د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
1
NECK SURGERY
ANATOMY OF LYMPHATICS OF HEAD AND NECK
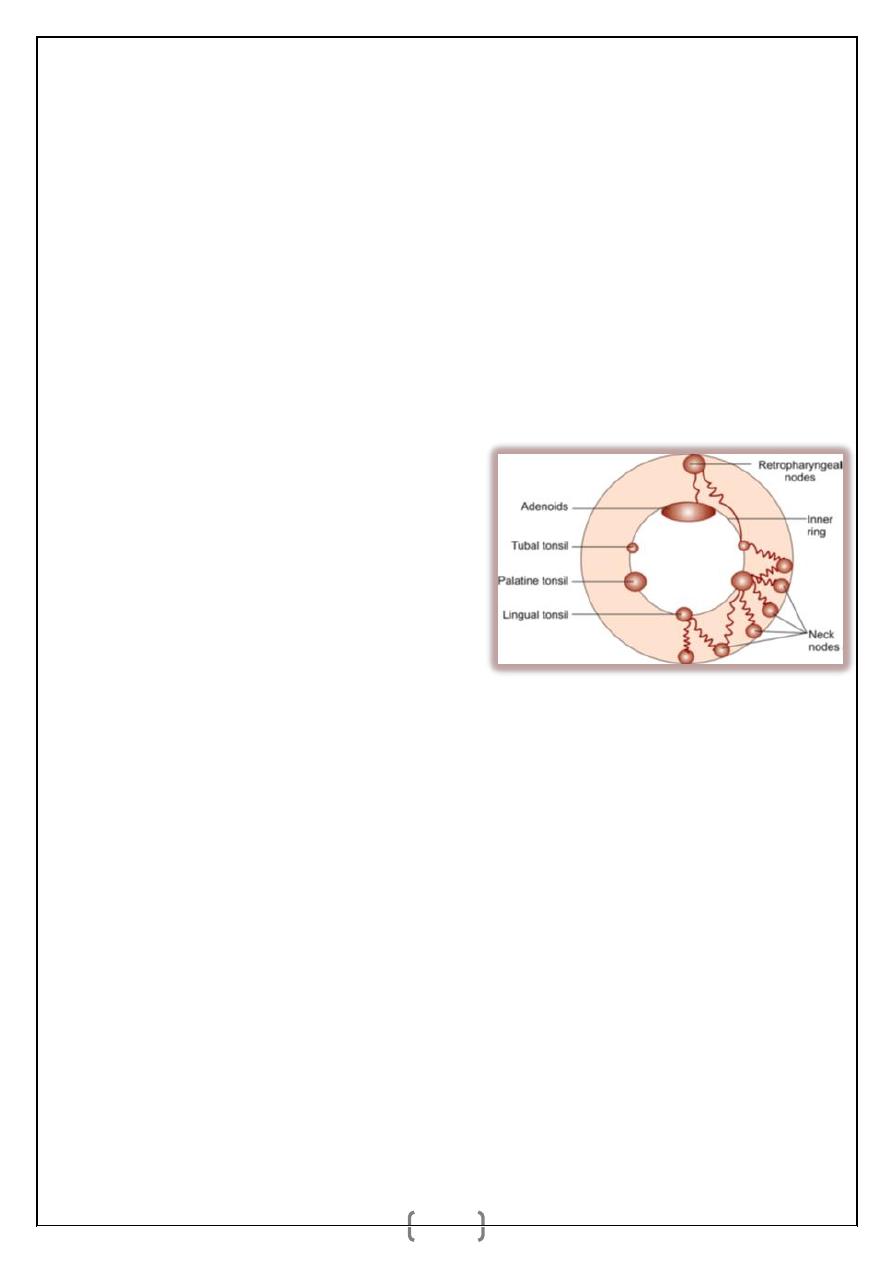
Waldeyer’s Lymphatic Ring (Inner)
It consists of adenoids above, lingual tonsils below and two palatine tonsils
laterally one on each side.
Outer Circular Chain of Nodes (Outer Waldeyer’s Ring)
Occipital, postauricular, preauricular, parotid, facial, submandibular, submental,
superfi cial cervical and anterior cervical.
Facial nodes are:
a. Superficial
_ Upper—infraorbital.
_ Middle—buccinator.
_ Lower—supramandibular.
b. Deep groups—in relation to pterygoids.
Submandibular lymph nodes drain
(Inner and outer Waldeyer‘s ring anatomy)
_ The side of the nose.
_ The cheek.
_ Angle of the mouth.
_ Entire upper lip.
_ Outer part of the lower lip.
_ The gums.
_ Side of the tongue.
