile is a simple, painless test that's performed during pregnancy to assess
your baby's well-being, and it is include: fetal tone, fetal movement, fetal respiration, non-
stress test, amniotic fluid pocket.
#What is the purpose of routine Ultrasound exam?
Check baby has a heartbeat.
Say whether mother pregnant with one baby or twins or more.
Detect an ectopic pregnancy, where the embryo implants outside the womb, usually in
the fallopian tube.
Find out the cause of any bleeding that may be having.
Accurately date pregnancy by measuring baby.
Assess baby's risk of Down's syndrome.
Find out why a blood screening test was abnormal.

Help with diagnostic tests, such as CVS or amniocentesis, by showing the position of the
baby and placenta.
Examine baby to see if all his organs are normal.
Diagnose most abnormalities, such as spina bifida.
Assess the amount of amniotic fluid, find out where the placenta lies.
Measure baby's rate of growth over several scans.
#What are the goals of ANC?
To prevent and identify maternal or fetal problems that adversely affect pregnancy
outcome.
To educate the patient about pregnancy, labor-delivery, and parenting as well as about
ways she can improve her health.
To promote adequate psychological support from her partner, family and caregivers.
#Write short notes about Contracted pelvis?
In android pelvis
Not delivered vaginally, but always by caesarian section
Clinical hints that indicate contracted pelvis:
o Failure of engagement (especially in primi)
o Early rapture of membrane
#What are the sigs of fetal distress?
Lead to: Decreased movement felt by the mother, Meconium in the amniotic fluid, Non-
reassuring patterns seen on cardiotocography (increased or decreased fetal heart rate,
decreased variability, late decelerations), Biochemical signs (fetal metabolic acidosis,
elevated fetal blood lactate levels).
Clinical features: Tachycardia, Hypoxia, Chorioamnionitis, Maternal fever, Mimetic
drugs, fetal anemia, sepsis, heart failure, arrhythmias.
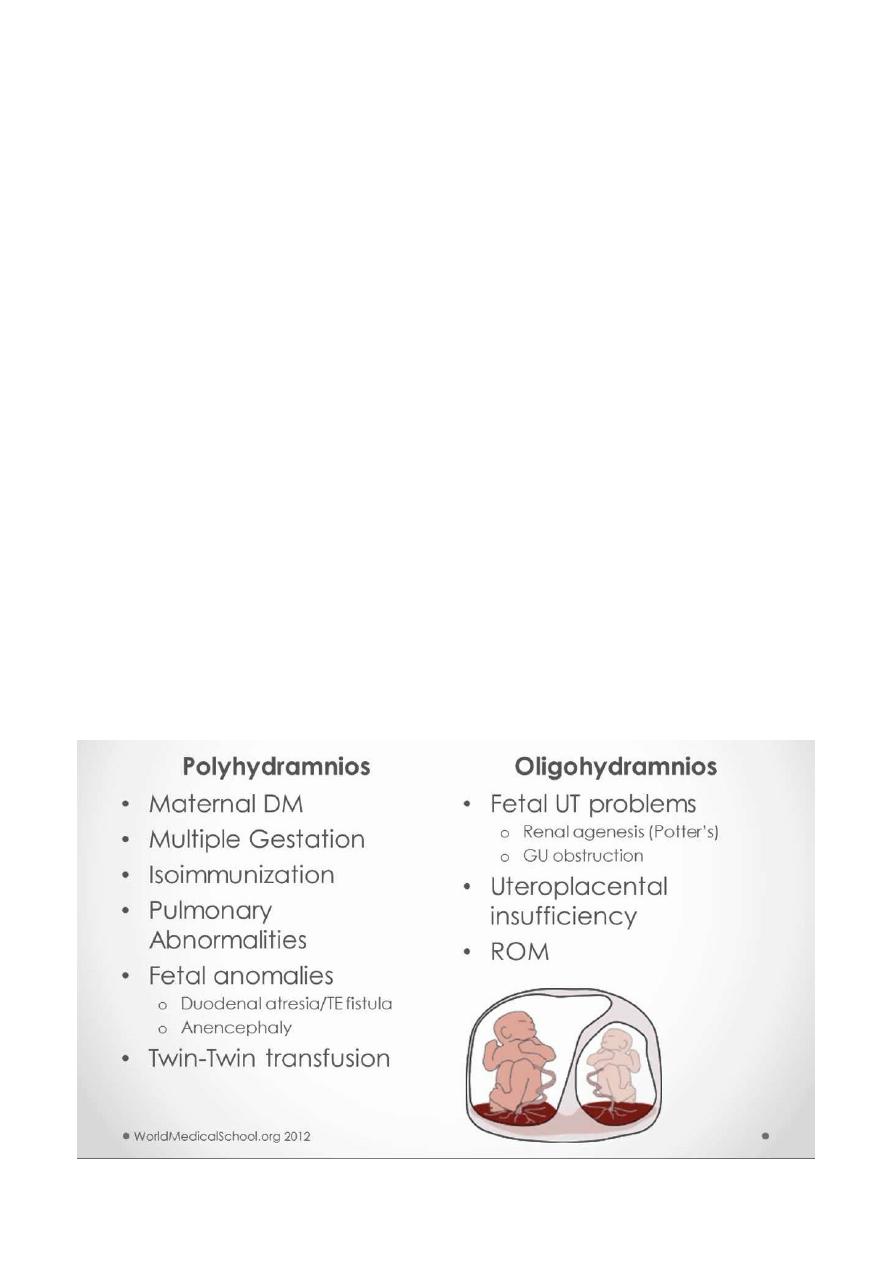
#What is the causes of polyhydramnious?
Fetal: Multiple pregnancies and Fetal abnormalities: anencephaly, esophageal and
