INVESTIGATION OF
RESPIRATORY DISEASE

Imaging:
The 'plain' chest X-ray
Chest radiography is performed on the majority of patients
suspected of having chest disease.
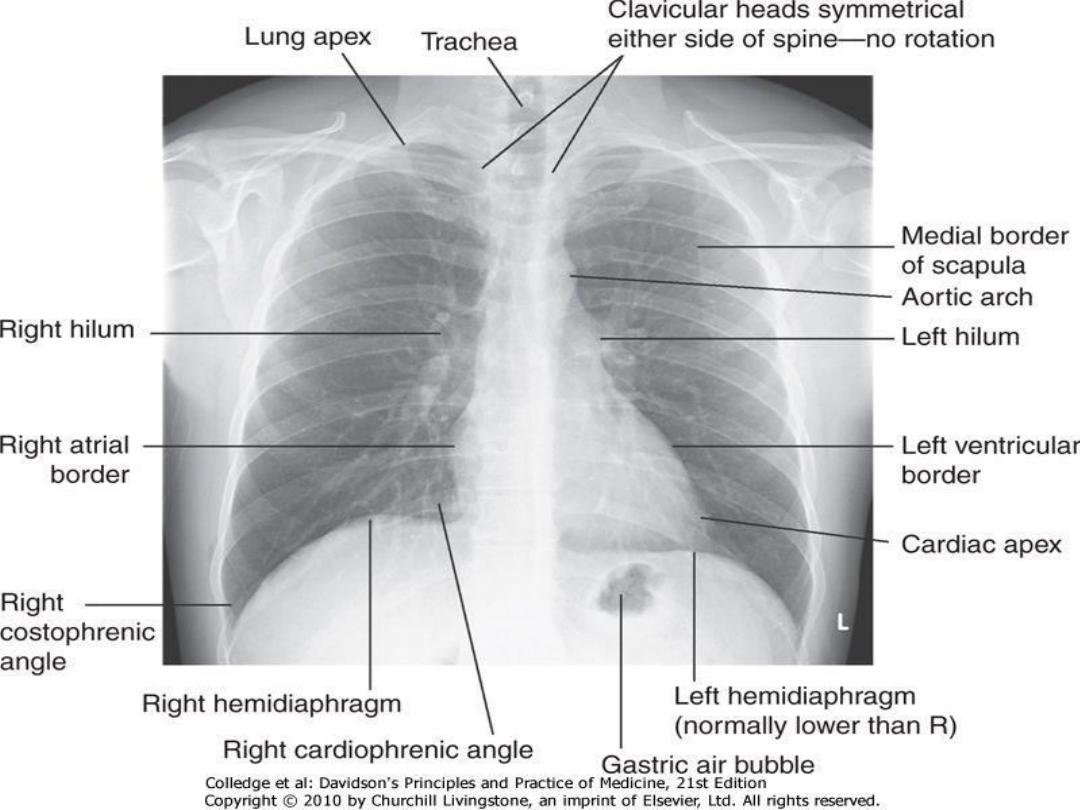
A postero-anterior (PA) film provides information on the lung
fields, heart, mediastinum, vascular structures and the
thoracic cage.
