A good dentist is one who is able to diagnose potential problems during the initial examination….and suggest the best treatment plan.


Diagnosis & treatment planning of completely edentulous patients
Dr. Zhala Dara MeranDept. of Prosthodontics
2017

INTRODUCTION
Each pt. uniqueGood clinical examination
Identifying the problems
Good assessment of patient’s physical and
psychological conditionAffect the outcome of treatment
Discuss with pt. …..all the facts ….educate pt.

The following procedures may be carried out prior to the initiation
of the denture treatment:Recording the general information
Recording the chief complaint and assessing
pt. expectations.
Recording the relevant medical history.
Recording current medicationRecording the relevant dental history
Performing a visual and manual examination of the mouth and head and neck regions.
Performing a radiographic examination.
Referring for additional tests ex. Blood, sugar.Referring to medical consultation if indicated.
Preparing study cast.
Discuss diagnosis ,treatment plan with pt.
Finalizing the fees and obtaining a signed consent.

Interviewing the pt.:
The first meeting is the most important……Trust
Understanding at this stage
Confidence
Dentist should …..
good listener
Show care for pt. problems.
General observation ...…appearance, general health,
Pt. also will assess the dentist…..so be simple, trustful.

Recording general information:
Before the dentist meets pt…………general inforeception staff or giving them form to fill:
Name: ….confidence building.
Age:…..Tissue healing, DM, heart diseasesSex:….female vs male {exacting and hysterical}
Occupation:….job …esthetic.
Contact number:…any time



Psychological evaluation:
The House Classification:…personalityPhilosophical……well motivated, rational, sensible, calm.
Exacting…..explain each step, give alternative, demands ….management : extra care, patience, listening only
Indifferent….questionable prognosis, no motivation,
not interested, tries to find faultsmanagement.:try …no … let go
Hysterical: easily excited, emotionally unstable, no cooperation .
Management: time effort, medical consultationSkeptical: bad result from previous treatment, doubtful
Management:care, time, attention.


Favorable adaptive response to CD:
TrustConfidence
Previous experience
Attitude
Realistic expectation
Age, health
Willingness, learning capacity
*Reason for seeking prosthetic treatment?
*Pt. expectation?
Maladaptive response to CD :
Lack trust
Poor communicationExperience
Anxiety
Un realistic expectation
Poor health
Poor learning
Medical history:
Any condition might affect procedureEmergencies
Transmitted diseases
Refer, consultation
DM, pre prosthetic surgeryCardiovascular disease ………….short , premedication, AB
Neurological disorder……………..cooperation
Malignancy………..radiation …….…tissue
Transmitted disease

Dental history:
History of tooth loss………..periodontal?Experience with old denture?............ Avoid same problems
Edentulous period? few month …………..…fast restoration.



EXTRAORAL EXAMINATION
1. General appearance
2. Facial examination
Facial symmetry
Facial form
Facial profile
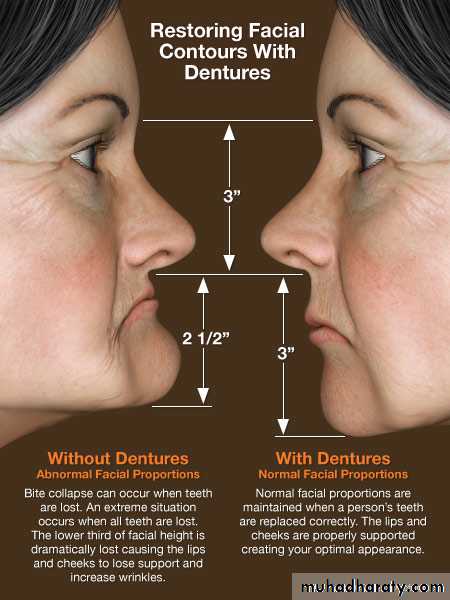
Lower facial height
3. Muscle tone
4. Head and neck
5.Lips
Lip length
Lip thickness
Lip support
6. Neuromuscular evaluation
7. Speech evaluation8. Temporomandibular examination
• GENERAL APPEARANCE:Does the patient appear healthy?
Does the patient show signs of proper nourishment?2. FACIAL EXAMINATION:
Facial symmetry
Does the face appear symmetric or asymmetric?Outline form of face important for the selection of tooth shape.

Facial form
Classification of (frontal) face formHouse and Loop, Frush and Fisher and William’s classified face form as:
Square, Square-tapering, Tapering, Ovoid
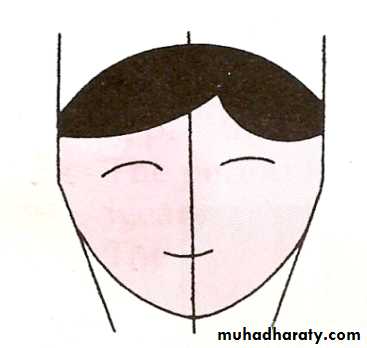
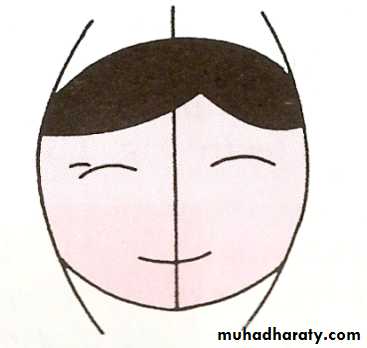
Examining the facial form helps in teeth selection.
General outline of the tooth should confirm to the general outline of the face when viewed from the frontal aspect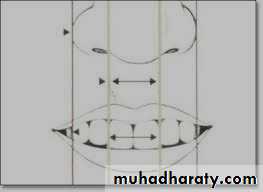


