Pain
DEFENISIONPain: sensation of suffering resulting from a noxious stimulus, physical or mental derangement. It is an unpleasant sensory and/or experience associated with actual or potential tissue damage.
Pain is initiated with the activation of nociceptors at the free nerve endings of two fiber systems, A-delta and C fibers, found in almost every tissue in the body.
Activation is followed by transduction, whereby mechanical, thermal, energy is converted into electrical - nerve impulses.
Lightly myelinated A-delta nerve fibres, conduct at rates of 12-30 m/s are responsible for bright, sharp, localized stabbing pain usually resulting from stimulation of mechanoreceptors (first or primary pain following acute
injury).
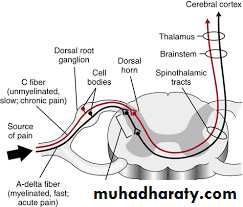
Stimulation of unmyelinated C-polymodal nerve fibres, which conduct at a rate of 0.5-2 m/s, gives rise to pain described as dull, aching and poorly localized (e.g. infection, secondary pain following acute injury, visceral
pain).
Following transduction, neural impulses are carried along primary afferent which enter the spinal cord via the dorsal roots or the brain stem via the cranial nerves. They end on inter neurons that make polysynaptic reflex connection to motor neurons at many levels as well as on the neurons of the ascending pathways that relay impulses to the cerebral cortex. The cortical receiving areas are concerned with the discriminative, exact, and meaningful interpretation of pain.
The main excitatory neurotransmitters for pain are substance P and glutamate. Inhibitory neurotransmitters include gamma aminobutyric acid (GABA), serotonin, norepinephrine and opioid-like chemicals, such as endorphins and enkephalins (which block pain by locking on to opioid receptors and switching on pain-inhibiting pathways or circuits).
Fast and slow pain
The presence of two pain pathways one slow and one fast explains the observation that there are two kinds of pain . A painful stimulus causes a sharp , localized sensation followed by a dull , intense diffuse and unpleasant feeling These sensations are variously called fast slow pain.Superficial And Deep Pain
The main difference between the superficial and deep sensibility is the different nature of the pain evoked by noxious stimuli. Unlike superficial pain, deep pain is poorly localized, nauseating, and is frequently associated with sweating, and changes in blood pressure.Somatic And Visceral Pain
The receptors for pain and other sensory modalities present in the viscera are similar to those in skin, but there are marked differences in their distribution. pain receptors are more sparsely distributed in the viscera compared to somatic structures, also there are few temperature and touch sense organs .Pain from visceral structures is poorly localized, unpleasant, associated with nausea and autonomic symptoms, and often radiates or is referred to other areas.
Referred Pain
Irritation of a viscus frequently produces pain which is felt not in the viscus itself but in a somatic structure that may be a considerable distance away.CLASSIFICATION OF PAIN BY ORIGIN
1-Nociceptive pain
Is believed to be caused by the ongoing activation of pain receptors in either the surface or deep tissues of the body. There are two types: "somatic" pain and " visceral" pain.
• a-"Somatic" pain is caused by injury to skin, muscles, bone, joint, and
• connective tissues.• b-"Visceral" pain refers to pain that originates from ongoing injury to the internal organs or the tissues that support them, when the injured tissue is a hollow structure, like the intestine or the gall bladder.
2-Neuropathic Pain
Arises from damage or alteration to the pain pathways, most commonly, a peripheral nerve injury from surgery or trauma, or central nervous system trauma as in thalamic stroke. Trigeminal neuralgia, post-herpetic neuralgia, post-stroke pain, and complex regional pain syndromes are examples.3-Psychogenic Pain
Resulting from psychic causes and not from noxious stimulation or neural abnormalities
CLINICAL EVALUATION OF PAIN
Clinical evaluation of pain requires an understanding of the patients subjective perception of discomfort. To reach such an understanding the following aspects must be studied:A- Onset of pain : A pain of brief duration from its onset to the request for treatment can suggest inflammatory somatic pain and exclude a chronic condition.
B- Localization of the pain : Somatic pain of the oral and perioral region nearly always arises from the affected site which is readily identified by the patient .inability of the patient to localize pain may indicate somatic pain originating from deep tissues or the pain is not somatic.
radiation of pain is the sensation of spreading to the adjacent areas from the primary source which may suggest a neurogenic component to the problem. (e.g acute pulpitis of mandibular first molar)
In rare instances pain is perceived at a site other than that of the somatic abnormality, this is referred or projected pain. (e.g MI pain or angina pectoris pain )
C-Characters of pain :
The descriptive terms chosen by the patient reflect his perception of pain, these could be sharp, dull aching, burning, stabbing, throbbing, pulsating.