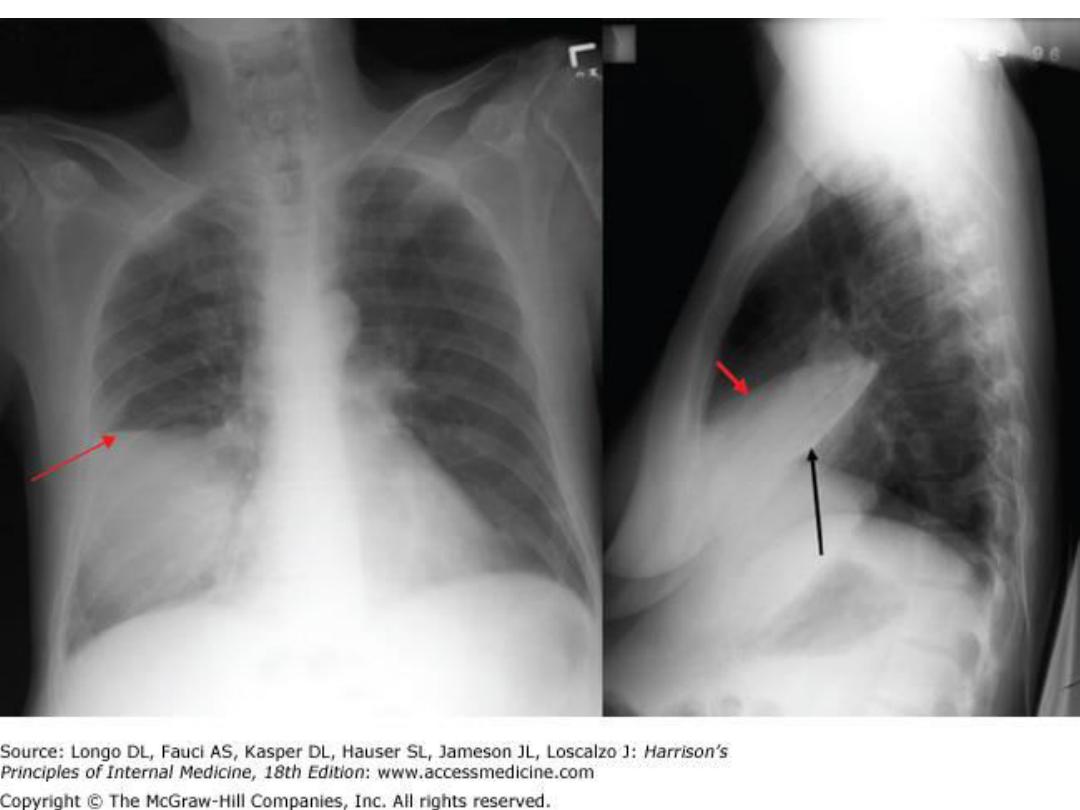
Additional information may be obtained from a lateral film,
particularly if pathology is suspected behind the heart
shadow or deep in the diaphragmatic sulci
.
COMMON CHEST X-RAY APPEARANCES
Pulmonary and pleural shadowing
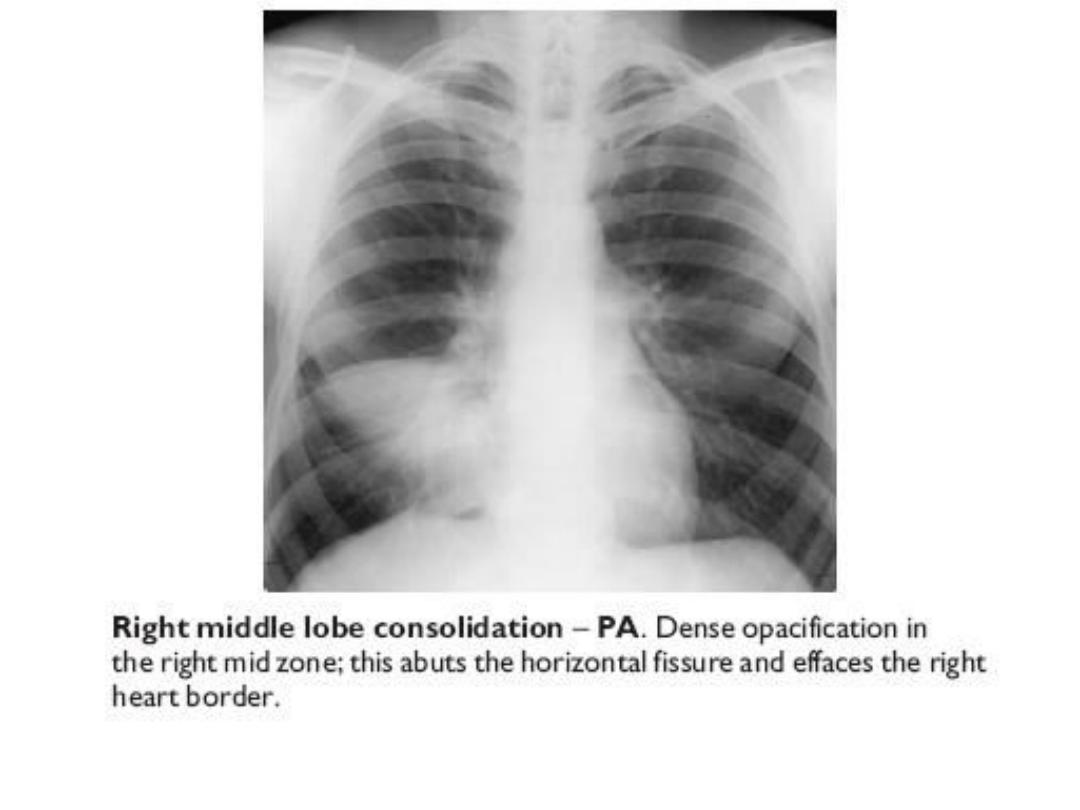
1. Consolidation
