LIP
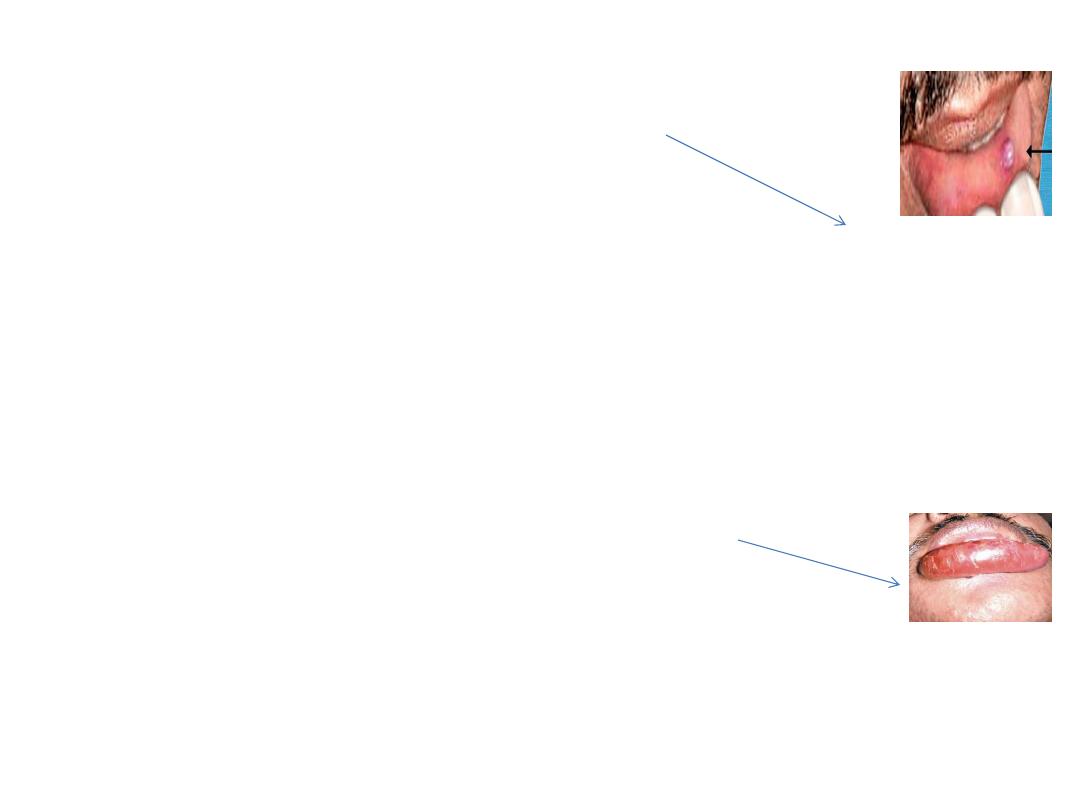
Mucous cyst of lip
is a common condition.
It can occur in upper or lower lip.
It is a retention cyst derived from mucous glands of the lip.
It presents as bluish, soft, fluctuant often transilluminating well
localized swelling.
It may resolve on its own.
If it does not it resolved,it should be excised under local
anaesthesia.
Macrocheilia
is enlargement of lip .
other swellings which can occur in lip.
*Lymphangioma.
*Haemangioma
,* inflammatory conditions.
*Papilloma, lipoma, pyogenic granuloma, keratoacanthoma, minor
salivary tumours

Cheilitis (inflammation of the lip)
• often associated with
stomatitis.
•
is common in vitamin deficiency, malnutrition, sepsis, drug induced,
RT induced presents as redness, pain, diffuse swelling.
In chronic cases, there will be linear ulcers especially at commissure.
Actinic cheilitis
is a premalignant lesion.
Pigmentation of lip occurs in;
* Peutz-Jeghers syndrome (brown),
*Addison’s disease la k .
Herpes labialis
is formation ulcers in lip due
to herpes simplex virus.
Repeated multiple ulcers develop in lip.
It is contagious by kissing.
Touching repeatedly can transfer the virus
to eye causing herpes keratitis.

NEOPLASM OF LIP
Minor salivary gland tumours are common in upper lip.
They are usually pleomorphic adenomas.