The severity of pain can be graded as mild, moderate or sever based on its disruption of normal daily activities like sleeping, eating, working.
D- Course of pain :
The course of pain often suggests possible causes. Steady increase in the severity of pain is typical of a progressive acute inflammation produced by a bacterial infection. Periods of relief followed by recurrences is a pattern of pain often caused by chronic periapical lesions that episodically undergo acute exacerbations.E- Factors that alter pain :
Alteration of pain following exposure to certain agents or conditions can reveal its nature and possible causes. Application of ice can soothe pain from most superficial inflammatory causes, and moist heat usually relieves the deeper discomfort of muscle spasm.


F- Associated findings :
Certain systemic conditions can cause or influence the nature of pain, and a variety of drugs can accentuate pain perception. Emotional stress may exacerbate somatic pain or suggest psychogenic nature.
SOMATIC PAIN
PAIN OF PULPAL ORIGIN:A common problem in dental practice which results from stimulation of the neural fibers of the dental pulp which occurs with :
Exposed dentin :
Attrition, abrasion, erosion, gingival recession, caries and tooth fractures can expose dentin to the oral environment. Sensitivity of the exposed dentin surfaces results from direct stimulation of the odontoblastic processes by chemical and physical insults. The resulting pain sensation is usually mild to moderate and stops immediately after removing the stimulation. Gradual dentin exposure as in chronic Periodontitis or in slow caries is associated with milder pain sensation when compared with sudden or abrupt exposure as for example in tooth fractures affecting dentin .treatment is based on promoting dentinal tubules sclerosis by dentifrices and other root desensitizing procedures
Pulpitis :
Blunt trauma, restorative trauma, dentin exposure, thermal, large metallic restorations, traumatic occlusion, and extensive carious lesions are among the causes of pulpitis.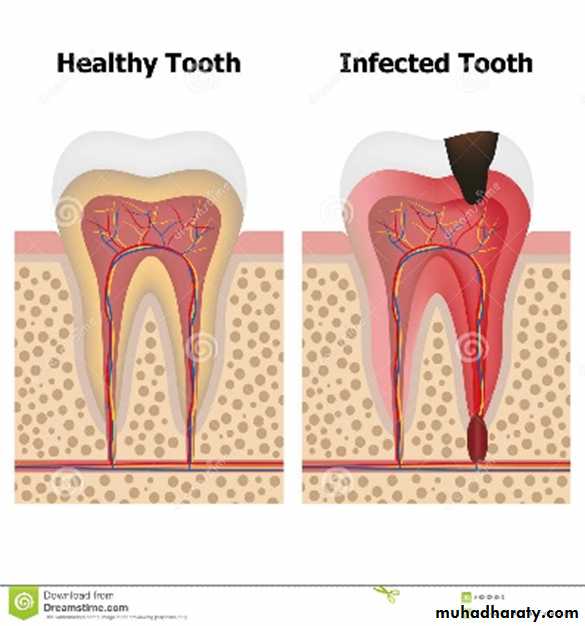
Pulpitis could be either:
Reversible, when elimination of the source of irritation is expected to promote resolution. Teeth with reversible pulpitis respond to stimulation by temperature extremes ( hot ,cold ) by mild pain sensation that abruptly stops after removal of the stimulus, but they are not spontaneously uncomfortable.Reversible pulpitis can progress in severity to become irreversible pulpitis if the source of irritation is not eliminated. Reversible pulpitis is treated by removal of the source of inflammation, placement of a sedative temporary restoration and palliation with systemic analgesics.
irreversible pulpitis, this could be either:
Acute pulpitis :
Extensive acute, inflammation of the dental pulp is a frequent immediate reversible pulpitis, although it may also occur as an acute of an existing chronic pulpitis .Acute pulpitis usually occurs in teeth with large carious lesions or restorations.
not uncommonly defective. Even in its early stages, when the inflammatory process involves only a portion of the pulp, relatively sever pain is elicited by thermal changes particularly cold, this pain characteristically persists long after the thermal stimulus has been removed and spontaneous pain is not uncommon.
