TEETHING AND DIFFICULT
ERUPTIONEruption of teeth cont…..
ObjectivesEffect of teething on the infant
eruption difficulties
Natal and neonatal teeth
Normal intraoral findings in the first month of the infant’s life
Local and systemic factors that influence eruption
increased salivation,
and the child will want to put the hand and fingers into the mouth.Effect of teething on the infant
Teething causes
daytime restlessness,
an increase in the amount of finger sucking or rubbing of the gum,
an increase in drooling,
and possibly some loss of appetite.
increase the incidence of infection,
does not cause any rise in temperature, erythrocyte sedimentation rate(ESR), or white blood cell count (WBC)and does not cause diarrhea, cough, sleep disturbance, or rubbing of the ear or cheek,
Studies showed that teething does not cause
Serious mistakes have been made in the care of infants and toddlers when their symptoms were ascribed to teething without completion of a thorough diagnostic evaluation and resulted in the overlooking of significant systemic disturbancesInflammation of the gingival tissues before complete emergence of the crown may cause a temporary painful condition that subsides within a few days.
The surgical removal of the tissue covering the tooth to facilitate eruption
is not indicated.
The parent can apply the topical anesthetic to the affected tissue over the erupting tooth three or four times a day.
Caution must be exercised, however, when one is prescribing topical anesthetics, especially for infants, because systemic absorption of the anesthetic agent is rapid, and toxic doses can occur if it is misused.
If the child is having extreme difficulty

The eruption process may be hastened if the child is allowed to chew on a piece of toast or a clean teething object.

Eruption difficulties
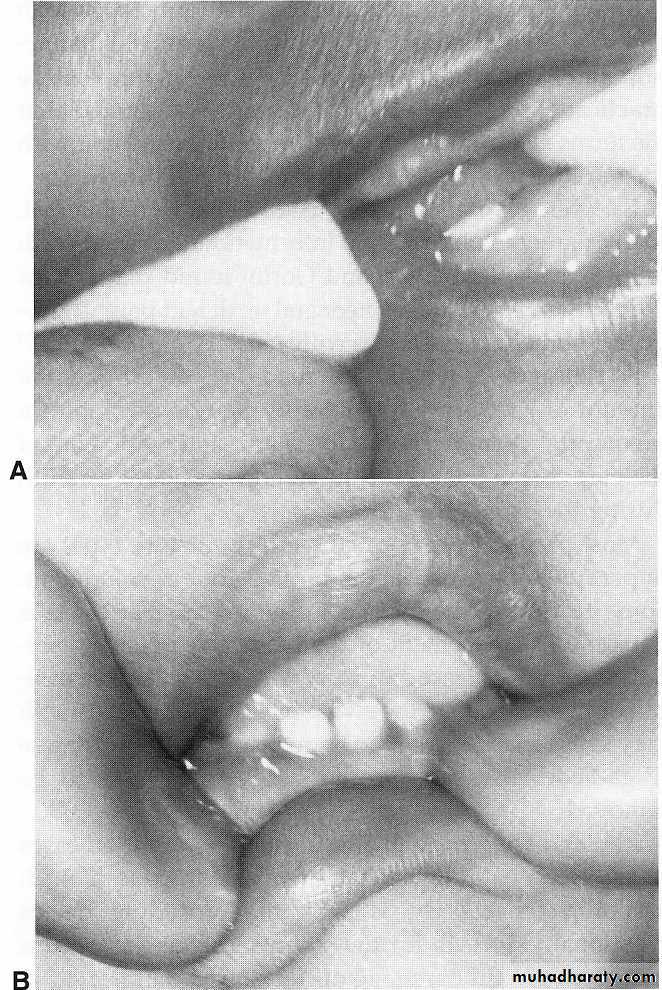
occasionally develops a few weeks before the eruption of a primary or permanent tooth.seen in the primary second molar or the first permanent molar regions
Usually within a few days the tooth breaks through the tissue, and the hematoma subsides.
Because the condition is almost always self-limited, treatment of an eruption hematoma is rarely necessary.
However, surgically uncovering the crown may occasionally be justified.
1. ERUPTION HEMATOMA (ERUPTION CYST)
Eruption cyst


