Pre Prosthetic Surgery
Dr. Zhala Dara MeranDept. of Prosthodontics
2017
Many conditions can exist in the mouth which can interfere with the construction and successful use of the denture .
The methods to improve denture :
NonsurgicalSurgical
Combination

Nonsurgical methods:
Rest of the supporting tissue(out of the mouth, tissue conditioner, finger message)
Occlusal correction of the old prostheses.
(old denture…wear occlusal surface, restore VD)Good nutrition
(vitamins ,minerals)Conditioning of of the pt. musculature.
(TMJ exercise)


Per prosthetic examination:
No mental, physical condition exist….interfere with tret.Medical history
Nutritional health.
Intra oral examination….maybe only nonsurgical.
TMJ examination
Radiograph, blood test, dental model.

Surgical procedures.
Preprosthodontic surgical procedures may be described under :Procedures to improve the bony foundation.
Procedures to improve soft tissue foundation.Procedures to improve ridge relationship
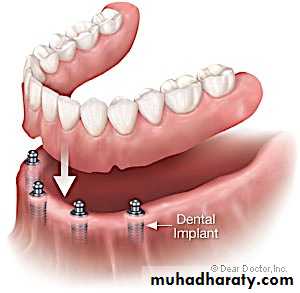
Implant procedures


Procedures to improve the bony foundation:
Retained dentition (un erupted, R.Root) associated with pathology….asymptomatic for years, may increase bone loss, impact upper third molar…preserve tuberosity .
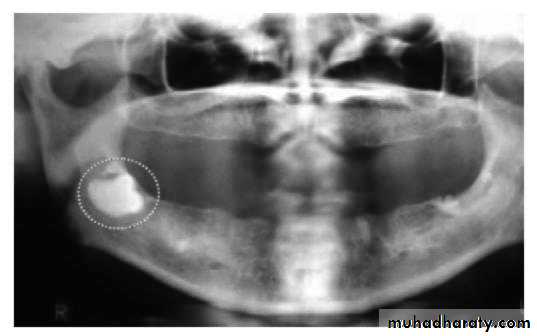
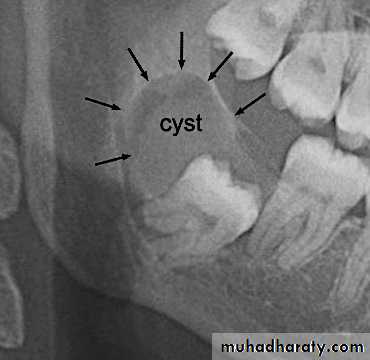
Removal of pathogenic bony conditions
( cyst, tumors)Cyst:…...enucleating or marsupialization
Tumor: ……Immediate attention.
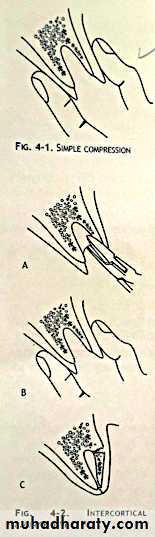
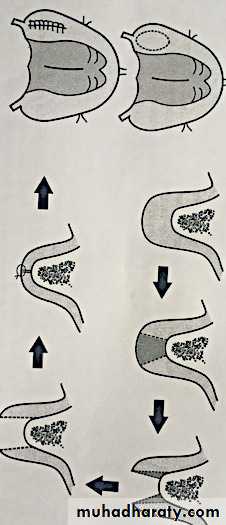
Technique to deal with alveolar excess:
AlveoloplastySimple compression
Cortical compression
Intercortical alveoloplasty
Alveolor repositioning
Tuberosity reduction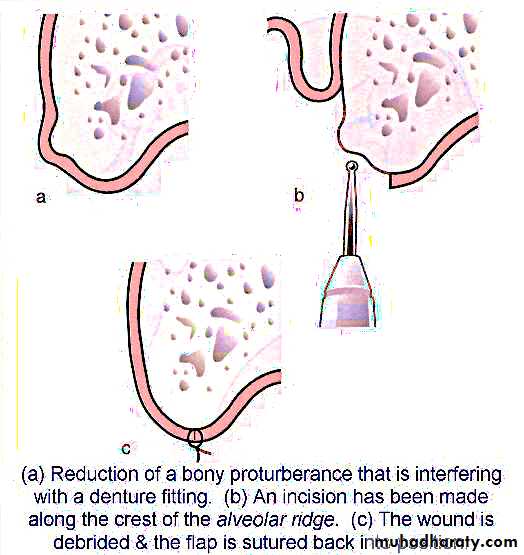
Technique to deal with alveolar excess:
Alveoloplasty: surgical smoothing and shaping of the alveolar ridge prior to denture placement.Extensive alveoloplasty….bone resorption…keep it minimum.