As a greater portion of the pulp becomes involved, the pain may become even more sever often described as lancinating, it may be continuous and its intensity may increase when the patient lies down .Teeth are not sensitive to percussion until the inflammatory process extends to the periapical periodontal ligament.
there is no successful treatment of an acute pulpitis involving most of the pulp capable of preserving the pulp and teeth involved may either be root canal filled or extracted.
Chronic pulpitis :
Chronic pulpitis may arise through quiescence of a previous acute pulpitis, but more frequently it occurs as the chronic type of the disease from the onset. As in most chronic inflammatory conditions, the signs and symptoms are considerably milder than those in the acute form of the disease.Pain is not a prominent feature in chronic pulpitis, although some times the patient complains of a mild, dull ache, which is more often intermittent than continuous. The reaction to thermal changes is significantly reduced in comparison to that in acute pulpitis because of the degeneration of nerve tissue in the affected pulp occurring over a prolonged period of inflammation. Treatment of chronic pulpitis does not differ dramatically from that of acute pulpitis.
PAIN ORIGINATING FROM THE PERIODONTIUM :
Periapical inflammation secondary to pulp necrosis :Acute apical periodontitis usually arises as a result of infection spread to the apical periodontal ligament following pulp infection and necrosis, but it also occurs after traumatic injury to the teeth, and in cases of irritation to the periapical tissues either by mechanical manipulation or by the application of chemicals in endodontic procedures. Occasionally the condition develops in the area of an existing chronic infection, the periapical granuloma.
The pain in this case is sever, spontaneous, and continuous with tenderness to pressure and percussion applied to the affected teeth. Examination reveals that single canal teeth are usually unresponsive to thermal or electrical stimulation, though occasionally heat can dramatically increase pain. Teeth with multiple canals may demonstrate different stages of pulpal degeneration in each canal a fact which can complicate diagnosis
Periodontal ( paradental ) abscess:
Periodontal abscesses are associated with poorly localized dull pain, adjacent teeth are tender, clenching the teeth, which are usually vital, characteristically brings relief. Mobility of teeth, pathologic sinuses, and evidence of periodontitis are often present
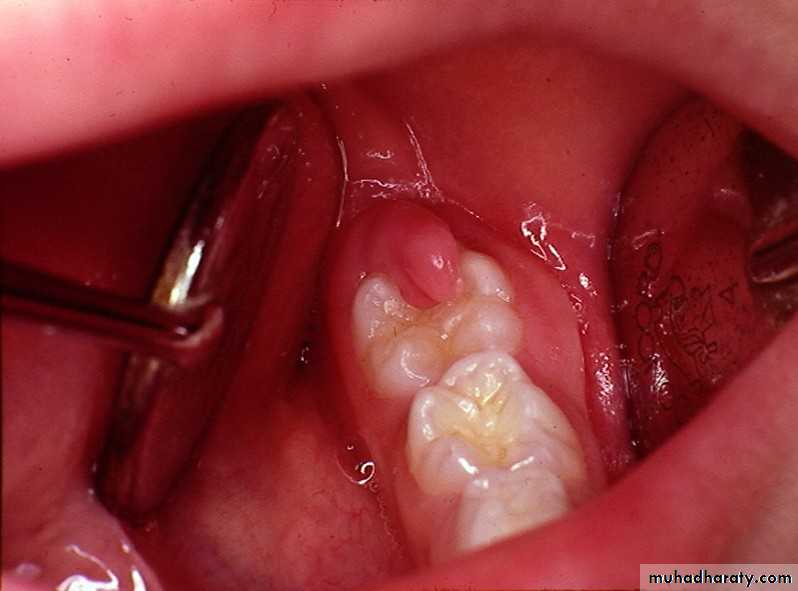
Pericoronitis :
Pericoronitis produces rapid onset of soreness or pain in the soft tissues surrounding the crown of a partially irrupted tooth.In the case of impacted third molars particularly the lower ones this soreness is a associated with pain on swallowing and trismus these symptoms are particularly sever in cases of acute pericoronitis. Subacute pericoronitis Is also associated with soreness, pain on swallowing, and trims but their degree severity is milder than that of the acute phase of the disease.


Occlusal trauma :
Excessive non-axial forces during functional and parafunctional contact of teeth can produce pain, tenderness and mobility of teeth due to overstretching of the periodontal ligament fibers.Pulpitis may also develop but the pulpal pain is usually mild when compared with the periodontal discomfort.