CARCINOMA LIP-
It is common after 40 years of age.
It may arise from vermilion surface or mucosa part of the lip.
In younger age group even though it is rare, carries poor outcome.
It is more common in whites; rare in blacks. It is common in Caucasians.
Verrucous carcinoma ;-
It is well differentiated squamous cell carcinoma
with exophytic, warty, dry surface. It carries good prognosis.
It is common in men. Common in lower lip.
Commonly due to exposure to sunlight. Common in pipe smokers.
Initially starts as a red, granular dry lesion which eventually gets ulcerated
and forms an ulceroproliferative lesion.
It spreads to submental nodes and later to other neck nodes on both sides.
Predisposing Factors;-1.
Cheilitis
—actinic type. 2. Solar keratosis.
3. Papilloma. 4. Leukoplakia. 5. Smoking. 6. Ultra-Violet rays.

Clinical features of carcinoma lip
1- Painless ,Non-healing progressive ulcer.
2- Everted edge with indurations , Growth moves with the lip
3- Submental, submandibular and upper deep neck nodes may get enlarged.
4- Fungation, bleeding, halitosis.
Differential Diagnosis
*Keratoacanthoma. *Basal cell carcinoma. *Malignant melanoma .
*Minor salivary gland tumours.
* Pyogenic granuloma in early cases only.
Diagnosis ;- *
Edge biopsy,
*FNAC” Fine needle aspiration cytology” of lymph nodes.
Treatment
1- If lesion is less than 2 cm, then curative radiotherapy, either brachytherapy
or external beam radiotherapy. It gives a good cure.
2- If tumour is more than 2 cm, wide excision is done.( Excision of more than
one-third of the lip requires reconstruction using different flaps).
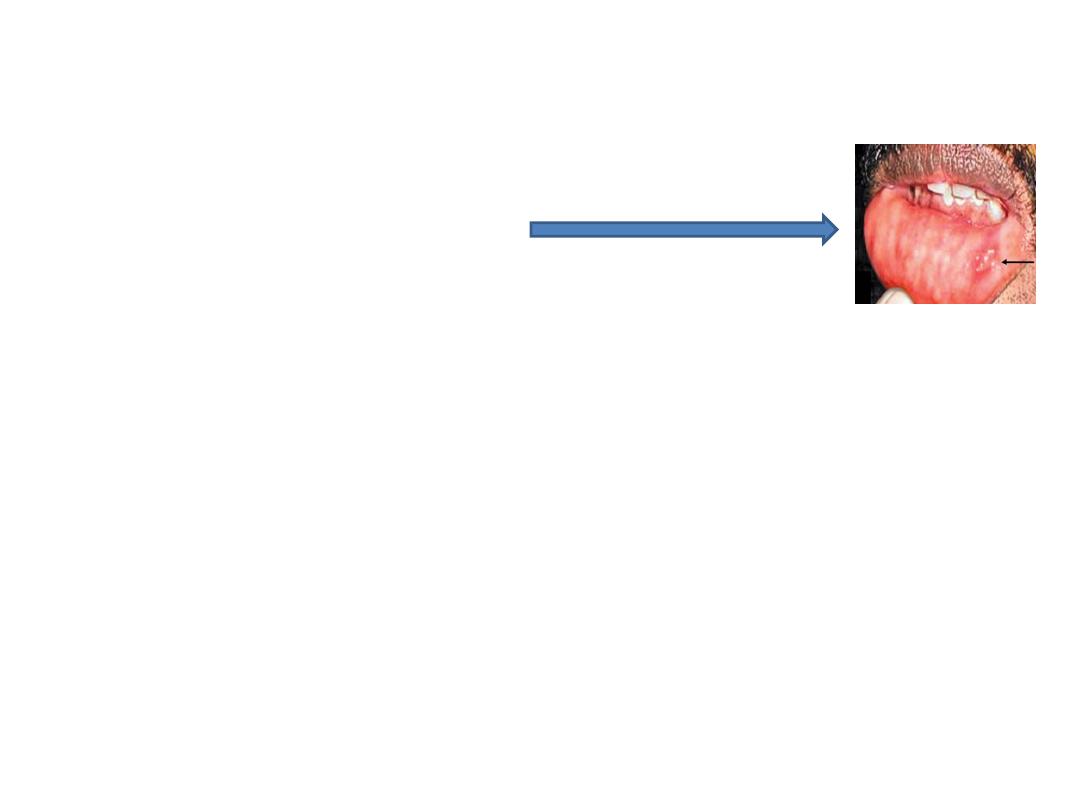
TONGUE ULCERS
Differential diagnosis for tongue ulcers
1-Painful ( Dental
— Aphthous ).