duodenal atresia, spina bifida, skeletal or cardiac or intrauterine infection (rubella –
toxoplasma), fetal tumors
Maternal: D.M and Rh isoimmunization
Placental: chorioangioma and circumvallate placenta syndrome
Idiopathic
#What are the indications and contraindication of labor induction?
Possible indications for labor induction may include gestational or chronic hypertension,
preeclampsia, eclampsia, diabetes, premature rupture of membranes, severe fetal growth
restriction, and postterm pregnancy. However, physicians should decide whether labor
induction is warranted on a case-by-case basis, after consideration of maternal and infant
conditions, cervical status, gestational age, and other factors.
Contraindications to labor induction include transverse fetal position, umbilical cord
prolapse, active genital herpes infection, placenta previa, and a history of previous
myomectomy.
#What are the signs of a uterine rupture?
The first sign of a rupture is usually an abnormality in the baby's heart rate. (This is one
reason why a woman attempting a vaginal birth after cesarean, or VBAC, needs continuous
fetal monitoring.)
The mother may also have symptoms such as abdominal pain, vaginal bleeding, a rapid
pulse, and other signs of shock, and she may even experience referred pain in her chest
caused by irritation to the diaphragm from internal bleeding. Labor may slow or stop.
#What are efficient uterine contractions?
Number of contractions (normally less than 5)
Duration of contraction (normally 45-60 seconds)
#What is Partogram?
Is a graph used in labor to monitor the parameters of progress of labor, maternal and fetal
wellbeing, and treatment administration
#How you could manage pregnant women with Rh- in 36 week of pregnancy?
First do blood group and Rh study to the mother and father blood to make sure that there
is Rh- mother with Rh+ father, then you should confirm the presence of Rh isoimmunization
by make some investigations like antibody screening, amniocentesis, amniotic fluid analysis,
spectrophotometry, cordocentesis, Coomb's test, and Doppler study for fetal middle
cerebral artery.