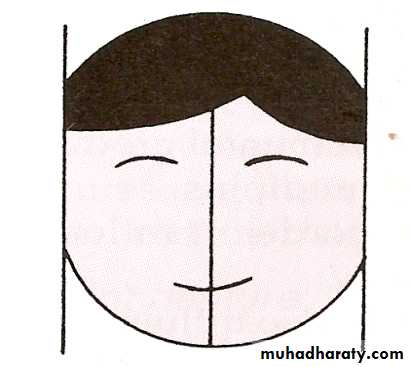
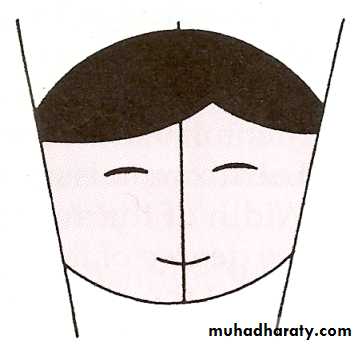
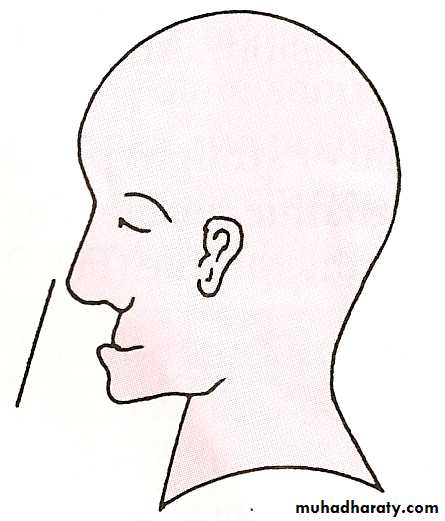
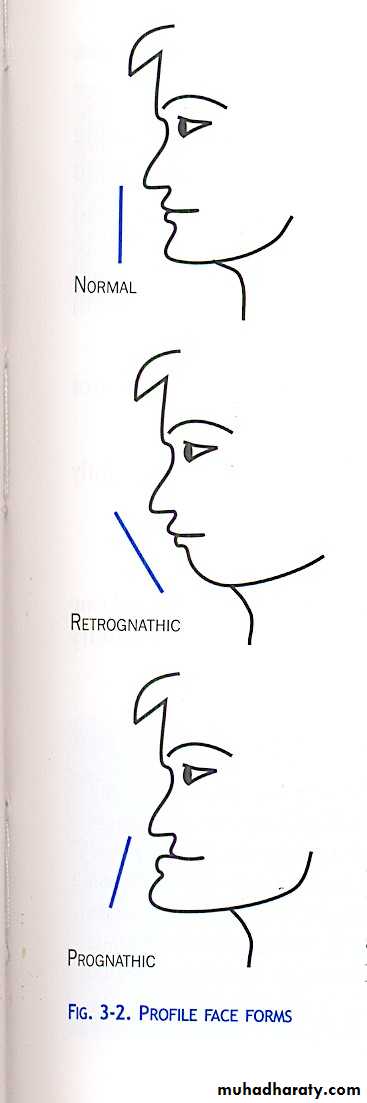
Facial profile
Classification of the facial profile(lateral face form) (Angle)
Class I – Normal
Class II – Retrognathic
Class III – Prognathic
Examination the facial profile is important because it determines the jaw relation and occlusion.
•
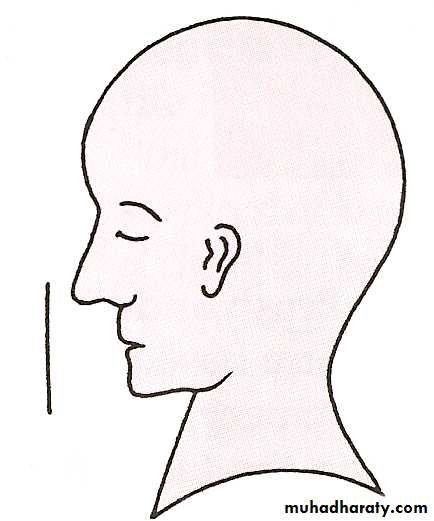
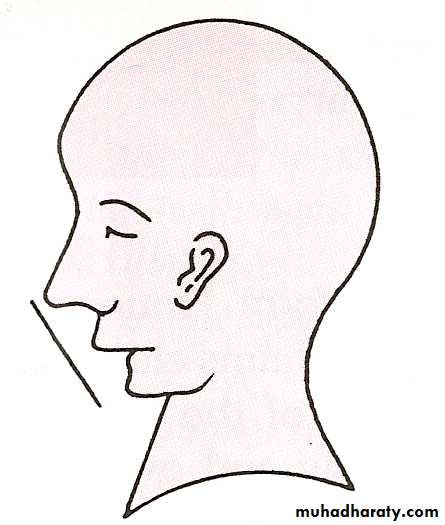
While observing the profile, dentist should ask the patient to :
Sit uprightWet the lips
Place them into light contact and
Relax
Profile is assessed by joining two
reference lines-

