FRACTURES OF THE OLECRANON
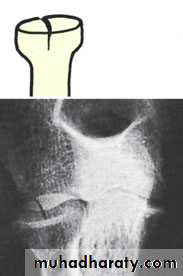
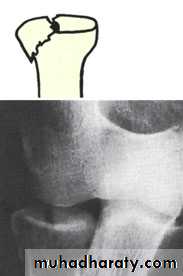
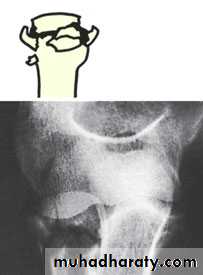
Two broad types of injury are seen: (1) a comminutedfracture which is due to a direct blow or a fall on the
elbow; and (2) a transverse break, due to traction
when the patient falls onto the hand while the triceps
muscle is contracted. These two types can be further
sub-classified into (a) displaced and (b) undisplaced
fractures. More severe injuries may be associated also
with subluxation or dislocation of the ulno-humeral
joint.
Clinical features
A graze or bruise over the elbow suggests a comminutedfracture; the triceps is intact and the elbow can
be extended against gravity. With a transverse fracture
there may be a palpable gap and the patient is unable
to extend the elbow against resistance.
X-ray



Treatment
1-A comminuted fracture with the triceps intact should be treated as a severe ‘bruise’. Many of these patients are old and osteoporotic, and immobilizing the elbow will lead to stiffness. The arm is rested in a sling for a week; a further x-ray is obtained to ensure that there is no displacement and the patient is then encouraged to start active movements.2-An undisplaced transverse fracture that does notseparate when the elbow is x-rayed in flexion can be treated closed. The elbow is immobilized by a cast in about 60 degrees of flexion for 2–3 weeks and then exercises are begun. Repeat x-rays are needed to exclude displacement.
3-Displaced transverse fractures can be held only by splinting the arm absolutely straight – but stiffness in that position would be disastrous. Operative treatment is therefore strongly recommended. The fracture is reduced and held by tension band wiring. Oblique fractures may need a lag screw, neutralised by a tension band system or plate.
Complications
1-Stiffness used to be common, but with secure internal fixation and early mobilization the residual loss of movement should be minimal.2-Non-union sometimes occurs after inadequate reduction and fixation. If elbow function is good, it can be ignored; if not, rigid internal fixation and bone grafting will be needed.
3-Ulnar nerve symptoms can develop. These usually settle spontaneously.
4-Osteoarthritis is a late complication, especially if
reduction is less than perfect. This can usually be treated symptomatically.
FRACTURED HEAD OF RADIUS
Radial head fractures are common in adults but are hardly ever seen in children (probably because the proximal radius is mainly cartilaginous) whereas radial neck fractures occur in children more frequently.
Mechanism of injury
A fall on the outstretched hand with the elbow extended and the forearm pronated causes impaction of the radial head against the capitulum.Clinical features
This fracture is sometimes missed, but tenderness on pressure over the radial head and pain on pronation and supination should suggest the diagnosis.X-ray
Three types of fracture are identified and classified by Mason as:Type I An undisplaced vertical split in the radial head.
Type II A displaced single fragment of the head.
Type III The head broken into several fragments (comminuted).
Treatment
1-An undisplaced split (Type I) Worthwhile pain relief can be achieved by aspirating the haematoma and injecting local anaesthetic. The arm is held in a collar and cufffor 3 weeks; active flexion, extension and rotation are encouraged.
2-A single large fragment (Type II) If the fragment is displaced, it should be reduced and held with one or two small headless screws.
3- A comminuted fracture (Type III) This is a challenging injury. Always assess for an associated soft tissue injury: Rupture of the medial collateral ligament; Rupture of the interosseous membrane (Essex
Lopresti lesion); Combined fractures of the radial head and coronoid process plus dislocation of the elbow – the ‘terrible triad’.
If any of these is present, excision of the radial head is contra-indicated; this may lead to intractible insta - bility of the elbow or forearm.
The head must be meticulously reconstructed with small headless screws or replaced with a metal spacer. A medial collateral rupture, if unstable after replacing or fixing the radialhead, sh ould be repaired.
Radial head excision usually gives a good long-term result if there are no contra-indications; however,
wrist pain from ulnar head impaction, valgus instability
of the elbow and trochleo-olecranon arthritis can develop.
Complications
1- Joint stiffness is common and may involve both theelbow and the radioulnar joints. Even with minimally
displaced fractures the elbow can take several months
to recover, and stiffness may occur whether the radial
head has been excised or not.
2-Myositis ossificans is an occasional complication.
3- Recurrent instability of the elbow can occur if the
medial collateral ligament was also injured and the
radial head excised