Types:_Simple compression……hand immediately after exo..for healing.
_Cortical compression………if denture construction urgent…..exo…crestal incision….. bone removed ….smoothed…suture if many exo._Intercortical alveoloplasty …… anterior ridge prominent…undercuts….interradicular septa removed …..rongeur …crushed…suture
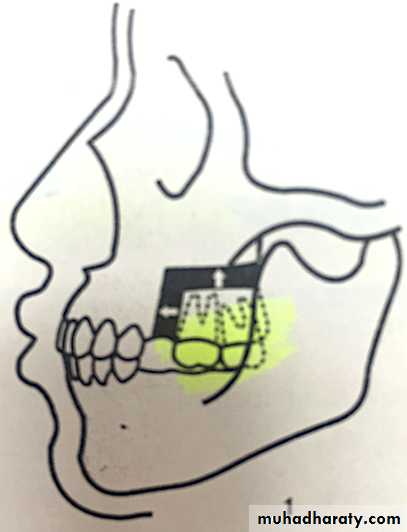
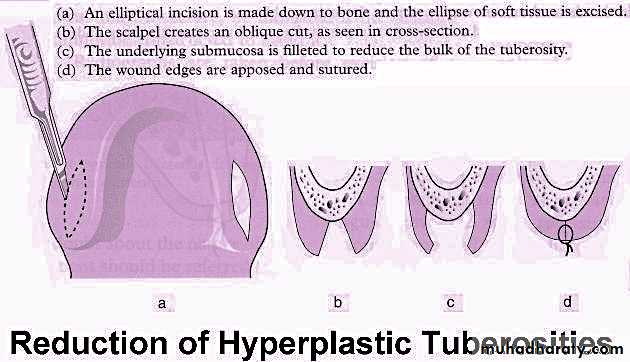
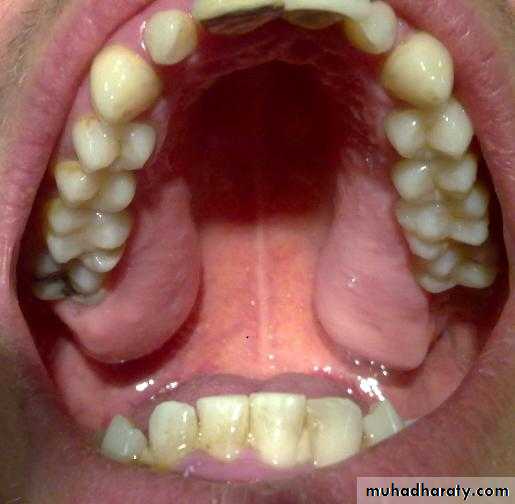
Tuberosity reduction:
Enlarge …interfere…..crestal incision….excess bone trimmed (Tissue cut)….(rongeur,bur)…….smoothed…….suture.
(Complication…..maxillary sinus…..antibiotic…avoid blowing).
Knife edge or irregular ridge:
Painful dentureIncision not on ridge crest but slightly below the crest….sharp edge removed rongeur …smoothed bone file….carful


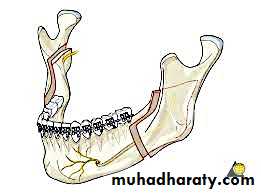
Mylohyoid ridge reduction
Due to bone resorption.