Submental lymph nodes: Drain from the central part of the lower lip, floor of the
mouth and apex of the tongue.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
2
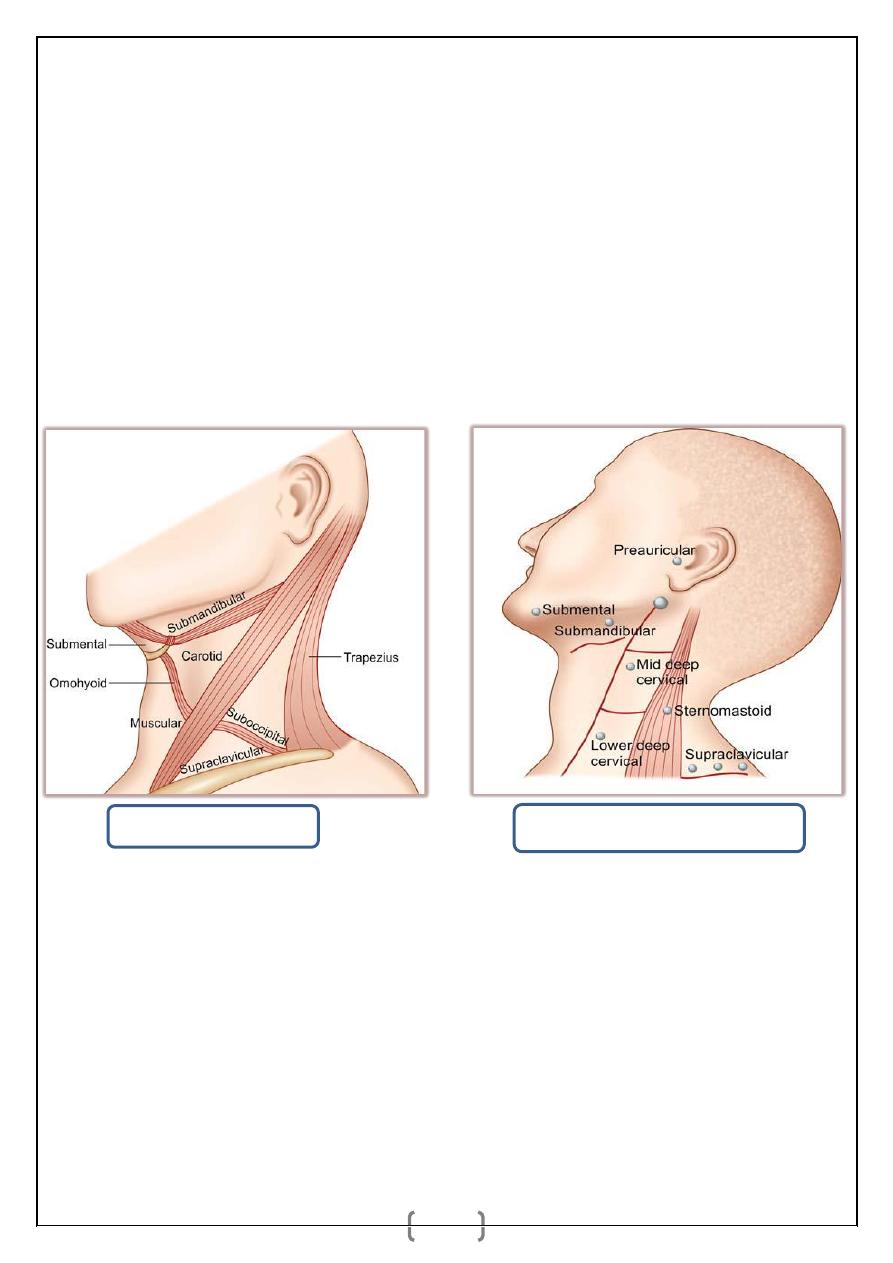
Superficial cervical nodes: They lie on outer surface of the sternomastoid around
the external jugular vein. They drain the parotid region and lower part of the ear.
Deep cervical lymph nodes: Upper deep cervical lymph nodes—jugulodigastric
nodes Below the digastric and in front of IJV.
Lower deep cervical lymph nodes—jugulo-omohyoid nodes—Above the
omohyoid and behind the IJV. They drain the ipsilateral half of head and neck,
finally form a jugular lymph trunk from lower deep cervical nodes to join
thoracic duct on the left side, and the junction of right subclavian and right
jugular vein on right side.