After that, if the mother have the first pregnancy with Rh-isoimmunization you should give
her Anti-D antibodies (300 microgram I.M) as prophylaxis for subsequent pregnancies.
Management of baby: if the baby is not mature you can give intrauterine blood transfusion
which need special center, but if the baby is mature you can do induction of labor and
delivery of baby bay vaginal route or cesarean section.
Postnatal monument of the neonate include: do some investigations like direct coombs
test, blood group, Rh type, Hb, and bilirubin, then if the case is mild you can do
phototherapy and correction of acidosis, but if the case is severe you can do exchange
transfusion.
#What are the criteria for vaginal delivery in breech?
#What are the physiological changes in pregnancy for CVS, Respiratory, and
cervix?
1- CVS: Blood:
Hemoglobin concentration.
Hematocrit.
Plasma folate concentration.
Protein S activity.
Plasma protein concentration.

Creatinine, urea, uric acid.
Erythrocyte sedimentation rate.
Fibrinogen concentration.
Activated protein C resistance.
Factors VII, VIII, IX, X and XII.
D-dimers.
Alkaline phosphatase.
2- CVS: Changes in circulatory system:
↑ Heart rate (10–20 per cent).
↑ Stroke volume (10 per cent).
↑ Cardiac output (30–50 per cent).
↓ Mean arterial pressure (10 per cent).
↓ Pulse pressure.
3- Respiratory system:
Thoracic anatomy changes.
↑ Minute ventilation.
↑ Tidal volume.
↓ Residual volume.
↓ Functional residual capacity.
Vital capacity unchanged or slightly increased.
Blood gas and acid–base changes:
↓ pCO2.
↑ pO2.
PH alters little.
↑ Bicarbonate excretion.
↑ Oxygen availability to tissues and placenta.
4- Cervix:
Increase in the ectocervix canal and secretion of cervical glands.
Increase in vascularity so that appear "bluer" in color and this what is called chadwick's
sign.
#How to manage 20 weeks pregnant women with D.M?
In gestational DM Treatment should be started as:
1. Dietary therapy: ώ appropriate caloric intake high fiber & complex carbohydrates:
a) (50-60) % CHO.
b) 20% Protein.
c) 25% Fat.
2. Insulin therapy: if initial blood glucose > 8 mmol/L or remain above 6 mmol/L in
spite of good diet control its stant single long acting injection at bed time. ώ
frequent measurement of blood sugar (about 4-6 times per day).
3. (Pre-prandial measurement) if blood glucose results during the day remain about
6 mmol/L its necessary to add 1-3 pre-prandial injection of short acting insulin
until keep blood sugar between (4-6) mmol/L.
4. Treatment of any complication like UTI, manila infection, regular check of B.P
and anemia treating on any other type of infection or C.
5. Obstetric MX. early trimester ULS by measurement of CR length to confirm
gestational age, exclude congenital abnormalities especially at 16weeks
deepened on biparietal diameter specially neural tube defects assess ant of CVS
system at (19-20 weeks) by ULS to excludde cardiac defects.
6. Serial measurements of fetal heed &abdominal circumferences to identify growth
of fetal and early detection of macrosomia.
7. Assessment of fetal wedge begs in third trimester by ULS & CTG done weekly or
twice weekly from 36 weeks gestation. Doppler ULS is required if there's element
of IUGR (which occur in Dm associated ώ sever PET).
8. Deal of complication like PET, preterm labour poly hydrations. Tocolytic like
salbutanal are diabetogenic effects and Elena blood sugar. So its C.I prefers
other types like adalate &Mg sulphate.
9. Timing of delivery our aim to achiever vaginal delivery between (38-
40 weeks) ώ
optimal diabetic control to reduce the ¢ of premastering and improve the chances
of spontaneous labour.
10. If patient necessity early delivery before 34 weeks due to badly controlled Dm or
other complication start 12mg dose of (Dexamethasone / 12 hours) Interval into
2 doses to improve lung maturity. Delivery after 40weeks ↑risk of macrosomia &
traumatic delivery due to shoulder Dystocia.