2- Painless (Ulcers in lichen planus
— Syphilitic –Malignant).
Aphthous Ulcer ;-
types-
(1)
Minor aphthous ulcer, common in menstruating women
as a crop with painful, round, yellow based ulcer with red margin.
It regresses spontaneously in 2 weeks.
(2)
Major aphthous ulcer, large and deep which often becomes chronic and Takes
more time to subside with a scar.
Chlorhexidine gluconate, local application of triamcinolone acetate,
choline salicylate gel are different local applicants used to promote healing.
(3)
Behcet’s syndrome is genital ulcer, conjunctival ulcer and multiple oral ulcers.
Dental Ulcer;-
1.
It is common on sides of tongue due to sharp tooth, denture, and broken tooth.
2.
Usually it is acute painful, self limiting ulcer.
Occasionally repeated trauma form an indolent chronic ulcer which mimic
carcinoma; it should be excised to rule out carcinoma and to cure the ulcer.
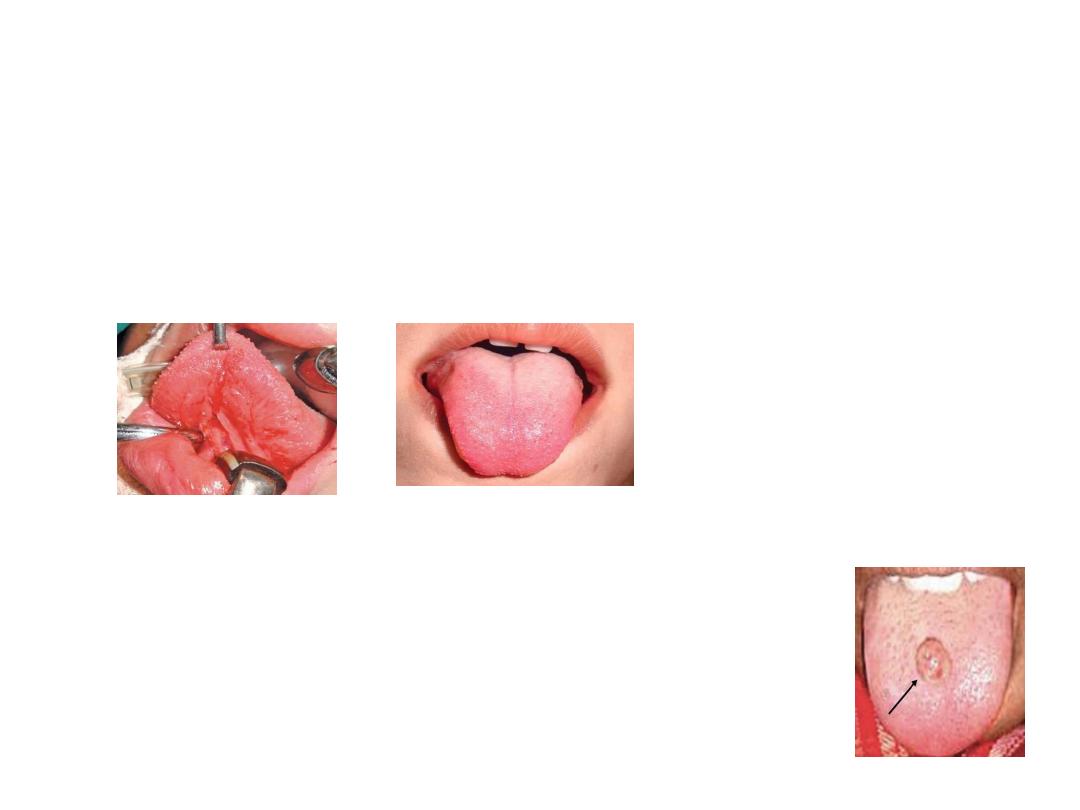
TONGUE TIE
It is short, thick, fibrous frenum linguae.