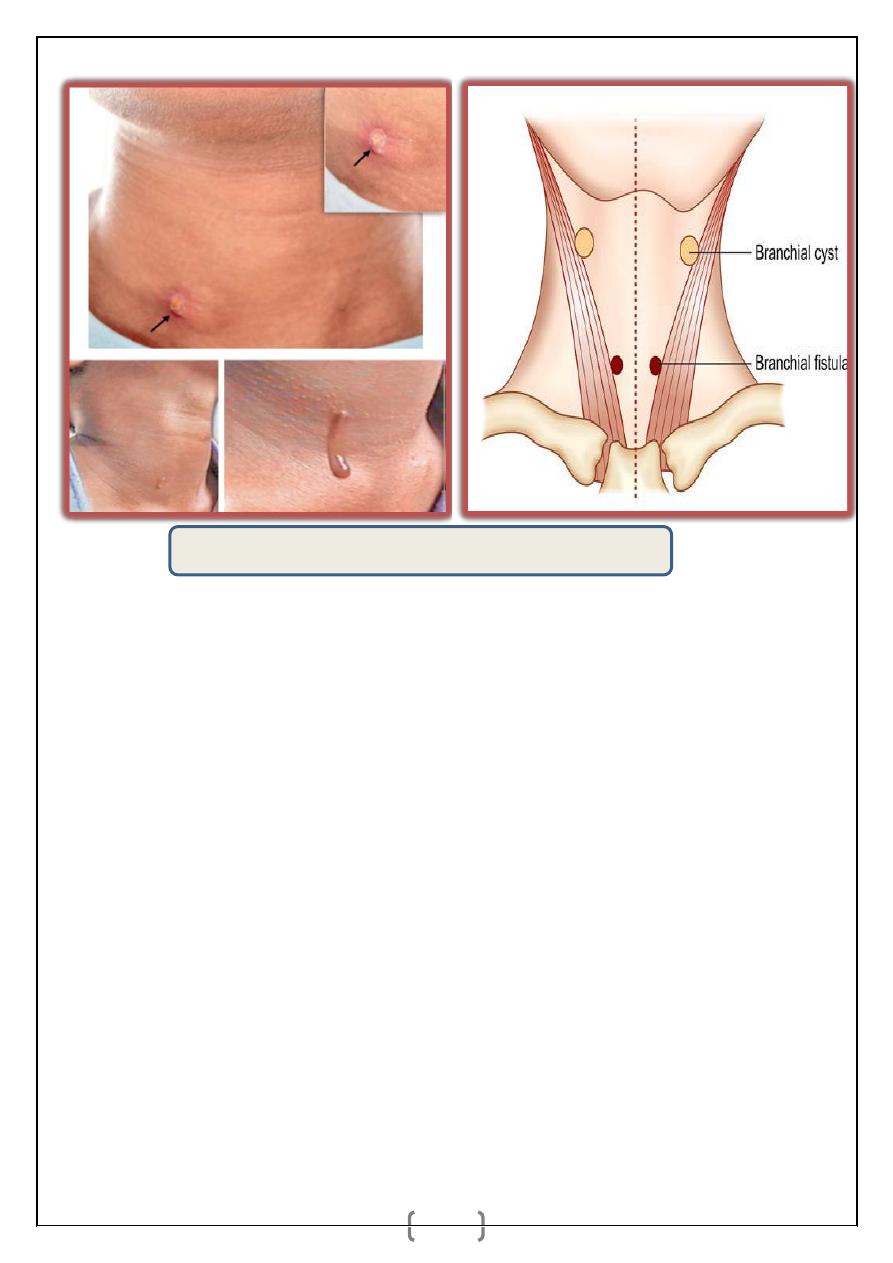
BRANCHIAL CYST
It arises from the remnants of second branchial cleft. Normally 2nd, 3rd, 4th
clefts disappear to form a smooth neck. Persistent 2nd cleft is called as cervical
sinus (of His) which eventually gets sequestered to form branchial cyst.
Epithelial infusion within lymph node may be the other cause as branchial cyst
contains lymphoid tissues in their wall. Six branchial arches with five pharyngeal
pouches (endoderm lining) inside and five pharyngeal clefts (ectoderm lining)
outside are present.
(Lymphatic drainage of the neck)
(Triangles of the neck)
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
3
Features
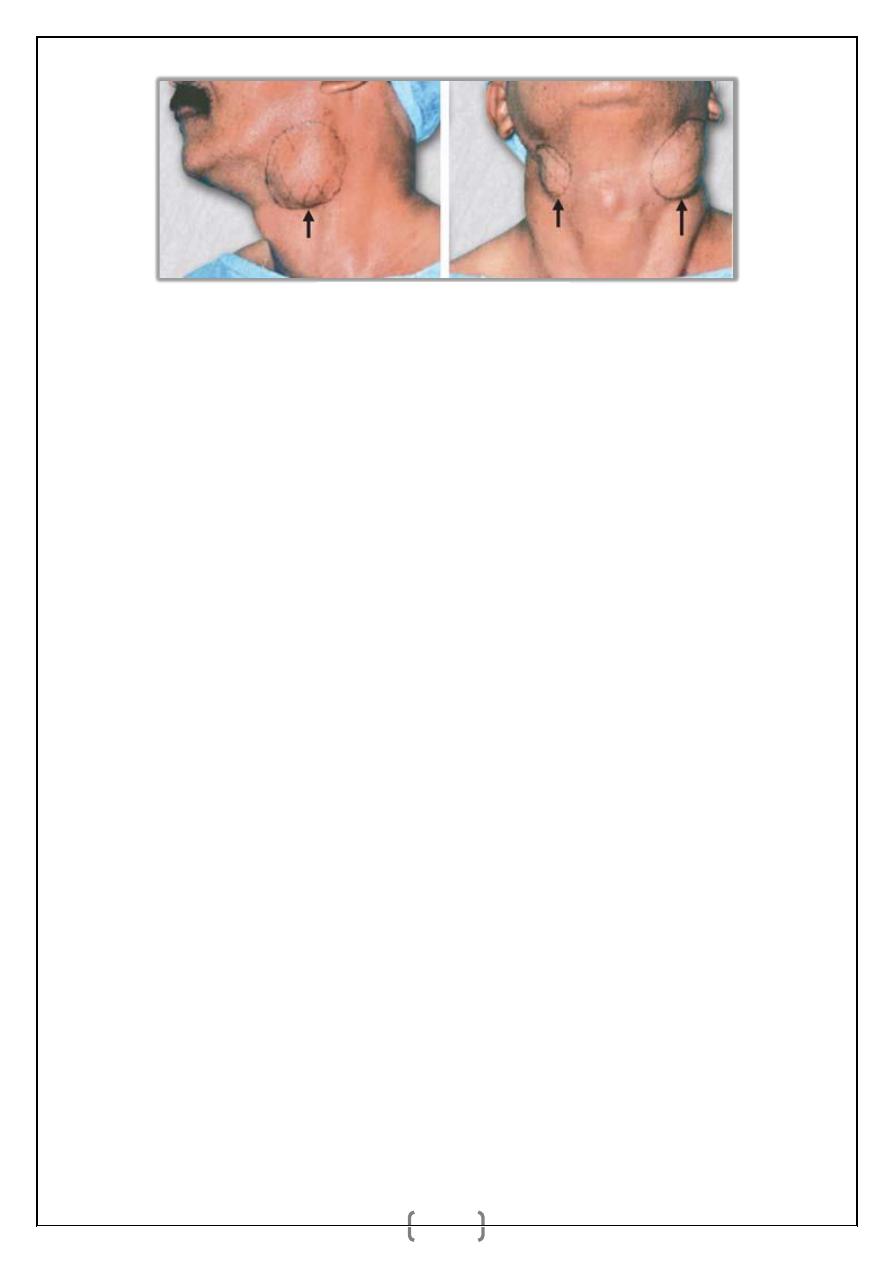
_ Swelling in the neck beneath the anterior border of upper third of the
sternomastoid muscle. It is smooth, soft, fluctuant, often transilluminant with a
sensation of ‘Half-filled double hot water bottle’.
_ It is equal in both sexes. Even though congenital, it is seen in late adolescents
and early 3rd decade.
_ Usually painless unless it is infected.
_ It contains cholesterol crystals which is from the lining of mucous membrane
which contains sebaceous gland. Cheesy toothpaste like material is typical
_ Histologically, it is lined by squamous epithelium. Occasionally it contains
ciliated columnar epithelium. Cyst wall shows plenty of lymphoid tissue.
_ It may get infected to form an abscess.
_ FNAC shows cholesterol crystals.
Complications
_ Recurrent infection.
_ Rupture may cause acquired branchial fistula at upper third of
sternocleidomastoid muscle.
Differential Diagnosis
1. Cold abscess, lipoma neck.
2. Lymph cyst.
3. Chronic lymphadenitis.
Branchial cyst—both sides.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
4
Treatment: Excision under G/A.
Cyst is in relation to carotids, hypoglossal nerve, glossopharyngeal nerve, spinal
accessory nerve, posterior belly of digastric and pharyngeal wall. Medially it is