Skin color can also reveal underlying disease and pathology:
*Pallor – may be indicative of anemia, hypothyroidism, or nephrosis or may be due to lack of nourishment* cyanosis vary from bluish purple to red purple.
*Bronzed skin – addison’s disease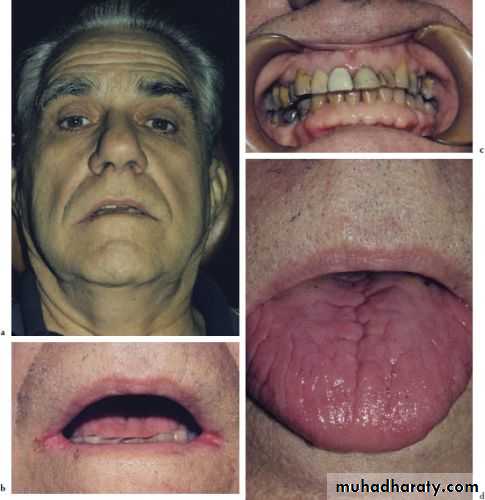
LIP EXAMINATION:
Lip support
Lip lengthLip thickness
Lip mobility
Health of the lips

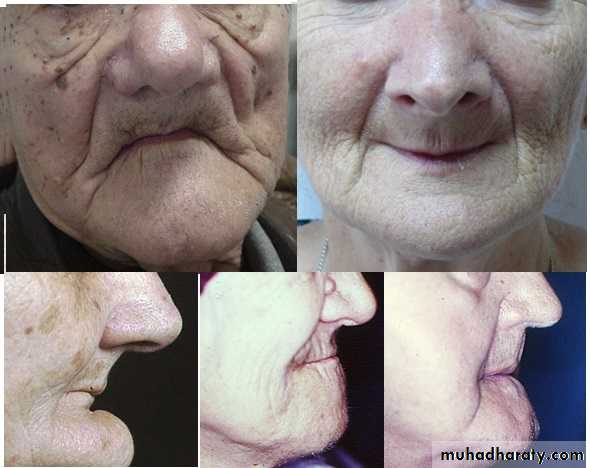
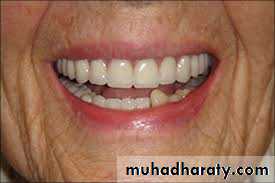
LIP SUPPORT – adequately supported
- unsupportedContour and appearance of the
vermillion border usually are alteredby tooth loss
Placement of anterior teeth
If the anterior teeth are set too far lingually or palatally, lips will lack the necessary support.

Unsupported lip


Lip length
How much tooth will be exposed ?Determinant in anterior teeth selection.
Lip length is classified as -
A. Long B. Medium C. Short