: infection, infarction, inflammation, and
rarely bronchoalveolar cell carcinoma
2. Lobar collapse
: mucus plugging, tumour, compression by
lymph nodes
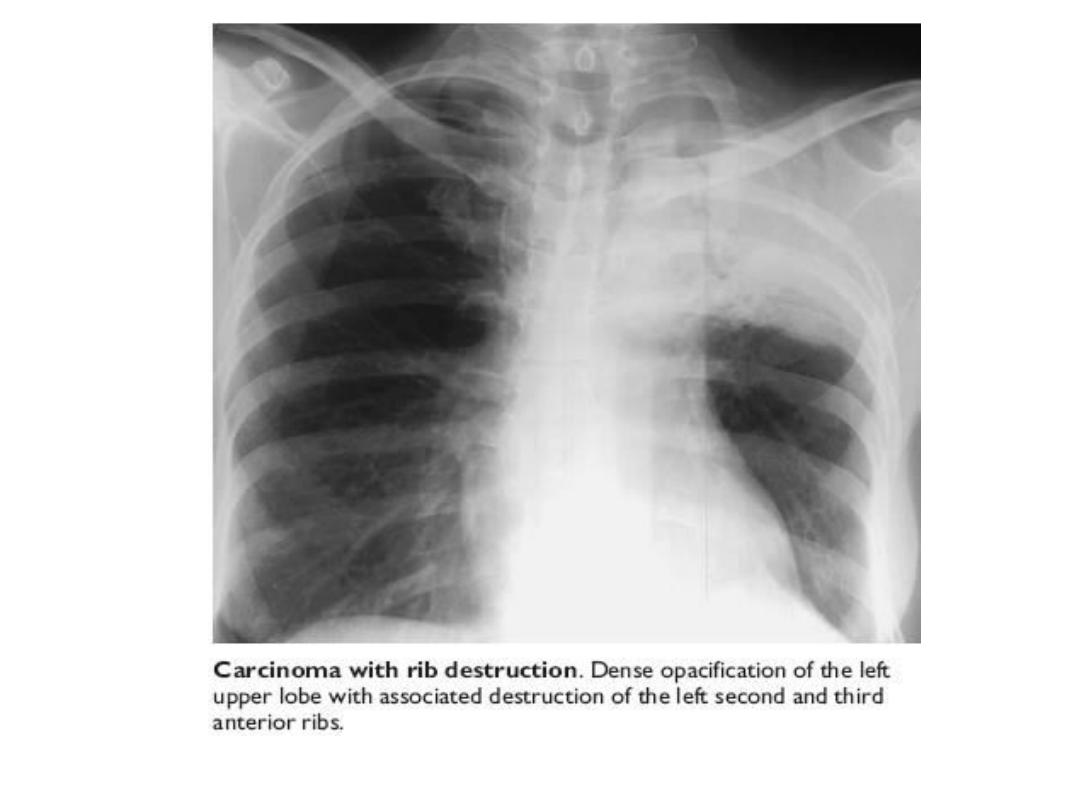
3. Solitary nodule:
4. Multiple nodules
: miliary TB, dust inhalation, metastatic
malignancy, healed varicella pneumonia, rheumatoid
disease