close to the posterior pillar of tonsils. During dissection, all these structures
should be taken care of.
Complications of Surgery
_ Injury to major structures.
_ Infection.
_ Recurrence/fistula formation due to incomplete removal of the track.
BRANCHIAL FISTULA
Branchial fistula is commonly a congenital lesion. It is due to persistent
precervical sinus between 2nd branchial cleft and 5
th
branchial cleft having
opening in the skin at lower 1/3rd of neck on the inner margin of
sternocleidomastoid muscle, often ends as a sinus just proximal to the posterior
pillar of fauces behind tonsil which is also the site of inner opening when
presents as fistula.
Fistula runs between the structures related to 2nd and 3rd branchial arches (2nd
arch artery is ECA, nerve is facial; 3rd arch artery is ICA, nerve
glossopharyngeal). From external opening at skin below, it runs in subcutaneous
plane to pierce deep fascia at level of thyroid cartilage; to travel between ECA
and ICA; behind posterior digastric belly and stylohyoid; outer to IJV,
stylopharyngeus, hypoglossal and glossopharyngeal nerves; perforates superior
constrictor to reach the internal opening.
Occasionally acquired branchial fistula can occur due to rupture of or after
drainage of infected branchial cyst or incomplete excision of the cyst track. This
type of fistula is located outside at skin at the level of upper third of
sternomastoid muscle.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
5
Clinical Features
_It usually presents at birth. It is common in children and early adolescent
period. Equal in both sexes.
_ Often it is bilateral (30%).
_ External orifice of the fistula is situated in the lower third of the neck near the
anterior border of the sternomastoid muscle.
_ External orifice is very small with a dimple which becomes more prominent on
dysphagia with tuck in appearance.