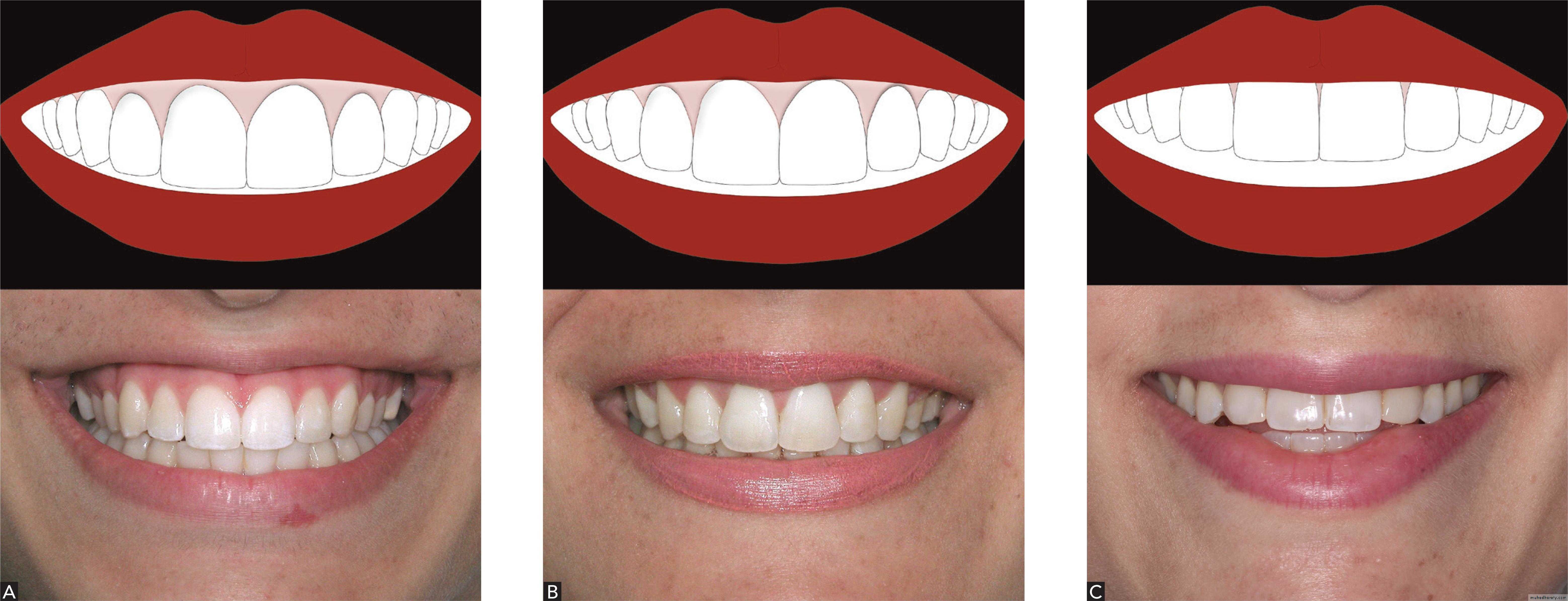
lip line , smile line classification:
A high lip lineLow lip line
Normal lip line
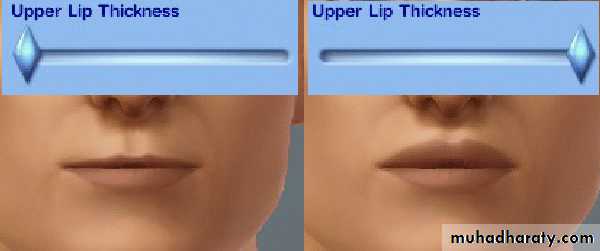
Lip thickness:
Thick lips – need lesser support from the artificial teeth and the labial flange.Thin lips – rely on the appropriate labiolingual position of the teeth, for their fullness and support
LIP MOBILITY
NormalReduced
paralysis
Patients with minimal lip mobility show very little of the anterior teeth
Some stroke ….. unilateral mouth droop and facial asymmetry

NEUROMUSCULAR EVALUATION
Poor neuromuscular coordination (stroke, paralysis, parkinsonism etc.) -difficult to adapt to a new denture.Asked to perform various mandibular movements.
Neuromuscular coordination may be classified as
Class I – Excellent
Class II – FairClass III- Poor
SPEECH EVALUATION
Patients with speech impediments require special attention in setting of anterior teeth and forming the palatal portions of the upper denture.Speaking activity may be classified as
NormalAffected

If pain or difficulty in opening the mouth.
Check for tenderness, clicking.Uncoordinated movements indicate difficulty in jaw relations.
• Temporomandibular joint examination
•

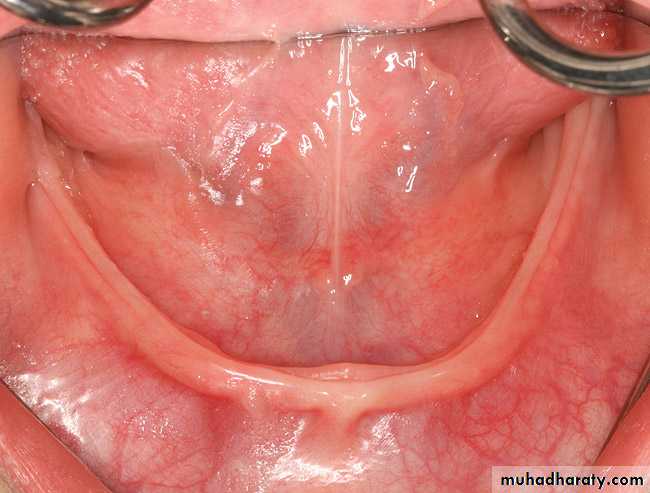
INTRAORAL EXAMINATION
INTRAORAL EXAMINATIONSoft tissue ExaminationCHEEKS
General contour of cheeks noted.
Filling buccal spaces- need concave buccal contours on dentures
Cheek tissue over the buccal flange of denture ….seal
Any lesions seen? Lichen planus?
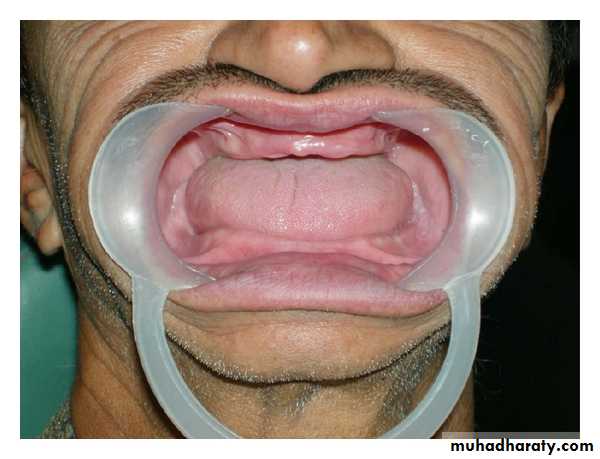
TONGUE
If patient is without teeth or prostheses for long time ………………become enlarged …….affects impression taking & denture instability.Small tongue facilitate impression making but jeopardize a lingual seal.