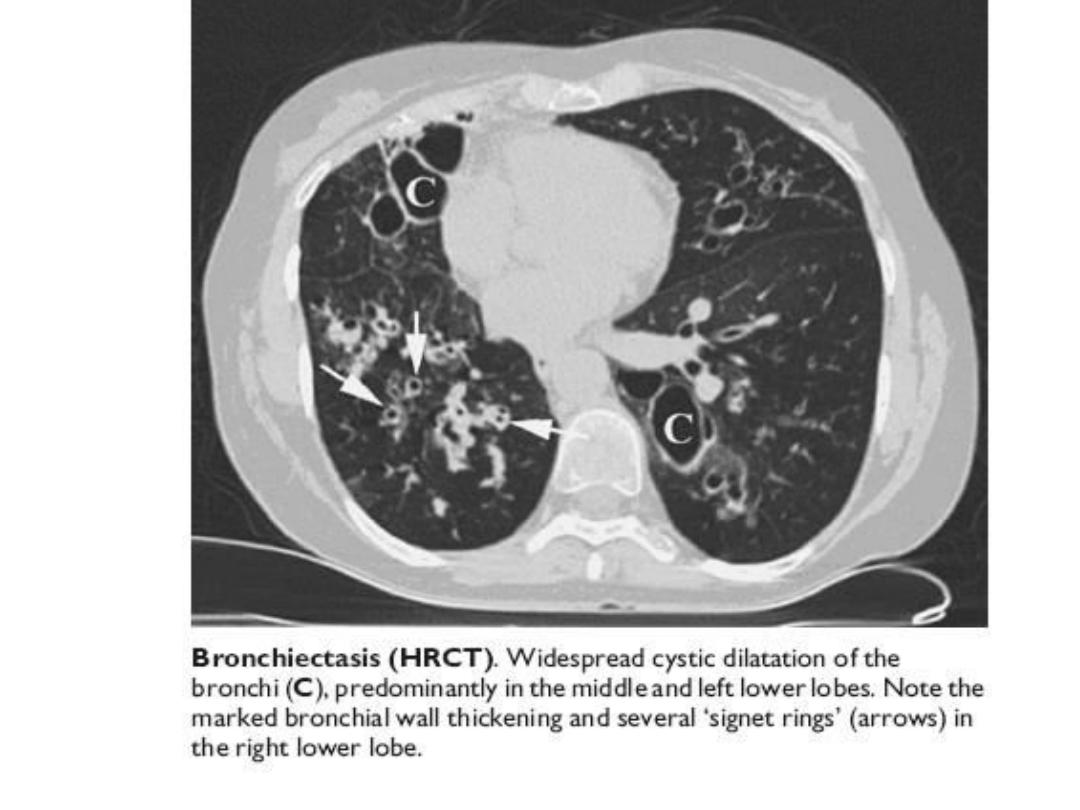
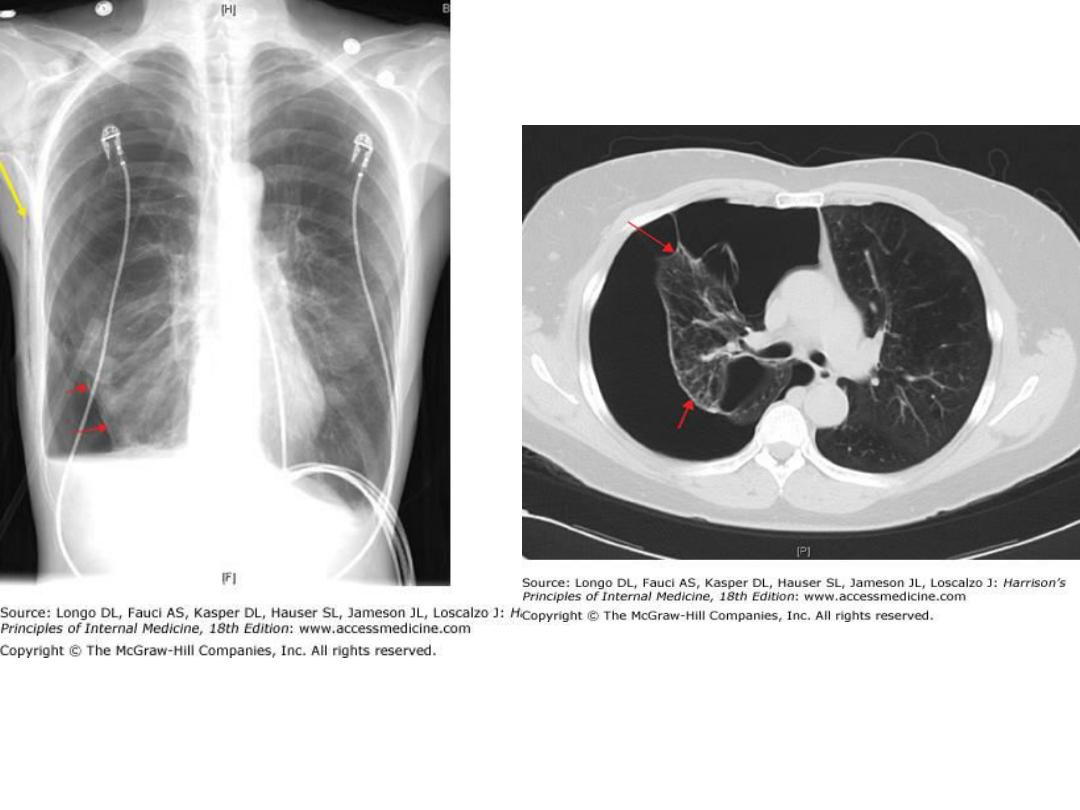
5. Ring shadows, tramlines and tubular shadows
:
bronchiectasis
6. Cavitating lesions
: tumour, abscess, infarct, pneumonia
(Staphylococcus/Klebsiella
,(
Wegener's granulomatosis.
7. Reticular, nodular and reticulonodular shadows
: diffuse
parenchymal lung disease infection.