_ Discharge is mucoid or mucopurulent.
_ Internal orifice is located on the anterior aspect of the posterior pillar of the
fauces, just behind the tonsils.
_ Sometimes fistula ends internally as blind end.
Histopathology: Track is lined by ciliated columnar epithelium with patches of
lymphoid tissues beneath it, causing recurrent inflammation.
Investigations: Discharge study, fistulogram, MR/CT fistulogram.
Positions of branchial cyst and fistula.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
6
Treatment
Always surgery:
_ Under general anaesthesia, methylene blue is
injected into the track. Probe is passed into the
fistulous track. Through circumferential/elliptical
incision around the fistula opening,
entire length
of the track is dissected until the internal orifice.
Care should be taken to safeguard carotids,
jugular vein, hypoglossal nerve, glossopharyngeal
nerve and spinal accessory nerve. Entire track
should be excised.
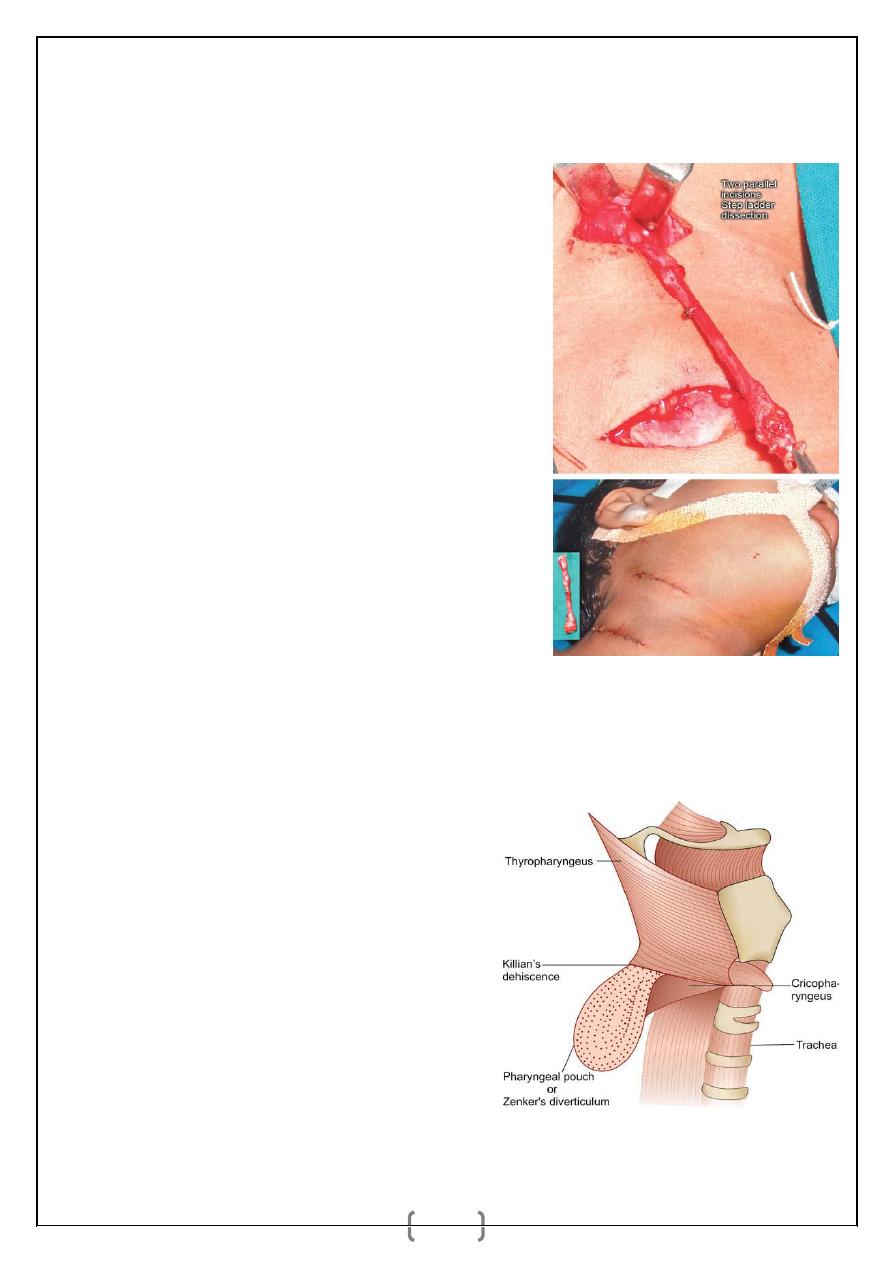
_ Step ladder dissection is done using two parallel
incisions one below at lower part another above at
upper part of the neck, will make dissection easier
and complete.
PHARYNGEAL POUCH
_ It is a protrusion of mucosa through Killian’s
dehiscence, a weak area of the posterior pharyngeal wall between
thyropharyngeus (oblique fibres) and cricopharyngeus (transverse fibres) of the
inferior constrictor muscle of the pharynx.