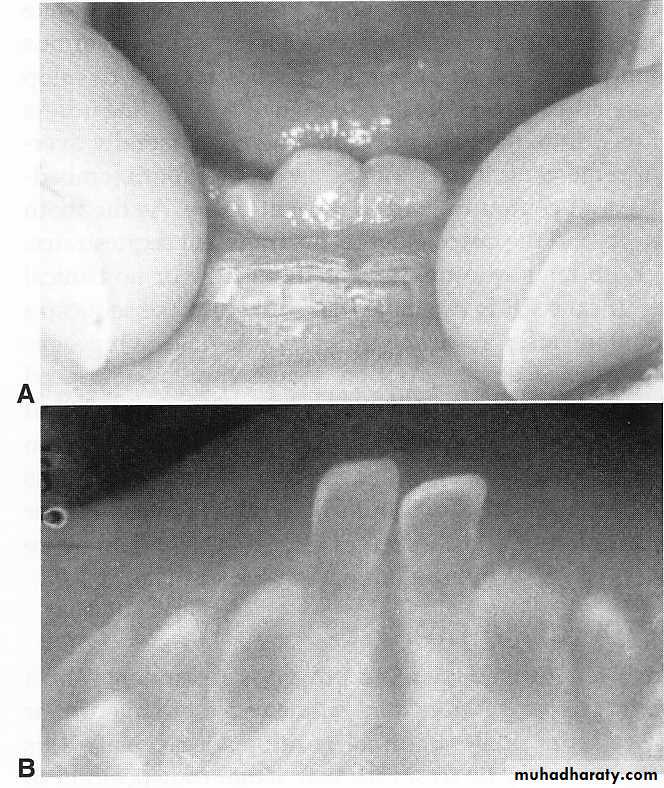
seen occasionally in children at the time of the eruption of the first permanent molar a tiny spicule of nonviable bone overlying the crown of an erupting permanent molar just before or immediately after the emergence of the tips of the cusps through the oral some of these sequestra spontaneously resolve without noticeable symptoms.'
2. ERUPTION SEQUESTRUM
after an eruption sequestrum has surfaced through the mucosa, it may easily be removed if it is causing local irritation.
If the base of the sequestrum is well embedded in gingival tissue when it is discovered,
application of a topical anesthetic or infiltration of a few drops of a local anesthetic may be necessary to avoid discomfort during removal.

ERUPTION SEQUESTRUM
a tooth erupts or try to erupt in :an abnormal position due to one of the following:Arch length inadequacy,
large toothor a variety of local factors .
3. ECTOPIC ERUPTION
Ectopic eruption of the maxillary permanent molars

Ectopic eruption
Maxillary left lateral
Maxillary left central

Natal and neonatal teeth
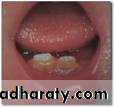
natal teeth (teeth present at birth)
neonatal teeth (teeth that erupt during the first 30 days)
85% of natal or neonatal teeth are mandibular primary incisors, and only small percentages are supernumerary teeth.
Early eruption of primary teeth seems to be familial.
A radiograph should be made to determine the amount of root developmentOne of the parents can hold the x-ray film in the infant's mouth during the exposure.
In some infants, however, the presence of such teeth may be a localized manifestation of an environmental cause or an underlying syndrome,and this underscores the importance of thorough diagnostic evaluations of infants with natal or neonatal teeth.
1. mobile to the extent that there is danger of displacement of the tooth and possible aspiration
2. sharp incisal edge of the tooth may cause laceration of the lingual surface of the tongue (Riga-Fede disease), and the tooth may have to be removed.
Most prematurely erupted teeth are hypermobile because of the limited root development.
in which case the removal of the tooth is indicated
After the tooth is removed,
careful curettage of the socket is indicated in an attempt to remove any odontogenic cellular remnants that may otherwise be left in the extraction site.Such retained remnants may subsequently develop atypical tooth like structures that require additional treatment
however, is to leave the tooth in place
and to explain to the parents the desirability of maintaining this tooth in the mouth because of its importance in the growth and uncomplicated eruption of the adjacent teeth.Within a relatively short time the prematurely erupted tooth will become stabilized, and the other teeth in the arch will erupt.
The preferable approach
Normal intraoral findings in the first month of the infant’s life:Three types of inclusion cysts
Small, white or grayish white lesions on the alveolar mucosa of the newborn may on rare occasions are incorrectly diagnosed as natal teeth.The lesions are usually multiple but do not increase in size
No treatment is indicated, since the lesions are spontaneously shed a few weeks after birth.
EPSTEIN PEARLS, BOHN NODULES, AND DENTALLAMINA CYSTS
Epstein pearls
1. Epstein pearls are formed along the midpalatine raphe.