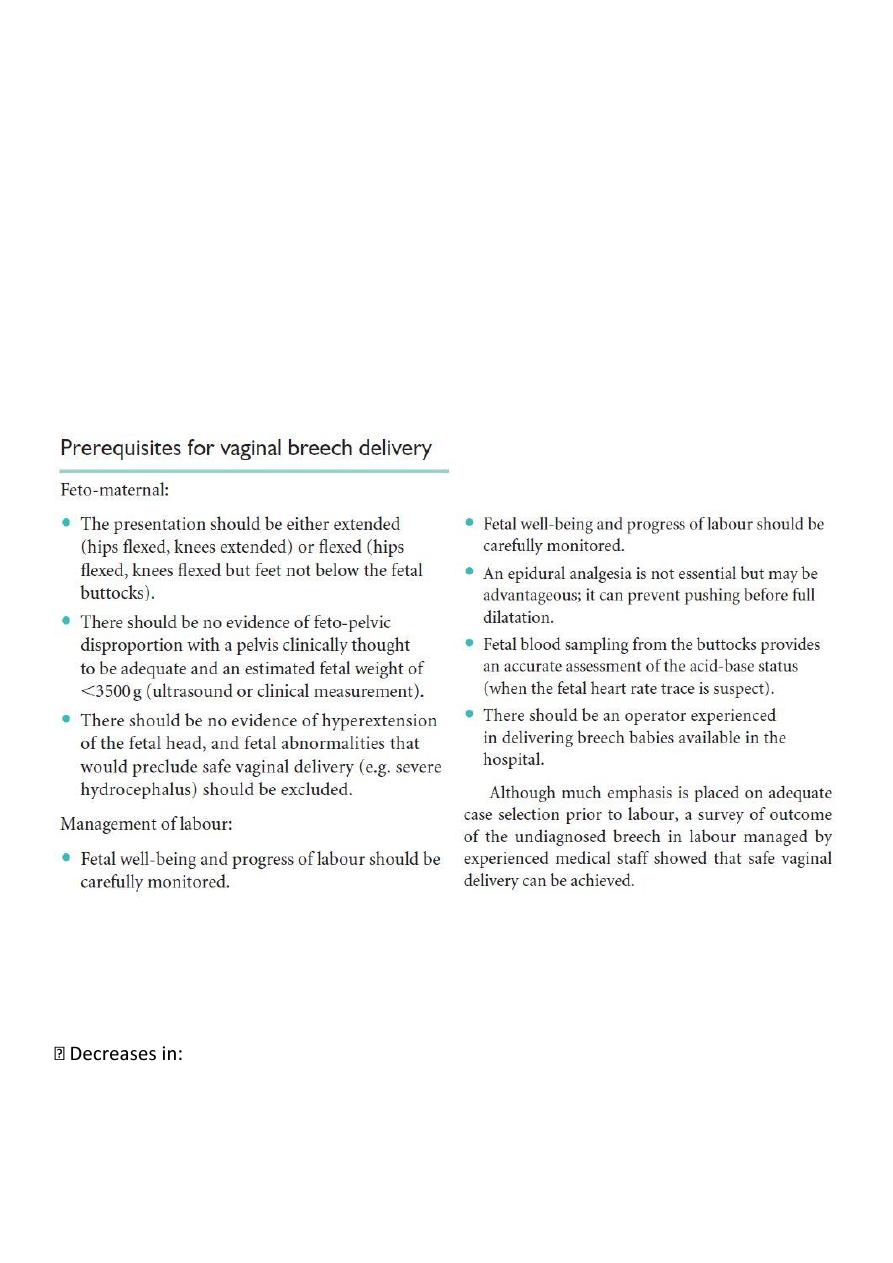
#What are the risk factors for shoulder dystocia?