_
Thyropharyngeus
is
supplied
by
pharyngeal plexus from cranial accessory
nerve. Cricopharyngeus is supplied by
external laryngeal nerve.
_
Pharyngeal
pouch
is
a
pulsion
diverticulum. It starts in the midline of
posterior pharyngeal wall. Once it expands
and reaches the vertebra, it deviates towards
left side of the neck because of resistance of
vertebra.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
7
_ Imperfect relaxation of the cricopharyngeus increases the pressure in the
pharynx, mainly during swallowing which leads to protrusion of mucosa through
the Killian’s dehiscence causing pharyngeal pouch. The protrusion is usually
towards left.
Clinical Features
_ Pain, dysphagia, recurrent respiratory infection, swelling in the neck on the left
side which is smooth, soft and tender.
_ Regurgitation during night while turning neck, smooth, soft, tender swelling in
the posterior triangle of the left side of the neck; typical gurgling noise while
swallowing—are typical features. It is common in males.
_ Swelling is deep to sternocleidomastoid muscle below the level of thyroid
cartilage; initially soft and emptying; impulse on coughing may be evident unless
opening of the pouch is blocked due to recurrent inflammation.
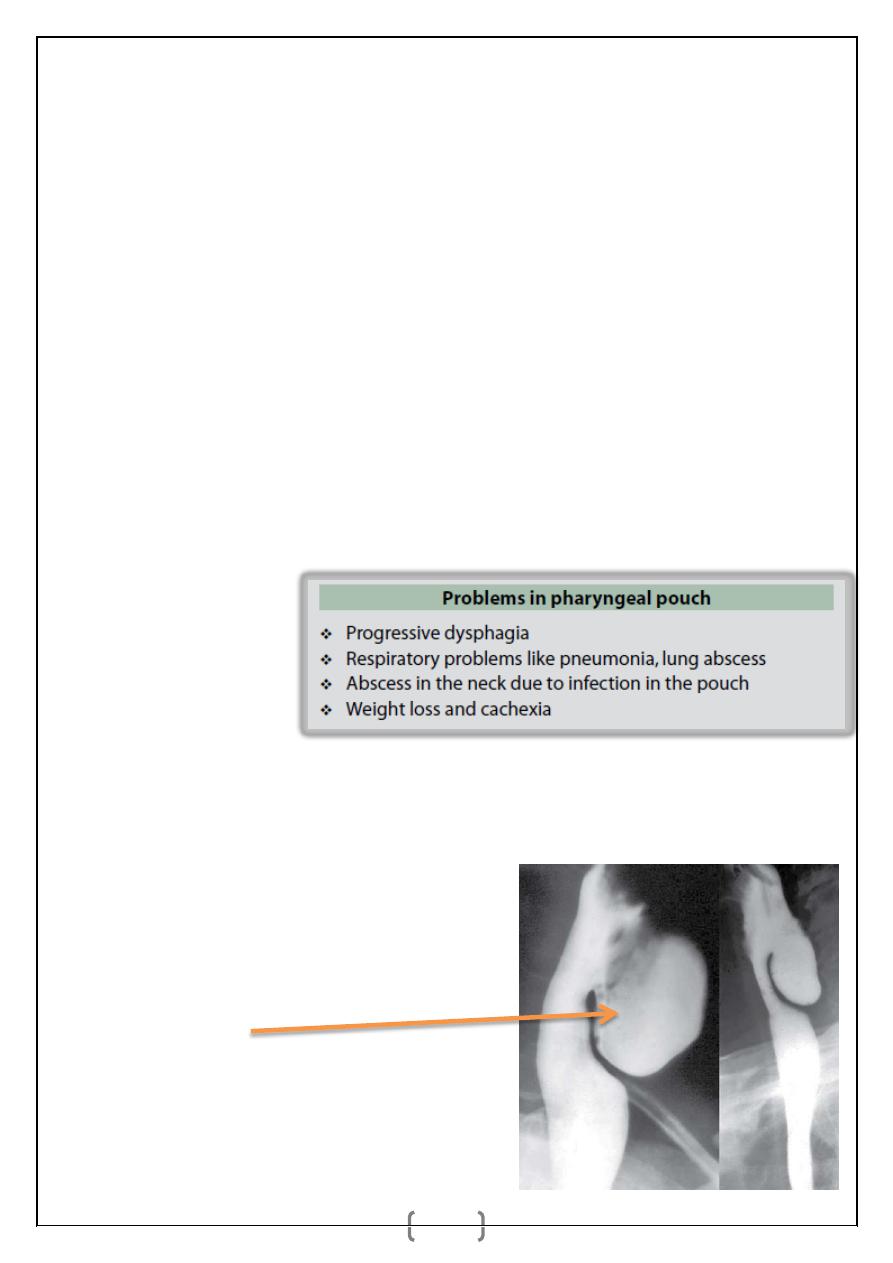
Complications:
Differential Diagnosis
_ Branchial cyst.
_ Cold abscess in the neck.
_ Lymph cyst.