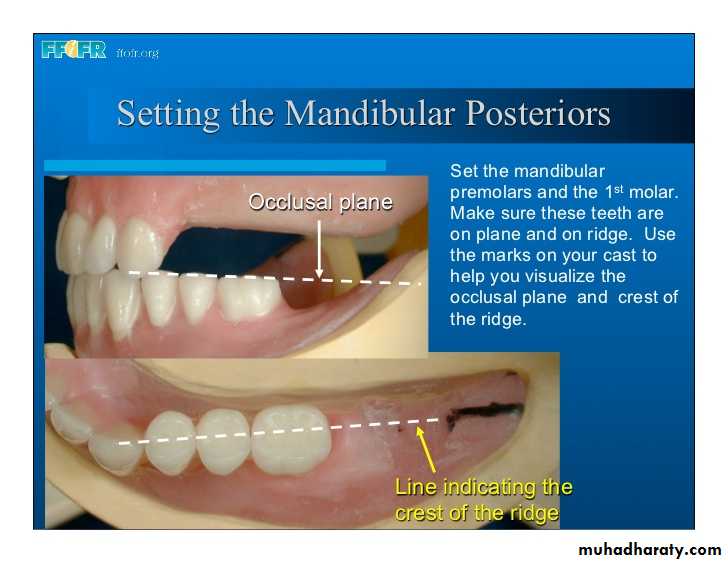
Large tongue management:
The occlusal plane loweredNarrower teeth
Grind off lingual cusps
Avoid second molar

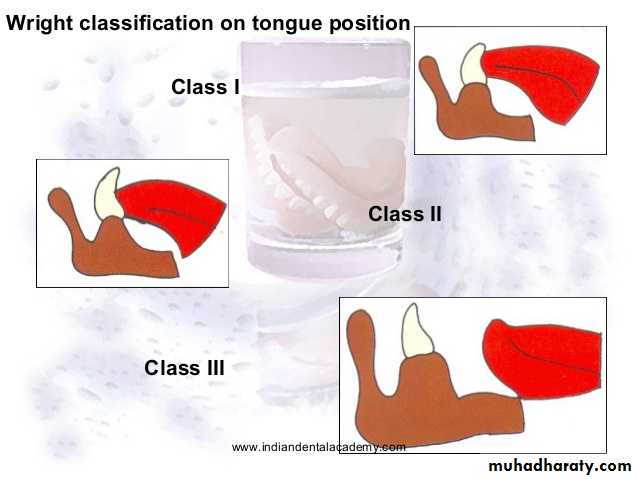
Wright classified tongue position as follows:
Class I- tongue lies in the floor of the mouth -tip forward and slightly below the incisal edges of the mandibular anterior teeth.Class II- tongue flattened and broadened- tip in normal position.
Class III- tongue retracted and depressed
into the floor of the mouth with the tip
curled upward, downward, or assimilated
into the body of the tongue.
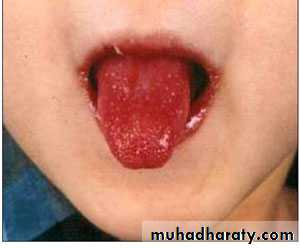
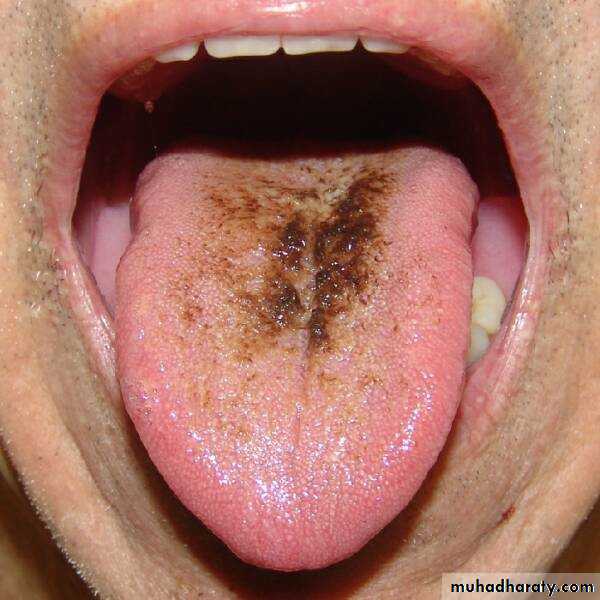
Tongue mucosa: geographic tongue, Red inflamed tongue ,hairy tongue , candida albicans.