8. Pleural abnormalities
: fluid, plaques, tumour

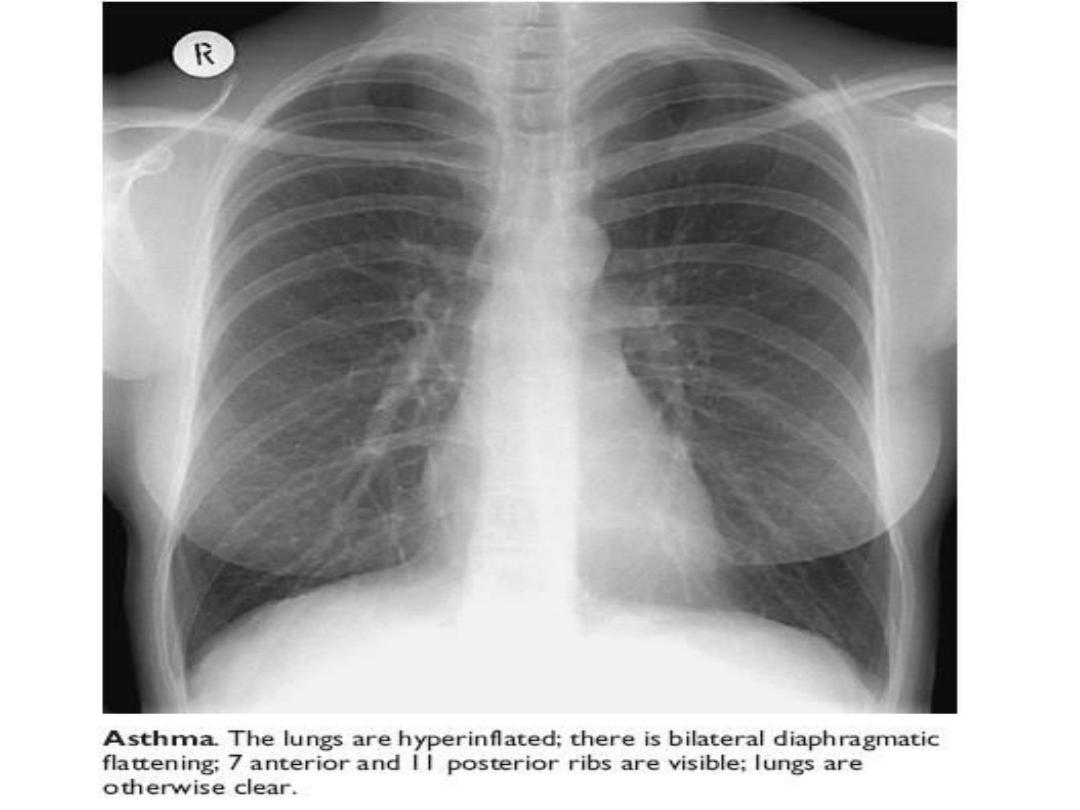
• Increased translucency
• Bullae
• Pneumothorax
• Oligaemia
• Hilar abnormalities
• Unilateral hilar enlargement: TB, bronchial
carcinoma, lymphoma
• Bilateral hilar enlargement: sarcoid, lymphoma, TB,
silicosis
• Other abnormalities
• Hiatus hernia
• Surgical emphysema

Increased shadowing may represent accumulation of
fluid, lobar collapse or consolidation.
Uncomplicated consolidation should not change the
position of the mediastinum and the presence of an
air bronchogram provides reassurance that proximal
bronchi are patent.
Collapse (implying obstruction of the proximal
bronchus)
is accompanied by loss of volume and
displacement of the mediastinum towards the
affected side
.

The presence of pleural fluid is suggested by a dense
basal shadow which, in the erect patient, ascends
towards the axilla.
In large pulmonary embolism relative oligaemia may
cause a lung field to appear abnormally dark.
Increased translucency is seen with emphysematous
bullae or a pneumothorax
.


Computed tomography (CT)
CT scanning provides detailed images of the pulmonary
parenchyma, mediastinum, pleura and bony structures.
The contrast can be altered to highlight different structures
such as the lung parenchyma, the mediastinal vascular
structures or bone.
Sophisticated software facilitates 3D reconstruction of the
thorax and virtual bronchoscopy
.
CT scanning is superior to chest radiography in determining
the position and size of a pulmonary lesion and whether
calcification or cavitation is present.
It is now routinely used in the assessment of patients with
suspected lung cancer and facilitates guided percutaneous
needle biopsy.
Information on tumour stage may be gained by examining the
mediastinum, liver and adrenal glands
.

High-resolution CT (HRCT) scanning
uses thin sections
to provide a detailed assessment of the pulmonary
parenchyma and is particularly useful in assessing
diffuse parenchymal lung disease,
identifying bronchiectasis
,
and assessing the type and extent of emphysema .