_ Haemangioma neck.
Investigations
_ Barium swallow—lateral view shows
pharyngeal pouch.
_ Chest X-ray shows pneumonia.
_ CT neck is very useful.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
8
Treatment
_ Antibiotic is started to control infection.
_ Pharyngeal pouch is excised by an oblique neck incision (approach from neck).
As there is cricopharyngeal spasm, cricopharyngeal myotomy (i.e. cutting of
cricopharyngeal circular muscle fibres without opening mucosa) is done to
prevent the recurrence.
Indications for surgery
_Progressive symptoms.
_Recurrent respiratory
complications.
_ Dysphagia.
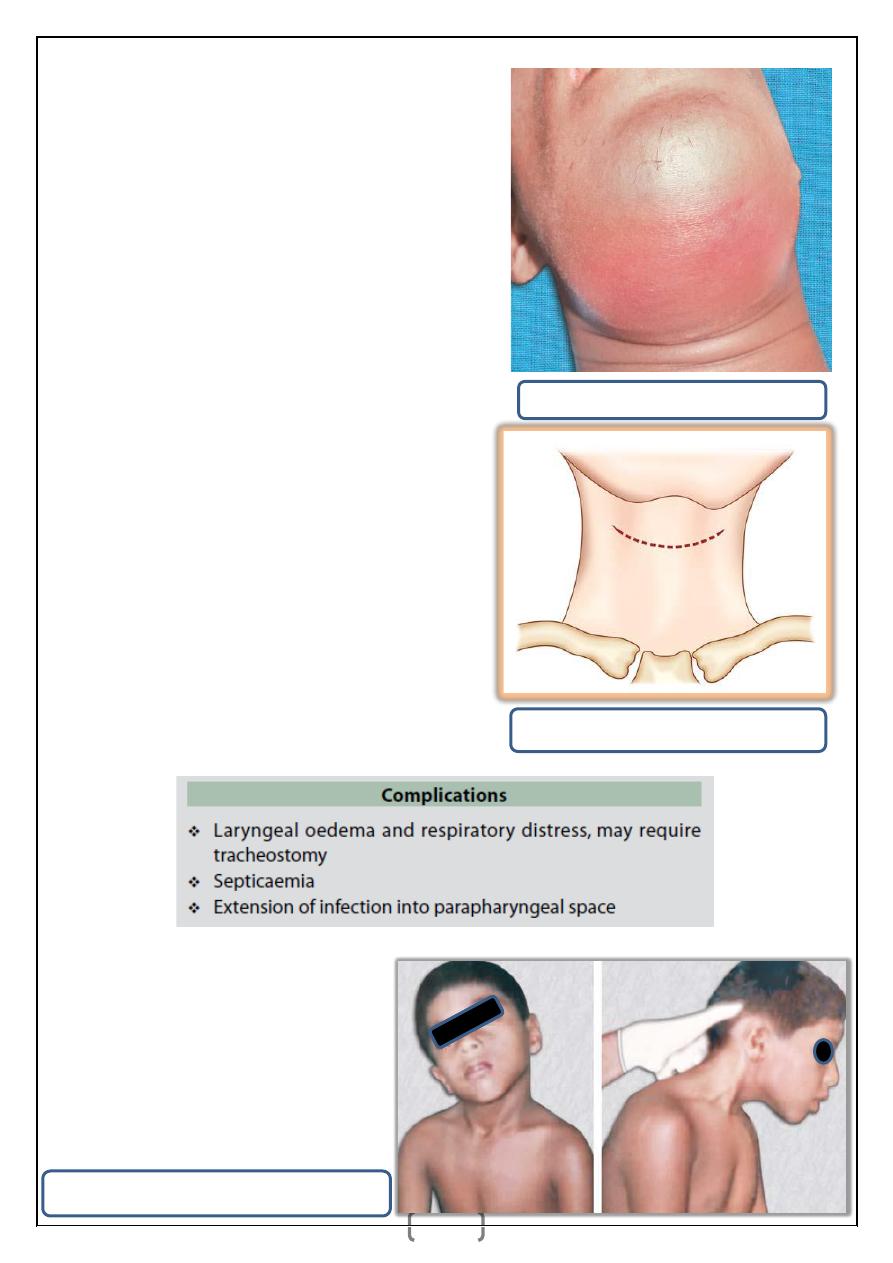
LUDWIG’S ANGINA
_ It is an inflammatory oedema of submandibular region and floor of the mouth,
commonly due to streptococcal infection.
_ It causes diffuse swelling and brawny oedema of the submandibular region. It
is common in severely ill and in advanced malignancy, causing trismus,
laryngeal oedema. Extension of infection into parapharyngeal space may lead to
dreaded internal jugular vein thrombosis.
_ As the infection is deep to the deep fascia in a closed fascial plane, it spreads
very fast causing dangerous complications.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
9
Clinical Features
_ Fever, toxicity, diffuse swelling, dysphagia,
dyspnoea, trismus.
_ Intraoral oedema is common.