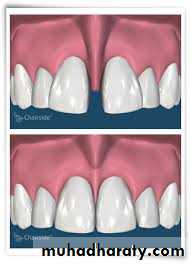
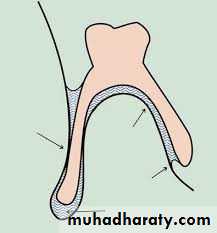
Frenal attachment:
Class l: low attachment ….goodClass ll: midway between sulcus and crest of ridge.
Class lll:high attachment crestal or near crest…poor

Maxillary tuberosity:
Too low….not enough space…
undercut removal and insertion .
Management?

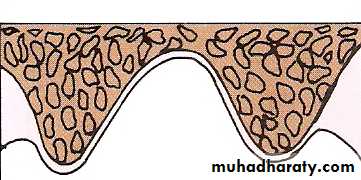
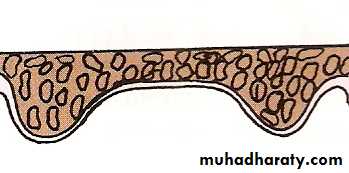
THE HARD PALATE
Shape of hard palate can be:U shaped -Most favorable for retention and stability.
V shaped- Not very favorable. Slight movement of the denture breaks the seal & loss of retention.
• May be associated with a tapered arch
Flat or shallow vault- Reduced resistance to lateral and rotatory forces. Usually accompanied by resorbed ridge.
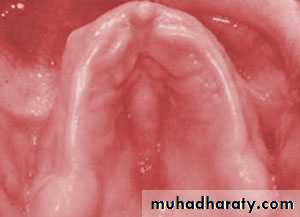
Palatal torus:
Class l: absent or minimal.Class ll: moderate.
Class lll: large
Management :1,2

Smoker palate stomatitis nicotinae:
Nodular center,red inflamed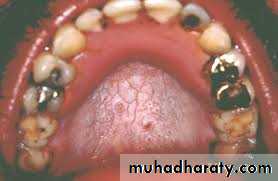

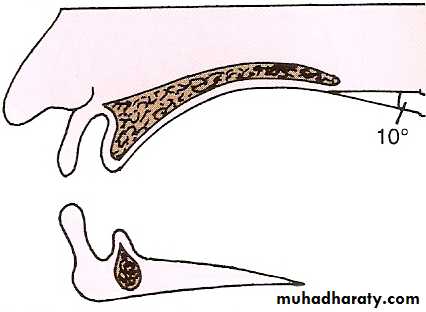
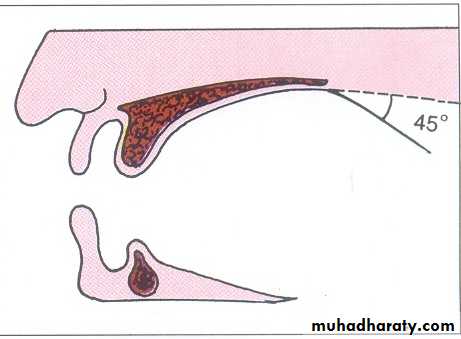
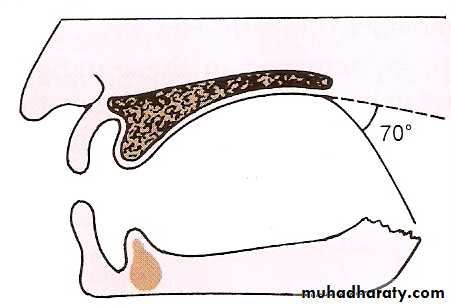
SOFT PALATE
Class I : Horizontal curving downwards.Most favorable as more surface area
covered for retention & wider seal area.
Muscular activity minimal.
CLASS II: Palate turns downward at about
45 degree angle to the hard palate
tissue coverage is less than Class 1
Good retention is usually possible
Class III : Turns downward sharply at 70o angle.
Greater movement of soft palate less seal areahence less favorable.
ARCH SIZE
Denture bearing area increases with arch size & increases retention.Discrepancy between the mandibular and maxillary arch size -difficulties in artificial teeth arrangement and decrease the stability of the denture.

Arch size
CLASSIFICATIONARCH FORM
Plays a role in support of a denture and in tooth selectionDiscrepancies between the maxillary and mandibular arch forms can create problems during teeth setting

Arch form
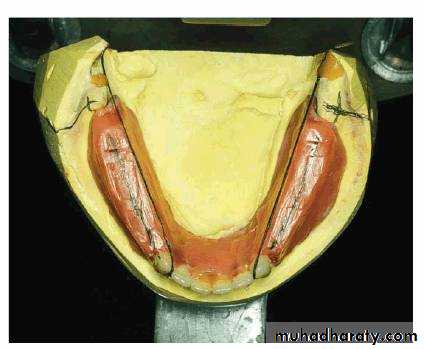
RIDGE CONTOUR
Ridges should be inspected and palpated
Should be palpated for sharp bon which produce pain on palpation
Ridges can be classified based on their contour as :
High ridge with flat crest and parallel sidesFlat ridge
Knife edged ridge
Arch size discrepancy :
Due to….Congenital, truma to TMJ, maloccusion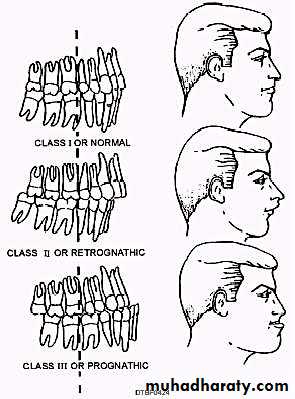