During protrusion lateral margin and tip of the tongue is everted with dorsal
mid part heaping.
It causes speech defect, difficulty in cleaning the inner part of lower teeth.
It is treated surgically under local anaesthesia (or general in child).
BENIGN TUMOURS OF TONGUE
*Papilloma
* Fibroepithelial polyp
* Haemangioma and lymphangioma
* Neurofibroma *Lipoma * Granular cell myoblastoma
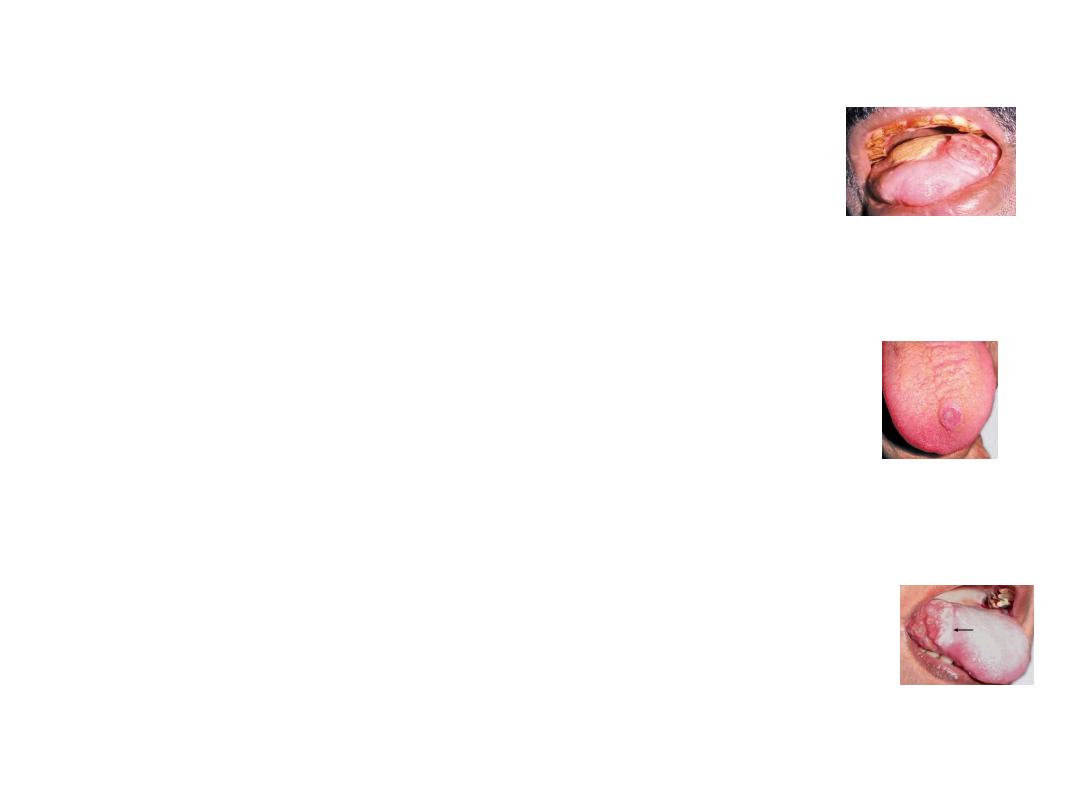
CARCINOMA OF THE TONGUE
* its incidence is increasing in females due to increase
in number of female smokers.
Aetiology;-
1- Leukoplakia. 2- Erythroplakia.
Types;-
1. Papillary.
2. Ulcerative or ulceroproliferative .
3. Fissure with induration.
4. Lobulated, indurated mass
—frozen tongue.