_ Brawny swelling in submandibular region.
_ Putrid halitosis.
Treatment
_ Antibiotics.
_ IV fluids.
_ Decompression of the submandibular
region is done, by making a deep incision
extending into the deep fascia and also
cutting both the mylohyoid muscles. Either
it is left open and delayed suturing is done
(better option) or it is loosely sutured.
Complications:
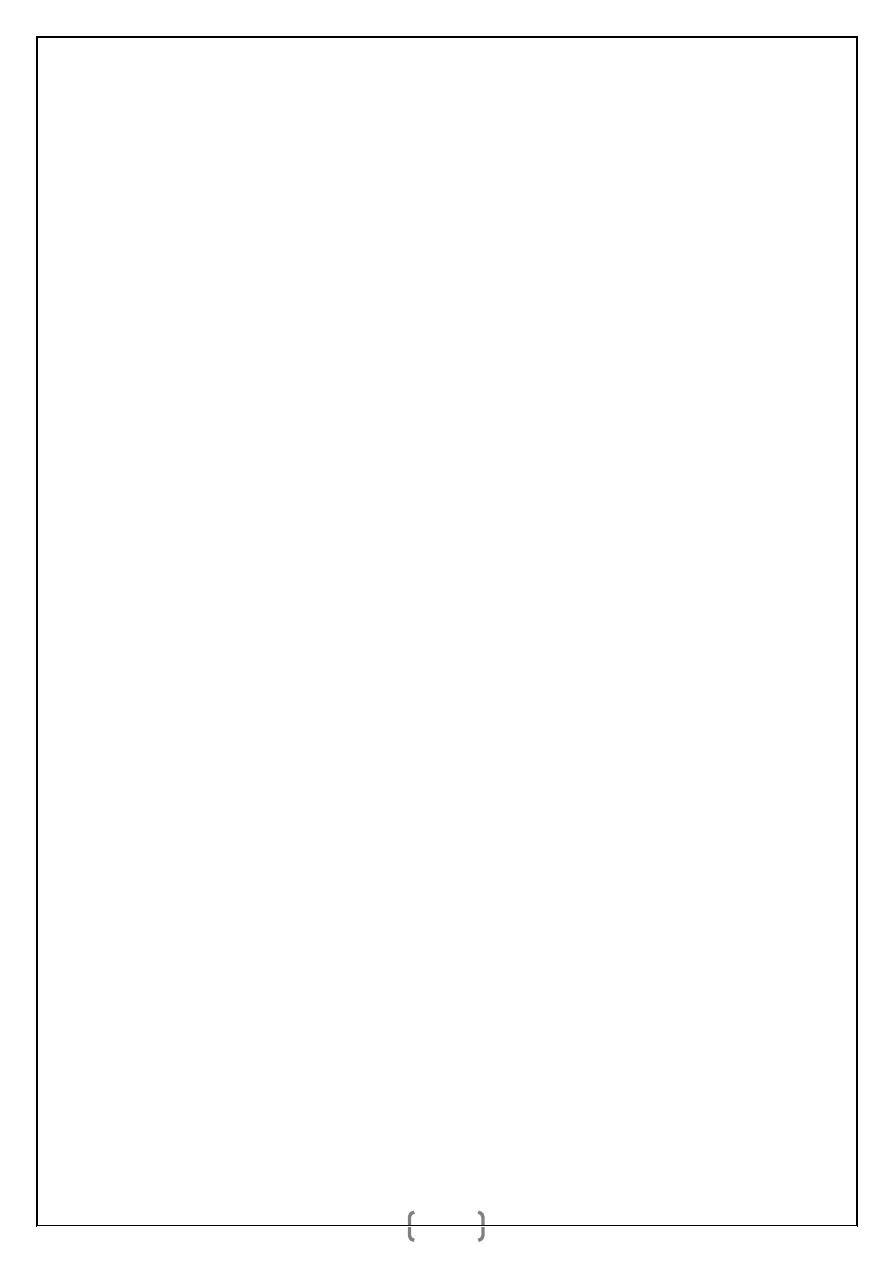
TORTICOLLIS (Wry Neck)
It is turning of the neck to one
side with chin pointing towards
opposite side.
Incision for draining Ludwig’s angina.
Typical Ludwig’s angina.
Boy having right-sided torticollis.
د.أشرف مزاحم الشاكر
كلية طب نينوى
الجراحة العامة
10
Causes:
_ Sternomastoid tumour.
_ Trauma—spinal injury, disc prolapse, spondylosis.
_ Inflammatory: Lymphadenitis either tuberculous or suppurative; tuberculosis of
cervical spine.
_ Spasmodic—due to spasm of sternomastoid muscle of same side or spasm of
posterior cervical muscles of opposite side.
_ Reflex.
_ Rheumatic—after exposure to cold/draught.
_ Burns—causing contracture.
_ Ocular causes.
_ Compensatory due to scoliosis.
Happiness is when what you think, what you say, and what you do are
in harmony —Mahatma Gandhi.