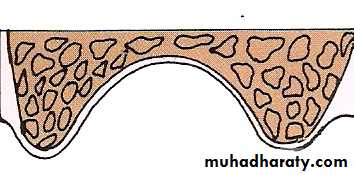
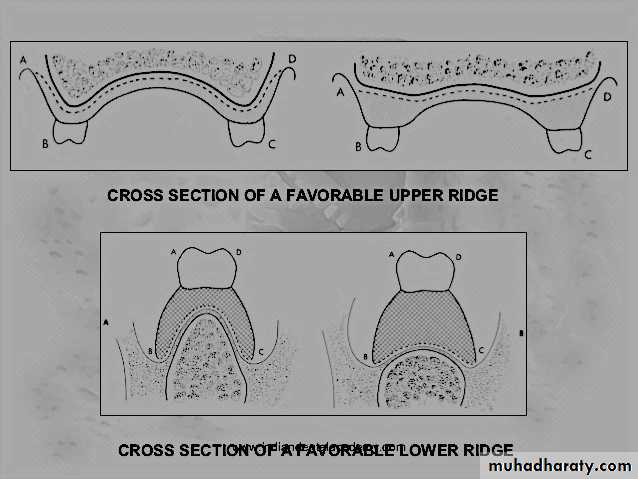
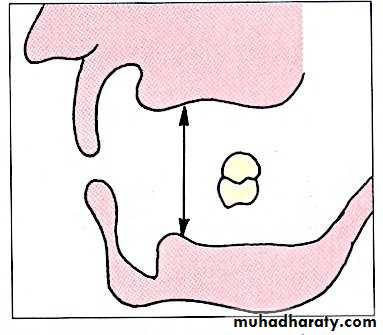
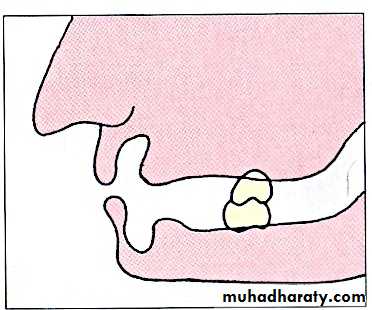
RESIDUAL RIDGE (CROSS SECTIONAL) CONTOUR
Ideal ridge - well developed high ridge with broad crest and parallel sides. Types based on shapes:Small amount of inter ridge distance leads to difficulty in setting teeth and maintaining a proper freeway space.
Also known as inter arch space and can be classified as :
a) Ideal interarch space to accommodate the artificial teeth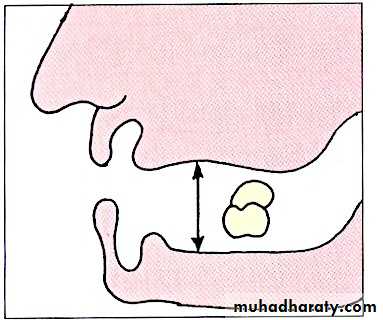
Excessive interarch space
Insufficient interarch space to accommodate the artificial teeth??????
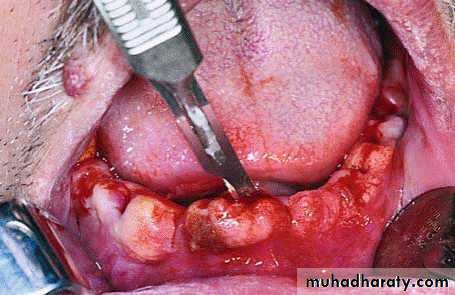
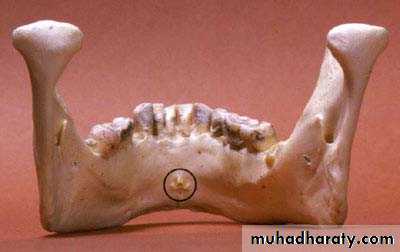
BONY PROMINENCES
Visual examination - manual palpation.Sulcus areas
Ridge crest and slopes
Palatal areas are palpated.
Midpalatal raphe
Bony spicules and sharp ridge crest
Sharp mylohyoid ridge
Palatal foramen
Bony fragments
Fractured root pieces
Genial tubercles