Need surgery :
Mucoperiosteum thin….irritationUndercuts
Displace denture
crestal incision……………flap reflected………
muscle detached………….trim,smooth,…….reattach again ,…with healing).
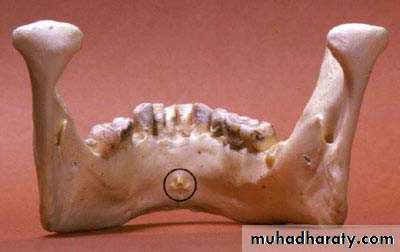
Genial tubercle reduction
Remove or not…act as shelf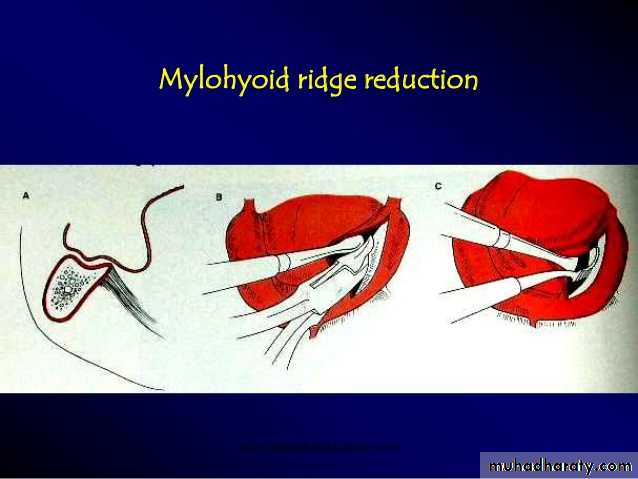
Removal of tori:
Mandibular torus:Interfere full or partially with denture
Ulceration
Interfere with speech if too large
Crestal incision……..flap reflected
osteotome……malleted if clear or bur……stent needed
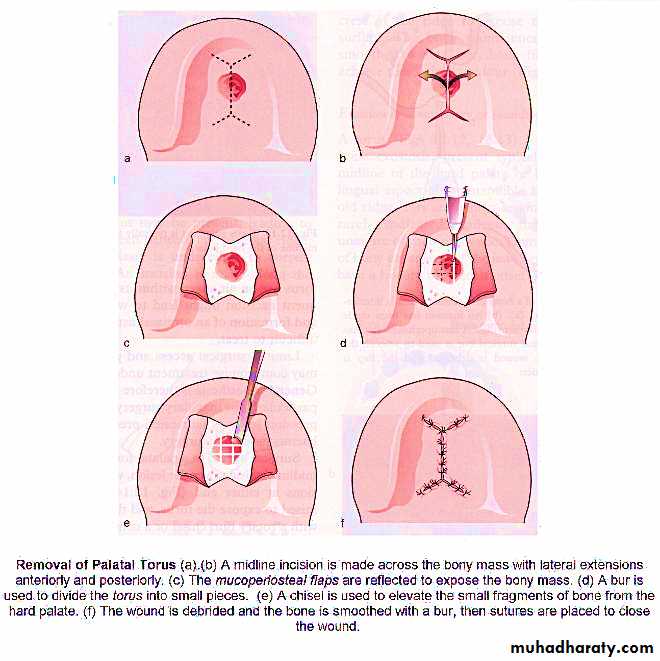
Palatal torus:
Small …ignore …relief
Same as mandibular indication
incisions:
Single midline palatal incision, Y, Horse shoe
Cut with fissure bur…..then use osteotome.. stent

Buccal exostoses:
More maxilla in mandible.if interfere …surgery.
Cleaved with osteotome or removed with rongure, bur.


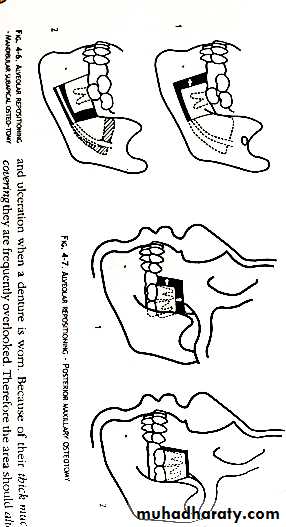
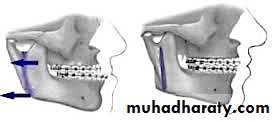
Alveolar repositioning:
Better retention and stability if alveolar bone aligned over basal bone.This is done by separating part or all of alveolar bone and realigning it over basal bone.