#What are the effects of pregnancy on diabetes?
Change in eating pattern
Increase in insulin dose requirements
Greater importance of tight glucose control
Increased risk of severe hypoglycaemia
Risk of deterioration of pre-existing retinopathy
Risk of deterioration of established nephropathy
#What are the effects of diabetes on pregnancy?
Increased risk of miscarriage
Risk of congenital malformation
Risk of macrosomia
Increased risk of pre-eclampsia
Increased risk of stillbirth
Increased risk of infection
Increased operative delivery rate
#What are the investigations of fetal well-being in the 3rd trimester?
Assessment of fetal movement (kick count) at least 10 movements in 12 hours or 3-4
movements in 1 hour
Doppler U.S
Biophysical profile:
o Fetal tone
o Fetal breathing
o Fetal movements
o Amniotic fluid pocket: normally 4-5 liters (below 5 liters oligo)
o Non-stress test
heart rate this mean fetal distress.
Do intervertebral test
#What are the classification of hypertension in pregnancy, and management?
Classification:
1- Hypertension develop after 20 weeks of gestation in non-hypertensive patient with
blood pressure 140/90 mmHg (PIH)
2- Hypertension develop after 20 weeks of gestation with protein (300 mg or more in 24
hours) (Pre-eclampsia)
3- Chronic hypertension (Pre-existing hypertension)
4- Hypertension before 20 weeks of gestation without pre-exesting hypertension (non-
classified type)
Management:
Decease blood pressure
Oral Methyldopa centrally acting till 2000 mg/day
Oral labetalol (alpha-blocking and beta blocking agent)
Oral nifedipne 10-40 mg (calcium-channel blocker)
IV hydralazine, IV labetalol, IV Mg sulphate (in severe cases to decrease blood pressure
and control convulsion)
#Write short notes about tocolytic, and its contraindications?
Tocolytics are medications used to delay preterm labor, which may reduce neonatal
morbidity and mortality.
Maternal contraindications to using tocolytics include hypertension from such sources as
eclampsia or chronic hypertension, antepartum hemorrhage, heart disease, sensitivity to
medications used for tocolysis, and any medical indication that contraindicates