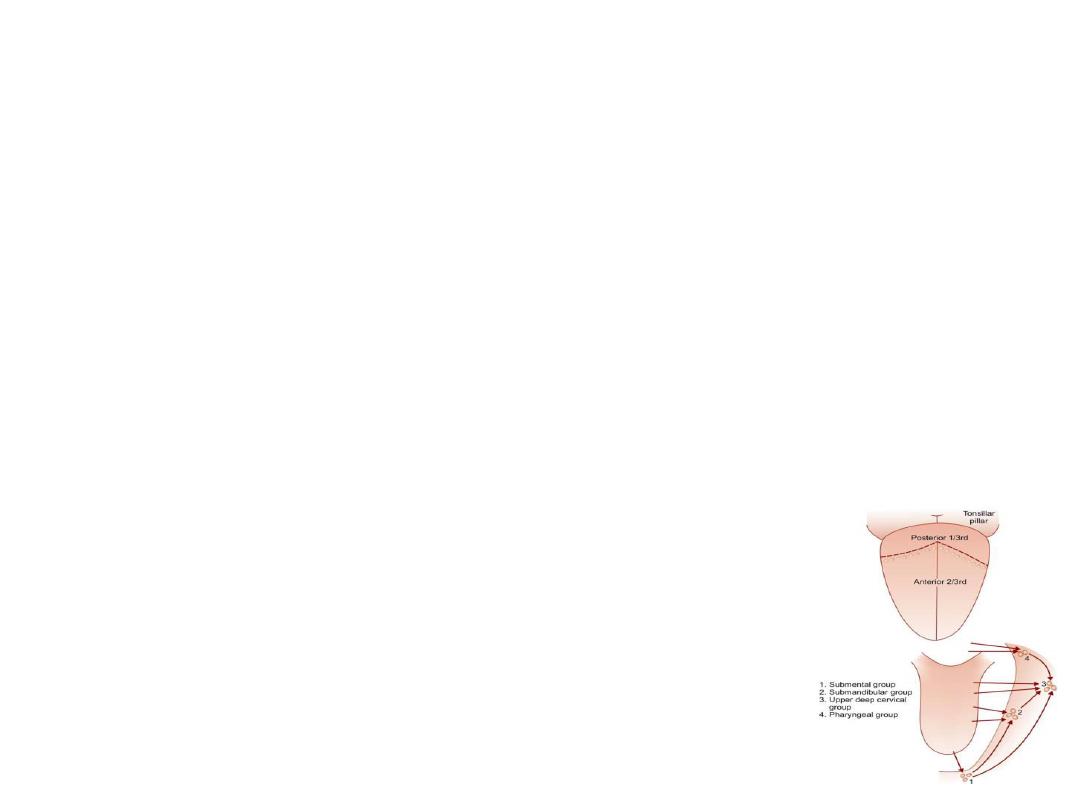
Sites;-
1.Lateral margin(commonest).
2. Posterior third.
3. Dorsum.
4. Ventral surface.
5. Tip.

Clinical Features
1- Painless ulcer/swelling in the tongue which later may become
painful.
2-Pain in the tongue due to infection or ulceration or due to the
involvement of lingual nerve (pain is referred to ear).
Pain on swallowing, in case of carcinoma of posterior third of tongue.
3- Excessive salivation. Saliva is often blood stained.
4-Dysphagia either due to fixed tongue or due to the involvement of
genioglossus or growth in the posterior third of the tongue.
5- Visible ulcer in anterior two-thirds of tongue.
I.
Ulcer can bleed on touch; edge, base and surrounding areas are indurated.
II.
Edge is everted commonly.
III. Ulcer may cross the midline ; may extend into the floor of the
mouth/alveolus/mandible.
IV. Growth or ulcer in posterior third, is usually not visible.
Investigations
1. Edge biopsy. 2. FNAC of lymph nodes.
3. Indirect and direct laryngoscopy to see posterior third growth.
4. CT scan ./ MRI is also very useful to assess the extent of primary tumour.
5. Chest X-ray (bronchopneumonia).
Spread of Carcinoma Tongue
Local spread:
In case of anterior two-thirds of tongue, the spread occurs to
genioglossus muscle, floor of the mouth, opposite side and mandible.
In case of posterior third of tongue it spreads locally to tonsil,
side of pharynx, soft palate, epiglottis, larynx and cervical spine.
Lymphatic spread:
1- sub mental nodes. Submandibular , later to deep cervical
lymph nodes.
2-From posterior third it spreads to pharyngeal nodes and
upper deep cervical lymph nodes.
Treatment=
Surgery, radiotherapy, chemotherapy.