Types:Anterior and posterior maxillary osteotomies
Le fort 1 osteotomy
Mandibuler subapical osteotomy
The repositioned segments are fixed using splints or denture held by wires.
Techniques to deal with alveolar atrophy:
A: Technique to reduce alveolar atrophy.
B: Technique to correct the condition.
C: Technique to compensate for alveolar atrophy.
A: technique to reduce alveolar atrophy.
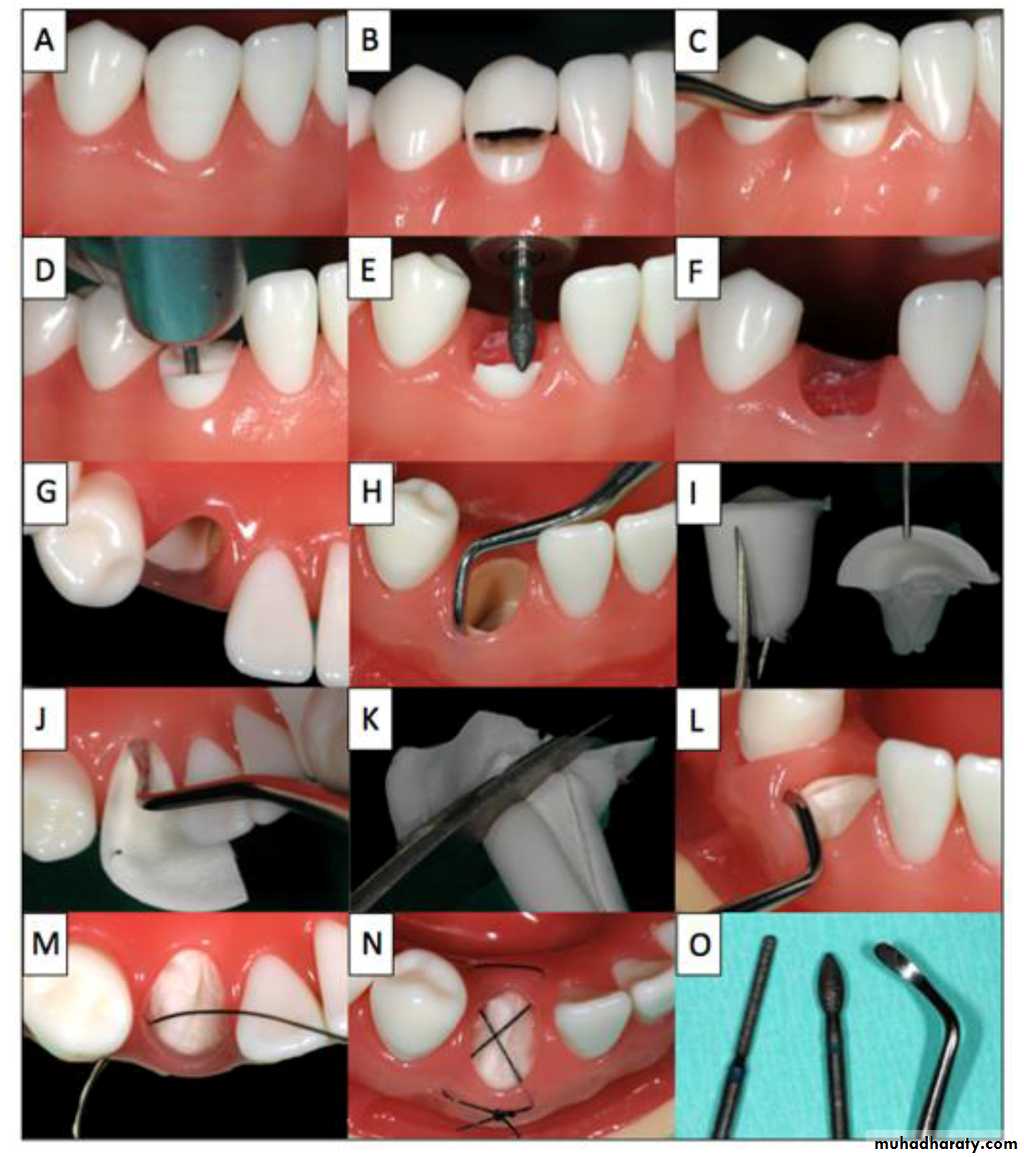
if root left in alveolar …less resorption???Overlay denture:
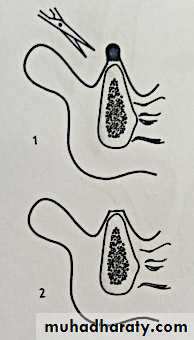
over endodontically treated teeth. Modified. Less resoption.Submucous vital root retention:
root reduced 2 mm below crestal bone…closure of mucosa bone and PDL will grow overDenture after 6 weeks.