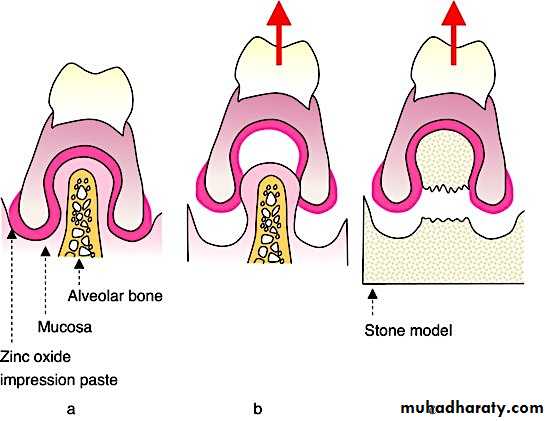
UNDERCUTS
Undercuts cause*Difficulty in denture removal & insertion
*Abrasion of mucosa & pain.
Classification:
Unilateral or bilateral
Labiall or lingual
Mild, moderate, severe.
Management :???
Both flow rate and viscosity important to denture success.
Lubricates the mucosa and assists retentionConsistency
Thin serous : more favorable for denture retention.Thick mucus: difficult to work with and tends to displace the denture.
Mixed : Contains equal quantities of both kinds.
Amount
NormalExcessive
Reduced
SALIVA

SUPPLEMENTAL DIAGNOSTIC AIDS
A. EXISTING DENTUREsometimes problem patient with unrealistic expectations.
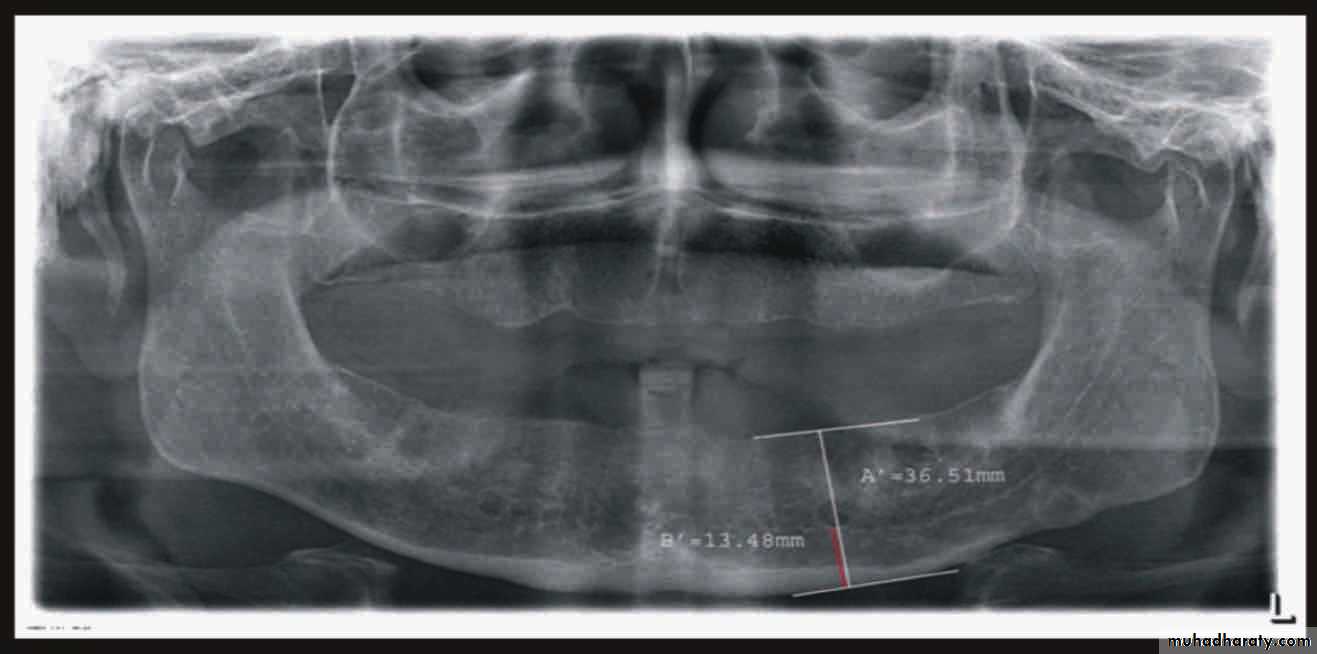
Radiographic examination:• Cyst
• Tumor• Retained root
• Periodontal condtion of remaining teeth
• Bone fracture
• Extend of bone resorbtion
• Locate cannal
• pt. education
What is treatment plan?Alternate Treatment Plan
Patient not prepared to undergo any kind of surgery or other dental proceduresNo time
patient demands or request may have to be considered (within limits).
If suggested treatment plan too expensive for the patient, a cheaper alternative has to be considered.
The alternative treatment plan may be ………less than ideal.
However………. must still try to achieve the best possible result.
Refusal of Treatment
Respect patient’s wishes and include it in the treatment plan whenever possibleSometimes, a patient’s demands are unreasonable or against professional judgment or ethics
Dentist may refuse treatment or refer him to another dentist for a second opinion

PROGNOSIS
After considering all factors – an experienced dentist must be able to predict the degree of success that can be expectedGive patient a fair idea of the possible outcome that can be expected
Leads to more realistic expectations and less frustration
CONCLUSION
A successful restoration does not just happen- it is planned!
Thorough diagnosis enables us to make a realistic prognosis