prolongation of the pregnancy.
Presumed fetal contraindications for tocolysis includes gestational age >37 weeks,
advanced cervical dilation and/or effacement, lethal anomaly, fetal demise, or
chorioamnionitis.
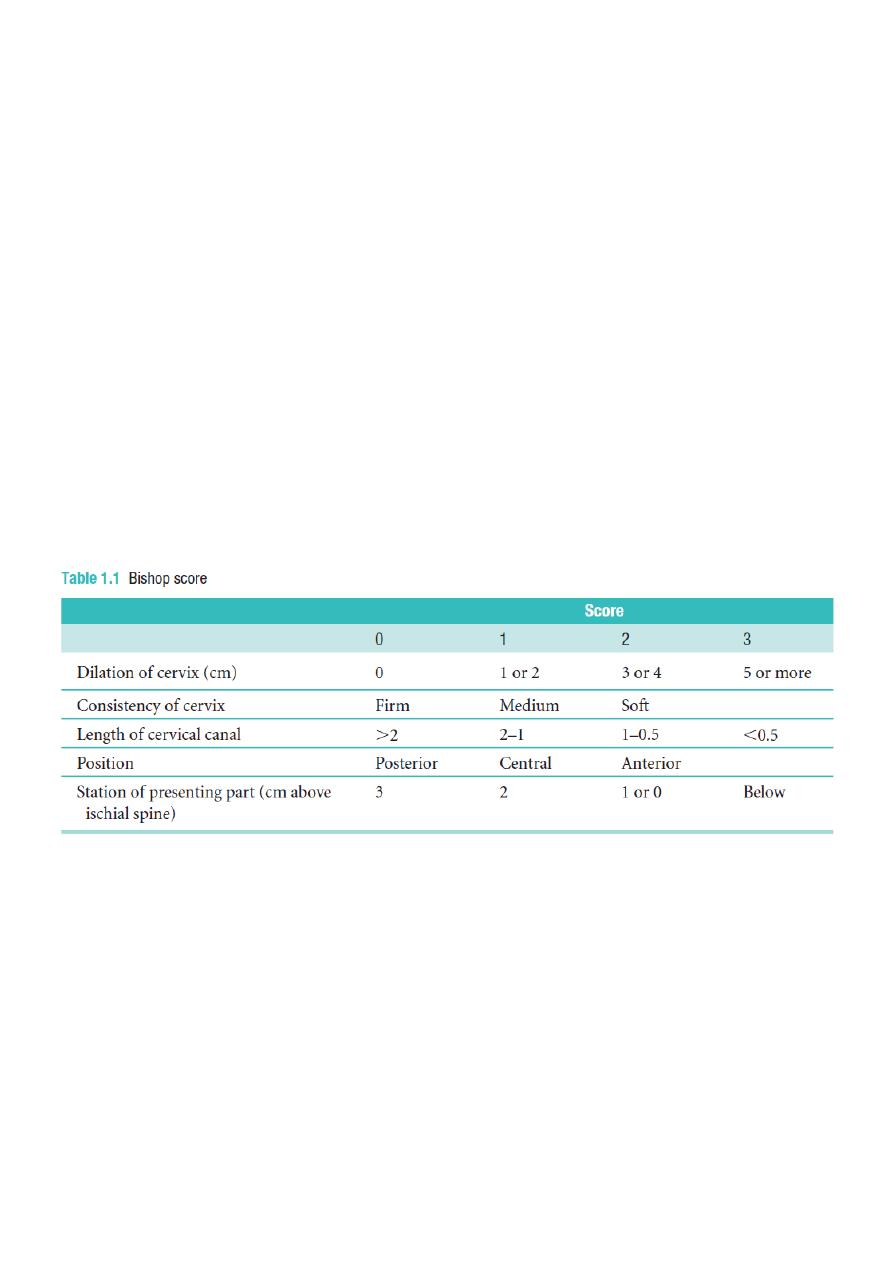
#What is Bishop score?
#What are the indications and contraindiactions of vaginal examination?
Indications:
Post-date pregnancy
Decreased fetal movements (normally 10 movements/12 hours)
Excessive or offensive discharge
Vaginal bleeding (in the known absence of a Placenta praevia)
To perform a cervical smear
To confirm potential rupture of membranes
Contraindications:
Known placenta praevia or vaginal bleeding when the placental site is unknown and the
presenting part unengaged
Pre-labor rupture of the membranes (increased risk of ascending infection)
#What are the indications of classical cesarean section?
Faults in the birth canal (passages): cephalopelvic disproportion, pelvic tumor, cervical
or vaginal stenosis or adhesions, double uterus obstruction
Fetal mal-presentation (passenger)
Uterine action (power)
Fulminating pre-eclampsia, hypertension, D.M
Repeated caesarian section
Fetal indication: placental insufficiency, cord prolapse, fetal distress (pass of meconium
green color discharge)
Bad obstetrical history: severe stillbirth or neonatal death
#What is the Management of primary PPH?
1- Identify the risk factors in the patient's history
2- Assess: vital signs, general condition, state of uterus, nature of bleeding, sign and
symptoms of blood loss, amount of blood loss, compare laboratory reports.
3- If atonic pregnancy: inform the obstetrician, massage the uterus, assess the general
physical condition, monitor pulse and blood pressure, put infant to the breast to suck or
stimulate the nipple manually, prepare instruments and equipments, administer
oxytocin, empty the bladder, examine the expelled placenta and membranes for
completeness, administer medication as ordered.
4- Reassure the mother
5- In case of traumatic bleeding, press on the tear or laceration, prepare equipment and
instruments.