Complication…dehiscence ..tension closure…pressure denture.Root cone implant:
Hydroxyapatite root cone implant after exo…less bone resorPtion

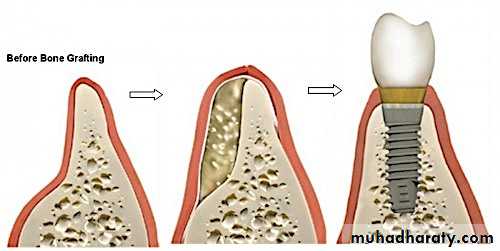
B: Technique to correct the condition:
1.Replacing the lost bone …augmentation.2.Regeneration the lost bone.
Grafting (natural and synthetic)
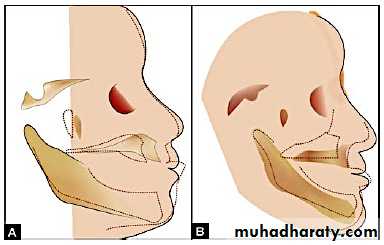
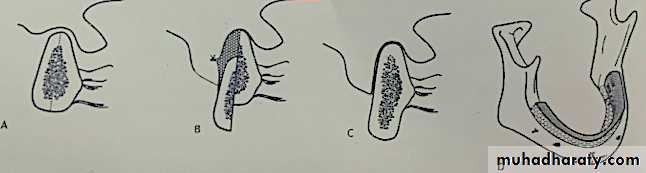