Bohn nodules
2. Bohn nodules are formed along the buccal and lingual aspects of the dental ridges and on the palate away from the raphe
Dental lamina cyst in the maxillary arch
3. Dental lamina cysts are found on the crest of the maxillary and mandibular dental ridges.The cysts apparently originated from remnants of the dental lamina.
Dental lamina cyst (arrow). No treatment is indicated;
such lesions disappear within a few weeks after birth
Dental lamina cyst

LOCAL AND SYSTEMIC FACTORS THAT INFLUENCE ERUPTION
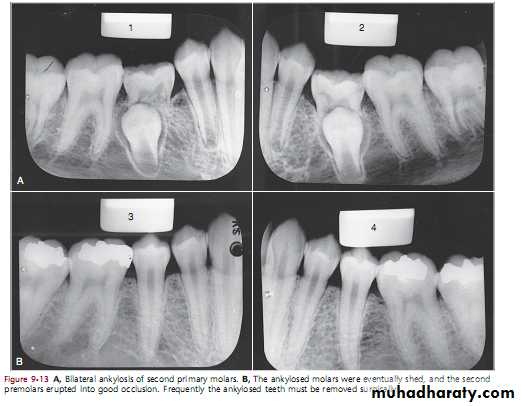
LOCAL FACTORSANKYLOSED TEETH
It is an interruption in the rhythm of eruptiona patient who has one or two ankylosed teeth is more likely to have other teeth become ankylosed.
The problem of ankylosed primary molars deserves much attention by dentists.
the ankylosed tooth is in a state of static retention, whereas in the adjacent areas eruption and alveolar growth continue and the tooth will be infra-occlussionThe mandibular primary molars are the teeth most often observed to be ankylosed
Infra-occlussion