#What are the causes of Polyhydramnious and oligo?

#How to manage heart diseases during pregnancy?
Antenatal management:
1- Cardiac examination.
2- Obstetric – cardiac clinic.
3- Decrease activity.
4- Echocardiography at the start of pregnancy and 28 weeks.
5- Table 12-1 , 12-2 (p 152)
6- Admission for bed rest.
7- Prosthetic heart disease 10% risk of thrombosis :
a- Use anticoagulant 6 -12 weeks (heparin).
b- Congenital heart diseases (warfarin).
c- Pulmonary hypertension (warfarin).
8- High risk heart conditions (p 153).
9- Fetal risk of maternal heart disease (p 153).
Management of labor:
1- Normal vaginal delivery is better.
2- Avoid induction.
3- Use antibiotic in structural heart defects.
4- Ensure fluid balance.
5- Avoid supine position.
6- Anesthesia – epidural with benefit to decrease pain and cause hypotension.
7- Shortened 2
nd
stage of labor by using oxytocin – slow administration.
8- Ensure good oxygenation.
9- Cesarean section (infection, hemorrhage , thrombosis ) unless its indicated.
#What are the conditions of Normal vaginal delivery?
1-normal pregnancy without usage of drugs that induced pregnancy
2-not use oxytocin for induction of the labor
3-not use vacuum or forceps in labor
4-No vaginal tear
5-No cervical tear
6-No artificial rupture membrane
7-No bleeding after delivery
8-No any compliant to mother
9-No any compliant to baby
#Define gestational diabetes?
One of the endocrine disorders affecting pregnancy and its significant hormonal
changes affect carbohydrate metabolism during pregnancy.
or
Diabetic defined: As either increases fasting blood sugar >7.8 mmol/L (144 mg/dl)
or > 11 mmol/L (200 mg/dl) following 75g glucose load (after 1-2 hour).

#Define fetal lie, presentation, position?
Fetal lie:the relation of fetal long axis to that of the mother, either longitudinal ,transverse
or oblique.
Presentation:that portion of the fetal body that is foremost within the birth canal or in close
proximity to it.
Position: the relationship of a chosen portion of the presenting part to the right or left sides
of the birth canal.
#What is the mechanism of labor?
1. Engagement:-
2. Descent:-
3. Flexion:-
4. Internal Rotation:-
5. Extension:-
6. Restitution:-
7. External Rotation:-
8. Expulsion:-
#What are the complications of forceps?
A. Maternal
1. episiotomy & lacerations
2. urinary and rectal incontinence
3. febrile morbidity
B. Fetal
1. apgar scores
2. cephalhematoma
3.caput
4. trauma
5. bilirubin
6. retinal he
#How to manage IUGR?
A. PROPHYLAXIS:
1. Small dose aspirin.
2. Protein energy.
3. Stop smoking.
4. Anti malaria.
5. Stop medications.
B. MONITORING:
1. Monitoring of normal SGA
– UADW better than bio physical profile & liquor.
2. CTG
– Unclear role – every 2 wk.
3. Monitoring of GRF.
-
if diagnosis > 34wk
→ delivery.
-
if diagnosis < 34wk
→ steroid.
-
if RDEF
→ delivery.
-
if AEDF
→ controversy.
-
MCA
→ ↑ flow → adaptive mechanism.
-
AEDF
→ fetal demise( 2 days to wk).
C. LABOR:
1. <37wk
→ C/S because at high risk of hypoxia & academia.
2. If normal UAD
→>37wk→ induction – continuous CTG, fetal scalp monitoring.
#How to manage acute uterine inversion?
1- Resuscitate patient (ABC)
2- Immediately replace uterus through cervix by manual compression
3- hydrostatic pressure by pouring saline
4- Tocolytics
5- Surgery to replace uterus
#What are the indications for induction in labor?