Rib graft augmentation of mandibular ridge.
Rib graft augmentation of lower border of mandible….extra oral incision bone placed….denture immediately can be worn…..scar….face shape change, nerve problem.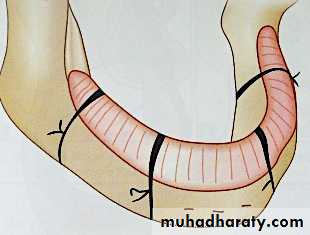
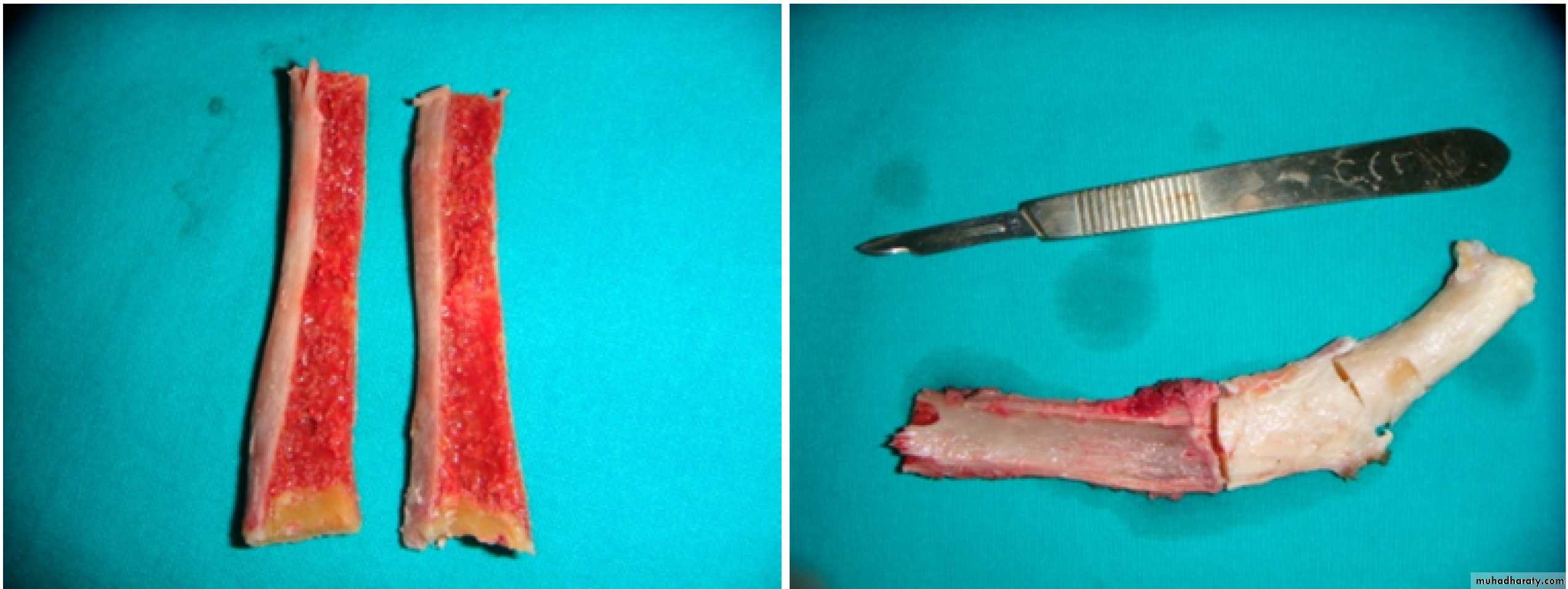

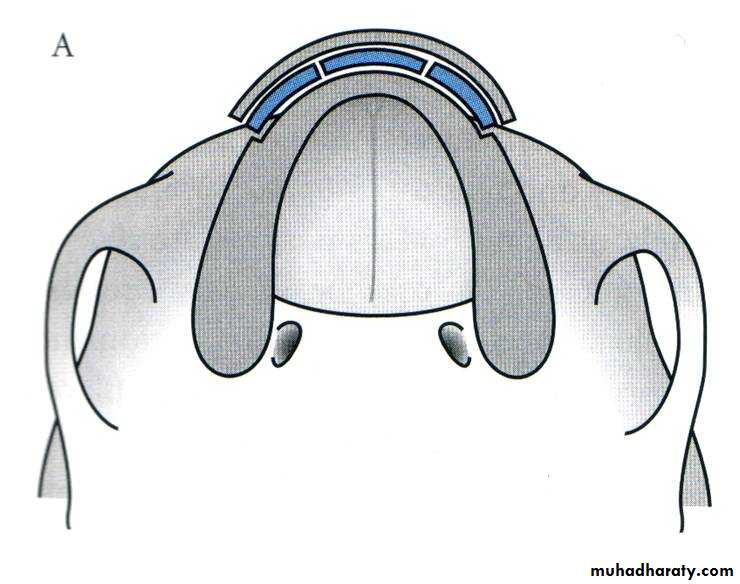
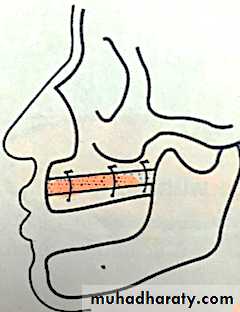
Direct rib augmentation of atrophic maxilla…graft lateral to ridge.