The cause of Ankylosis of the anterior primary is trauma
The cause of ankylosis in the primary molar areas isunknown,
but at least three theories
have been proposed.
1. follows a familial pattern
2. congenital absence of permanent teeth3. race :ankylosis occur more in white children
theories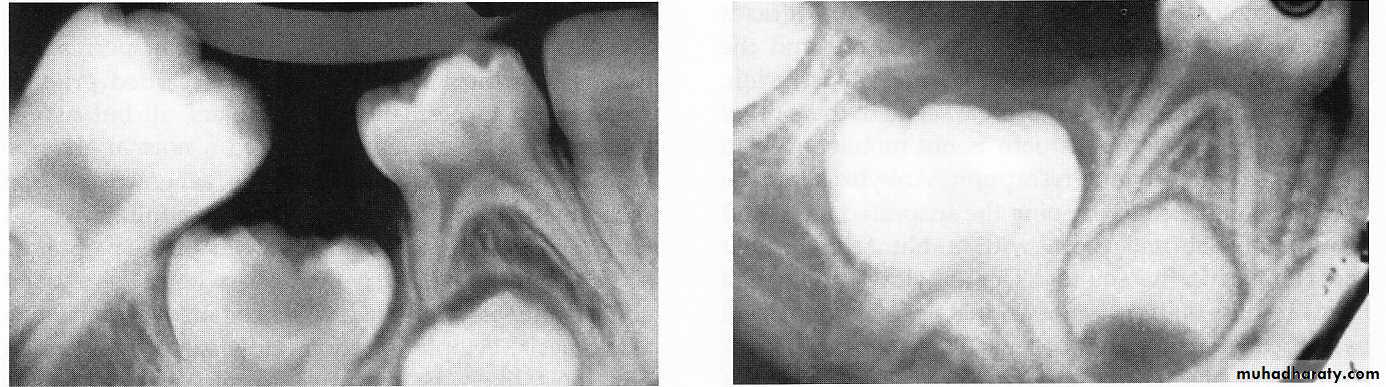
Ankylosed second primary molar with a carious lesion in the occlusal surface.
This tooth probably becameankylosed soon after root resorption began.
An ankylosed, deeply embedded second primary molar. Surgical removal of this tooth is indicated
early ankylosis of a mandibular second primary molar that was not diagnosed until the patient was 10 years of age; at that time the succedaneous second premolar was lying malposed “
Surgical removal of this tooth is indicated
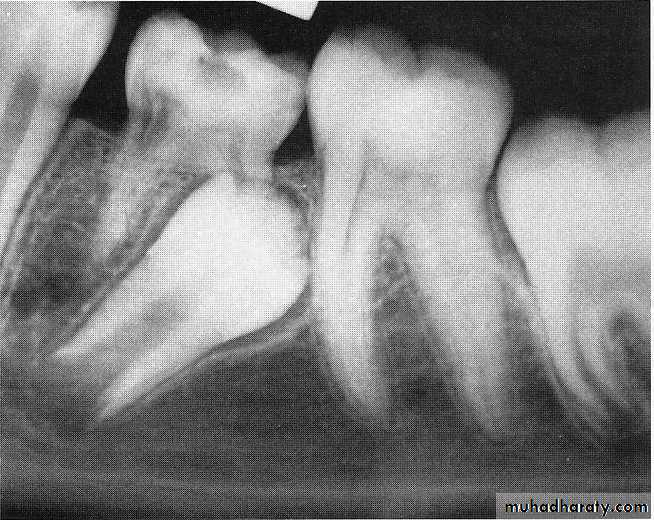
The second primary molar is ankylosed and below the normal plane of occlusion.
There is evidence of root resorption and deposition of bone into the resorbedareas.
1. Opposing molars in the area seem to be out of occlusion
2. The ankylosed tooth is not mobile, even in cases of advanced root resorption3. Confirmed by tapping the suspected tooth and an adjacent normal tooth
The ankylosed tooth will have a solid sound, whereas the normal tooth will have a cushioned sound
The diagnosis of an ankylosed tooth
4. A break in the continuity of the periodontal membrane indicating an area of ankylosis is often evident
radiograph is often a valuable aid in making a diagnosis
1. When patient cooperation is good and recall periods are regular, a watchful waiting approach is best.
2. If loss of arch length is evident, the dentist may choose to keep the tooth under observation.
A tooth that is definitely ankylosed may at some future time undergo root resorption and be normally exfoliated.
3. The eventual treatment may involve surgical removal
TreatmentSometimes the ankylosed primary tooth shed by itself, if not extraction is the treatment
ANKYLOSIS OF PRIMARY MOLARS WITH ABSENCE OF
PERMANENT SUCCESSORSIf missing one tooth or two teeth do onlay
If missing of three or four teeth referred to ortho
If one side or two sides missing permanent tooth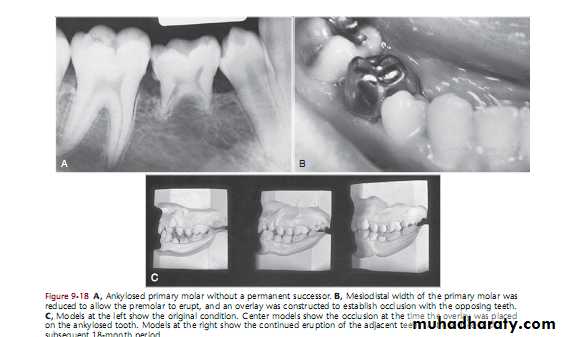
Systemic factors
1.TRISOMY 21 SYNDROME (DOWN SYNDROME)Systemic factors


2. CLEIDOCRANIAL DYSPLASIA
(absence of clavicle bone)

3. congenital
HYPOTHYROIDISM:
4. HYPOPITUITARISM

:
1. delay eruption of primary teeth
2. delay exfoliation of primary teeth due to retention
3. delay eruption of permanent teeth
4. sometimes presence of supernumerary teeth
So they need follow up from birth until adulthood.
In all those systemic diseases