1- prolonged pregnancy
2- FGR
3- Pre-eclampsia
4- D.M
5- cholestasis
6- twin
7- PROM
8- APH
9- Rh isoimminization
#What are the differences between placenta pravea and placenta abruption?
Placenta pravea
Placenta abruption
Painless
Painful
Less distress
Distress
Soft abdomen
Tender tense abdomen
Abnormal lie, presentation
Normal lie, presentation
Normal CTG
Abnormal CTG
No preeclampsia
May be associated with preeclampsia
No coagulation defect
Coagulation defect

#How to manage twin pregnancy?
"Antenatal Management"
• Early diagnosis (mainly by ultrasound).
• Adequate nutrition: Caloric consumption increased by 300 Kcal per day,Iron 60-100
mg per day, Folic acid 1mg per day,
• Frequent prenatal visit: observe maternal and fetal complications, frequent ultra
sound à fetal growth, congenital anomalies, amniotic fluid, Doppler, BPP.
• Routine antenatal care for all women involves screening for hypertension and
gestational diabetes.
• These conditions occur more frequently in twin pregnancies and there is also a higher
risk of other problems (such as antepartum hemorrhage and thromboembolic
disease).
"Intrapartum Management":-
A. In Labor Management:-
1. Trained obstetrical attendant.
2. Available blood.
3. Good access I.V live.
4. CTG monitoring.
5. Anesthetist à ER C-S.
6. Pediatrician for each fetus.
7. Mode of delivery depend on presentation.
B. Preparation:-
1. A twin CTG machine should be used for fetal monitoring and a portable
ultrasound machine should be available during delivery.
2. A standard oxytocin solution for augmentation should be prepared, run
through an intravenous giving-set and clearly labelled
‘for augmentation’, for
use for delivery of the second twin, if required.
3. A second high-dose oxytocin infusion should also be available for the
management of postpartum hemorrhage.
4. It is essential that two neonatal resuscitation trolleys, and two pediatricians
are available and that the special care baby unit and anesthetist are informed
well in advance of the delivery.
C. Twin Delivery:-
•
Analgesia during labour.Epidural analgesia is recommended.
•
Fetal well-being in labour.
-
Fetal heart rate monitoring should be continuous throughout labour.
-
An abnormal fetal heart rate pattern in twin I may be assessed using fetal
scalp sampling, as for a singleton pregnancy.
-
However, a non-reassuring pattern in twin 2 will usually necessitate delivery by
Caesarean section.
-
The condition of twin 1, as acute complications such as cord prolapse and
placental separation are well recognized.
-
Delivery of the first twin is undertaken in the usual manner and thereafter the
majority of second twins will be delivered within 15 minutes.
-
After the delivery of the first twin, abdominal palpitation should be performed to
assess the lie of the second twin.
-
It is helpful to use ultrasound for confirmation, which is also useful for checking

the fetal heart rate.
-
If the lie is longitudinal with a cephalic presentation, one should wait until the
head is descending and then perform amniotomy with a contraction.
-
If contractions do not ensue within 5-15minutes after delivery of the first twin,
an oxytocin infusion should be started, out let forceps and vacuum extraction
can be used.
-
IF second twin transverse or oblique presentation, we can perform external
cephalic version or breech extraction with or without internal podalic version.
-
Continue oxytocin drip &give ergometrine to avoid risk of PPH,handle both
cords deliver them by controlled cord traction method.
•
Delivery of vertex-non-vertex:-
-
Non-vertex first twin
-
When twin 1 presentation as a breech, clinicians usually recommend delivery
by elective Caesarean section.
-
Other factors include dwindling experience of breech delivery and the rarely
seen phenomenon of
‘locked twins’.
•
Internal podalic version;-
-
superior or posterior. If the back is inferior or if the limbs are not imnuediately
palpable, ultrasound may help to show the operator where they would be
found. This will rninirnize the unwanted experience