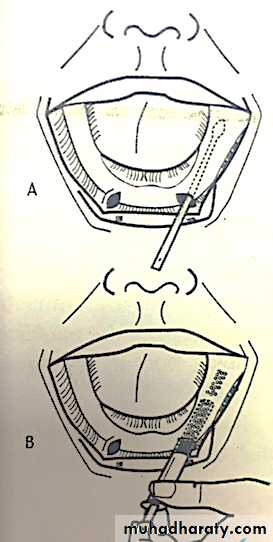
Ridge augmentation with synthetic graft (tunnel):Bilateral vertical incision. Anterior to mental foramen….use syringe inject material….molded by finger.
Labial undercut augmentation of anterior ridge
Augmentation with pedicle and interpositional bone grafts
Horizontal osteotomy …sandwichVertical osteotomy….split…sutured…nerve damage
Combined vertical and horizontal
C: Technique to compensate for alveolar atrophy:
Vestibuloplasty:
Prong denturesZygomaticoplasty
Tuberoplasty
Lowering the mental foramen
C: Technique to compensate for alveolar atrophy:
Vestibuloplasty:a surgical procedure designed to restore alveolar ridge height by lowering muscles attaching to the facial labial lingual aspects of the jaw.
Objectives:
To extend denture bearing surface for retention and support.Reposition muscle attachment from crest of the ridge.
Better functioning of the denture.
Classification:
- Secondary epithelialization:Deepening of vestibule…portion left exposed….wound heals new mucosa formed
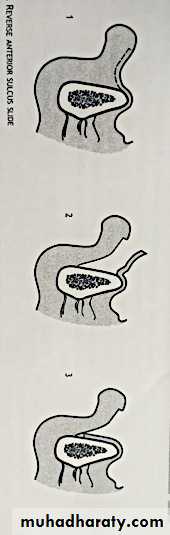
Reverse anterior sulcus slide
Anterior sulcus slideTranspositional flap
two flap repositioned
- Submucosal resection
- Soft tissue graft
Split thickness skin graft
Mucosal grafts ( palatal, buccal)

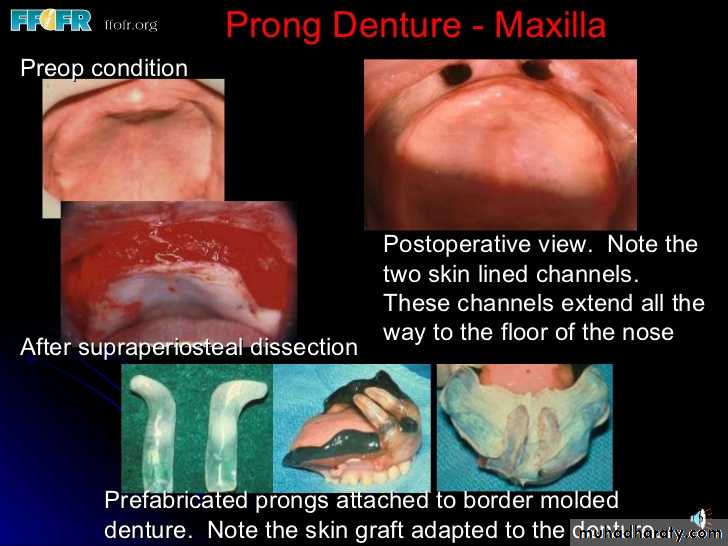
Prong denture
Aid retention of both maxillary and mandibular dentures…..now more in maxillaProcedure :
Involves the creation of two skin lines pockets in which acrylic prongs are placed
Provide lateral stability
Prevent displacement
C: Technique to compensate for alveolar atrophy:
Vestibuloplasty:Prong dentures
Zygomaticoplasty
Tuberoplasty
Lowering the mental foramen
Zygomaticoplasty:
Using bur….cut….Providing height and lateral stability for dentureTuberoplasty:
Provide increased height on the distal aspect ofmaxillary tuberosity …prevent anterior displacement.
Lowering the mental foramen:
Nerve near crest…discomfort….expose nerve…

Surgical procedures.
Preprosthodontic surgical procedures may be described under :Procedures to improve the bony foundation.
Procedures to improve soft tissue foundation.Procedures to improve ridge relationship
Implant procedures
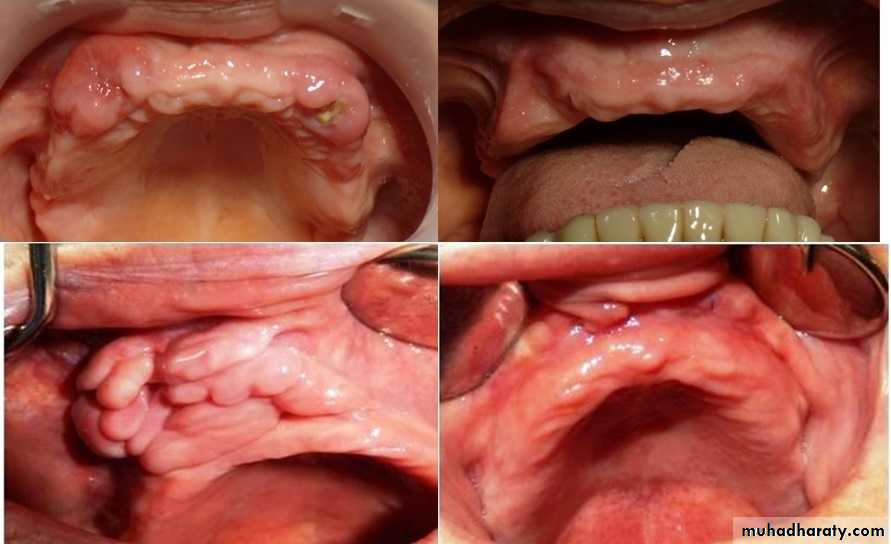
Procedures to improve the soft tissue foundation:
Hypermobile tissue correctionnon surgical modify impression….W.O pressure
Surgical
injection of sclerosing solution…become firm
Fibrous hyperplasia epulis fissuratum
Excision knife, scissors, electrosurgery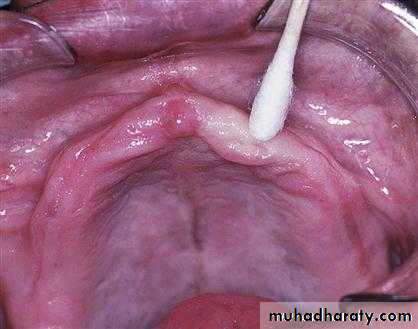

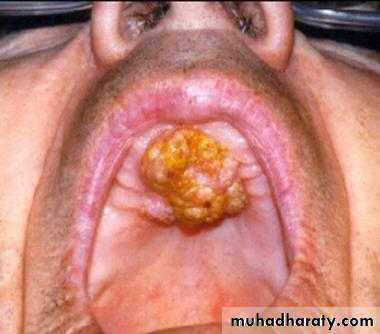
Palatal hyperplasia
(poor hygiene, day and night)(electrosuergery, scraped sharp bone file)
Hyperplastic maxillary tuberosity
Frenectomy
Hypertrophic labial frenumAbnormal lingual frenum
high buccal frenum
Soft tissue lesions. biopsied


Surgical procedures.
Preprosthodontic surgical procedures may be described under :
Procedures to improve the bony foundation.Procedures to improve soft tissue foundation.
Procedures to improve ridge relationship
Implant procedures
procedures to improve ridge relationship:
Maxillary advancement procedures:Le Fort 1 osteotomy with or W.O graft
Maxillary retrusion procedure:
Le Fort 1 osteotomy maxillary repositioned superiorly and posteriorly
Mandibular advancement procedure:
Sagittal osteotomyMandibular retrusion procedures:
Osteotomy of the body of mandibular on ramus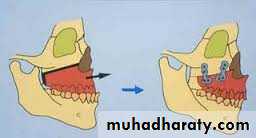
Surgical procedures.
Preprosthodontic surgical procedures may be described under :Procedures to improve the bony foundation.
Procedures to improve soft tissue foundation.
Procedures to improve ridge relationship
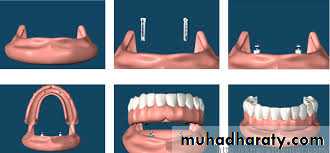
Implant procedures
Implant procedure: