1
st
lecture
Dr. Bushra Rashid

The foundation of practicing dentistry for
children is the ability to
guide them through
their dental experiences.
Previously
named behavior management
In 2003, American association of pediatric
dentistry (AAPD) changed the name into
Behavior guidance
Definition
Variables influencing children’s dental
behaviors
Classifying children’s cooperative
behavior
Parents of pediatric patients
Pre-appointment behavior modification
Fundamentals of behavior guidance
Communicating with children
Retraınıng
enhancing
communication with
the child and parent
to promote a
positive
attitude
and
good
oral health
.

A
major difference
between the
treatment of children and the treatment
of adults is the
relationship.
Treating adults generally involves a one-
to-one relationship, that is, a dentist-
patient relationship. The child patient
relationship resembles a triangle as
follows:
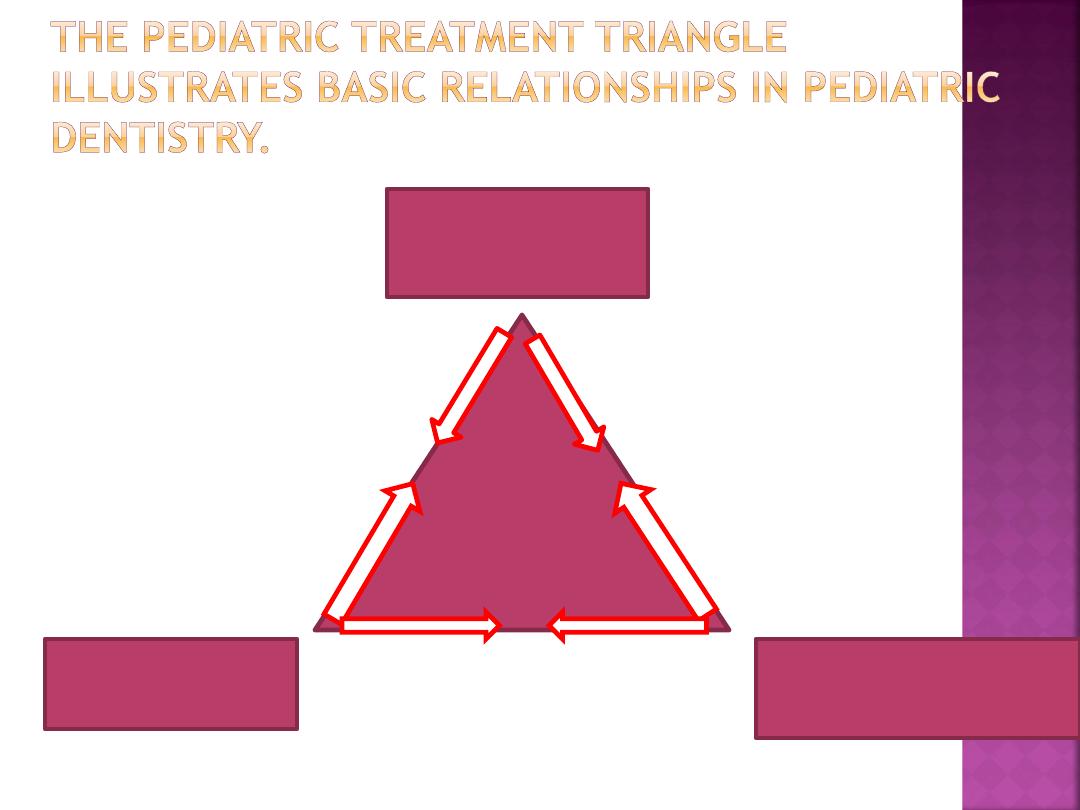
Family
(
mother
)
Dentist and
environment
Child
patient
The key for successful
outcomes is;
appropriately
motivate
the
child and family to prepare
them to actively participate in a
positive manner in the child’s
oral health care.
compliance,
relief of anxiety,
completion of quality
care,
and development of
trusting relationship

VARIABLES INFLUENCING
CHILDREN’S DENTAL
BEHAVIORS
several variables in
children’s backgrounds have
been related to it:
Parental Anxiety
Medical Experiences
Awareness of Dental Problem
General Behavior Problems
1.Wright’s clinical
classification
places children in three
categories:
• Cooperative
• Lacking in cooperative
ability (under 3 years)
• Potentially cooperative
2. Frankl Behavioral Rating Scale
Rating 1: Definitely negative.
Refusal
of treatment
, crying, fearfulness,
or any other overt evidence of
extreme negativism
• Rating 2: Negative.
Refuse
treatment,
uncooperativeness,
some evidence of negative attitude
but not pronounced
( withdrawn)
Rating 3: Positive.
Acceptance of
treatment
; at times with
reservation, but patient
follows
the dentist’s directions
cooperatively
• Rating 4: Definitely positive.
Good rapport
with the dentist,
interest in the dental procedures,
laughter and enjoyment.
Parents of pediatric patients often
require
understanding
and have to
be led through their children’s dental
experiences.
Communication
can mean many
things, but in this instance it refers
to the
dentist’s getting
his or her
message across to the parents
and
having them work with the dentist.
It refers to
anything that is
said or done to
positively
influence the
child’s behavior
before the child
enters a dental
operatory.
1. Films or videotapes have been developed to
provide a model for the young patient.
The goal
is to have the patient reproduce behavior
exhibited by the model.
On the day of the appointment, or perhaps at a
previous visit, the new pediatric patient views the
presentation.

2. Take the child in a tour in the dental clinic


3. Live patient models
such as siblings, other
children, or parents.
Many dentists
allow young children into the
operatory with parents
to preview the dental
experience.
4. Another behavior modification method
involves
pre-appointment parental
education
(1) stimulation of new behaviors.
( like dental brushing, enjoy talking)
(2) facilitation of behavior in a
more appropriate manner.
(like
letting the child move his hand when he feel
non-comfortable)
(3) removal of inappropriate
behavior due to fear.
(when the
child feel comfortable)
(4) extinction of fears.
1. Positive Approach
Positive statements
increase the
chances of success with children.
Like: thank you
2. Team Attitude
A pleasant smile
tells a child that
an adult cares. Children respond
best to a
natural and friendly
attitude.

3. Organization
A well-organized,
written
treatment
plan must be
available for the dental
office team.
Delays
and in decisiveness
can build apprehension in
young patients.

4.Truthfulness
Truthfulness is extremely important in
building
trust;
it is a fundamental principle in caring for
children.
5. Tolerance
Tolerance of the dentist and staff differ from time
to time, it is affected by the several things like an
upsetting experience
at home can affect the
clinician’s mood in the dental office. So
receptionists should book children with behavior
problems the first thing in the morning.

6.Flexibility
Because children are children,
lacking in maturity, the
dental team
must be prepared to change its
plans at times.
A child may begin
fretting or squirming in the dental
chair after half an hour, and the
proposed treatment may have to be
shortened. Thus the dental team
must be flexible
as the situation
demands.
Called:
treatment deferral

COMMUNICATING WITH
CHILDREN
Several effective communication techniques can
be suggested.
1.Establishment of Communication
Involving a child in a conversation
not only enables
the dentist to learn about the patient but also may
relax the child
. differs with the
age
of the child.
Procedure:
1.initiated with complimentary comments,
(e.g: you
are so beautiful)
2.followed by questions that need an answer other
than “yes” or “no
.”(e.g: which cartoon do you like)

2. Establishment of the
Communicator
It is important that
communication occur from a
single source
.
When both dentist and dental
assistant provide directions, the
result may be a response that is
undesirable simply because the
child becomes confused.

3.Message Clarity
Communication is a complex,
multisensory process. It includes a
transmitter, a medium, and a receiver.
The dentist
or dental health team is the
transmitter
,
the
spoken word
frequently is
the
medium
,
the
pediatric patient
is the
receiver
.

Very often, to improve the
clarity of messages to young
patients, dentists use
euphemisms to explain
procedures.
For pediatric dentists,
euphemisms or word substitutes
are like a second language.
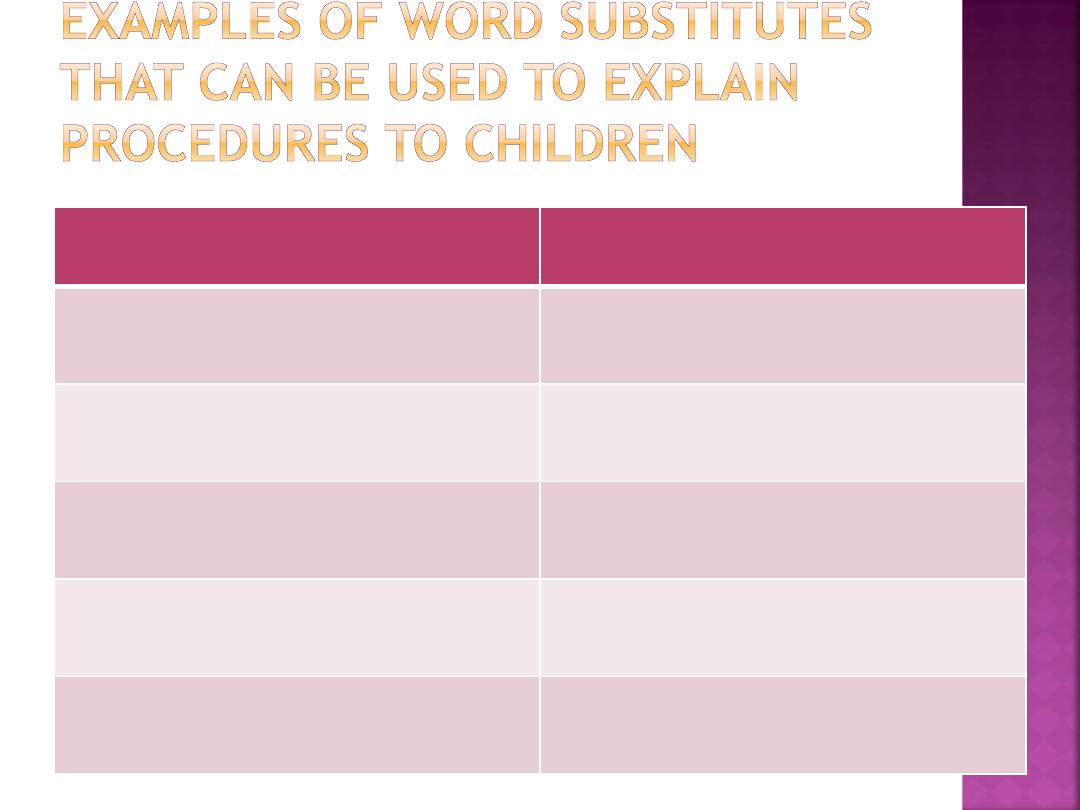
DENTAL TERMINOLOGY
WORD
SUBSTITUTES
Band
Tooth ring
Retainer
Tooth button
Sealant
Tooth paint
Fluoride varnish
Tooth vitamins
Air syringe
Wind gun
Water syringe Water gun
Suction
Vacuum cleaner
Alginate
Pudding
Study models
Statues
High speed
turbine
Whistle
Low speed
handpiece
Motorcycle

.4.Voice Control
Sudden and firm commands are
used to get the child’s attention or
to stop the child from whatever is
being done.
A sudden command of
“Stop
crying and pay attention!”
may be
a necessary preliminary measure
for future communication.
5. Multisensory Communication
Nonverbal messages
also can be sent to patients.
Body contact can be a form of nonverbal
communication.
The dentist’s simple act of placing a hand on a
child’s shoulder
while sitting on a chair-side stool
conveys a feeling of warmth and friendship.
This type of physical contact helped children to relax,
especially those 7 to 10 years of age.
Eye contact
is also important.
The child who avoids it often is not fully
prepared to cooperate.
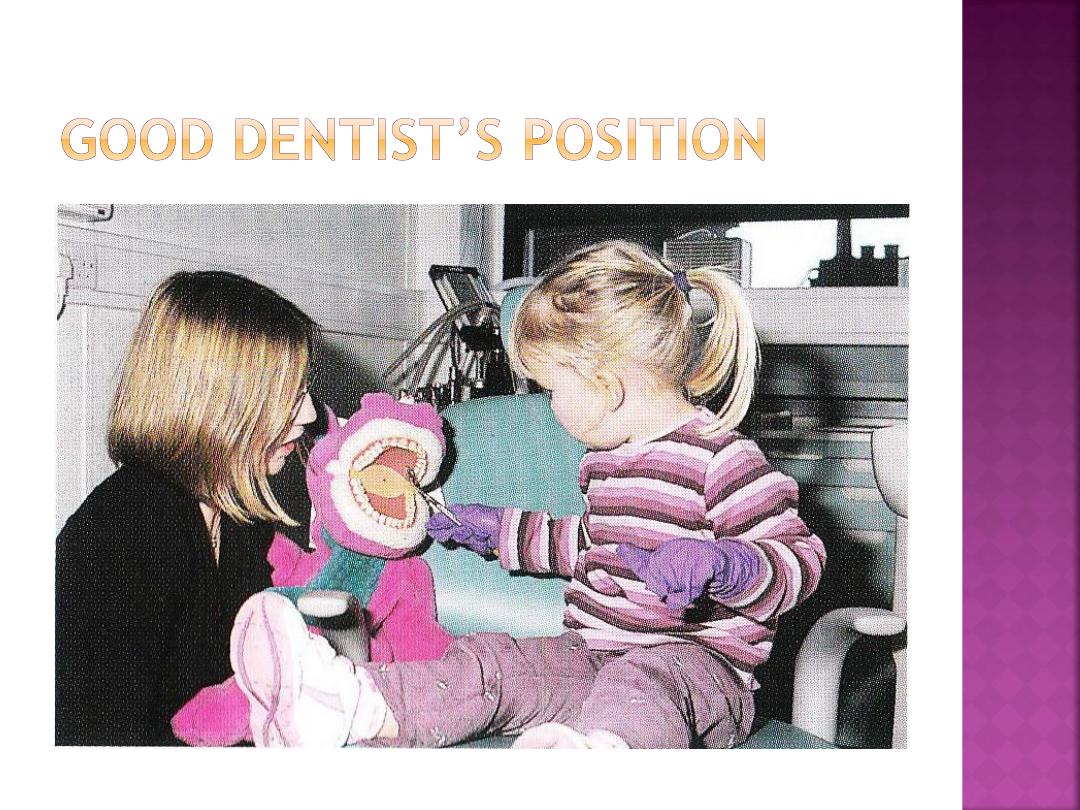
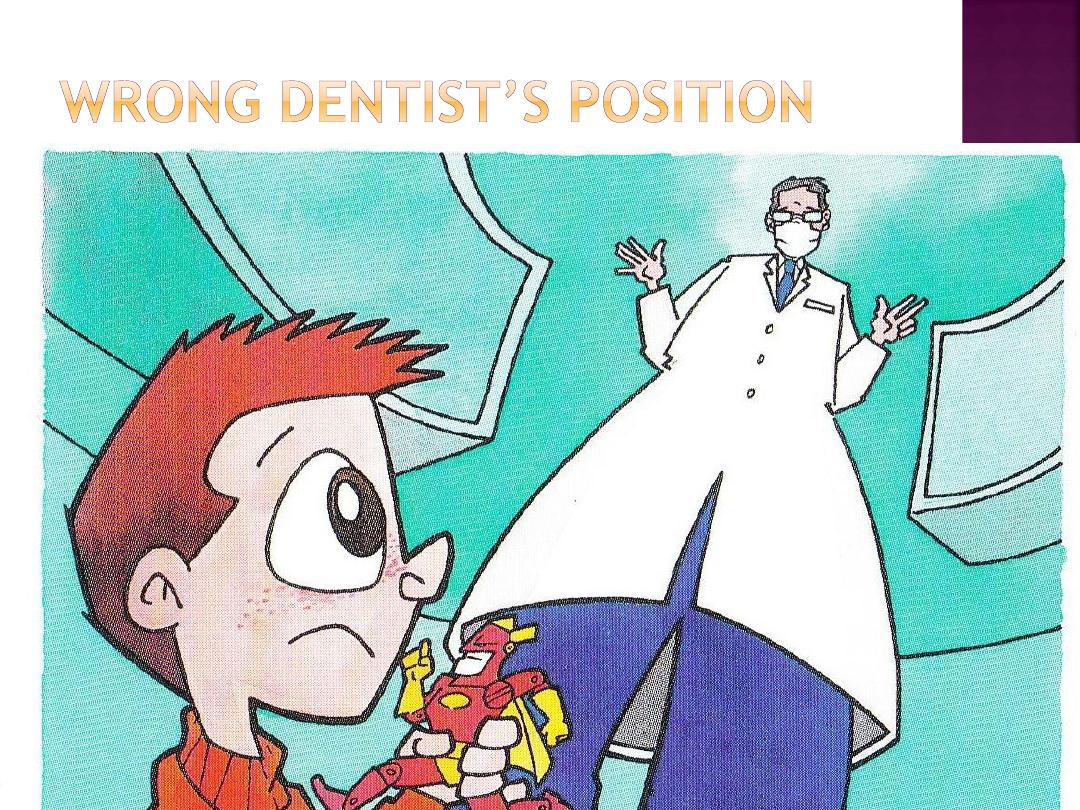
When the dentist talks to children, every
effort should be made
not to tower
above them
.
Sitting and speaking at
eye level
allows for friendlier and less
authoritative communications.
6. Problem Ownership
Sometimes dentist forget he is
dealing with a child patient
There are negative messages only
which only undermine the rapport
between a pediatric patient and
dentist shouldn’t use them:
Example
“you” messages. For
example, “You must open your
mouth wide!”
An alternative
is to send
“I” messages
.
These messages establish
the focus of the problem,
such as “
I can’t fix your
teeth if you don’t open your
mouth wide.”
7. Active Listening
Listening also is important in the
treatment of children.
However, listening to the
spoken words
may be more important in establishing
rapport with the
older child
.(over ten)
While establishing
rapport with younger
child,
with nonverbal
behavior often is
more crucial. (7-10 years)
stimulate the child to express feelings,
and the dentist does the same,
as
necessary processes in communication.

8. Appropriate Responses
The response should be
appropriate to the situation
It depends primarily on:
1. extent and nature of the
relationship with the child.
2. the age of the child.
3. evaluation of the motivation
of the child’s behavior.
An inappropriate response would be
a dentist’s displaying extreme displeasure with
an anxious young child on the first visit
when
there has been insufficient time to establish a
good rapport.
The appropriate response is
if
a dentist has made inroads with a child
, who
then displays unacceptable behavior,
a dentist
may well express disapproval without losing
personal control..
Definition, it is that procedure which very
slowly develops behavior by
reinforcing
successive approximations of the desired
behavior
until the desired behavior comes to
be.
the dental assistant or dentist is teaching a
child how to behave.
The child has to be communicative and
cooperative to absorb information
1. State the
general goal
or task to the child at
the outset.
2. Explain the necessity for the procedure
. A child
who understands the reason is more likely to
cooperate.
3.
Divide the explanation for the procedure.
Children cannot always grasp the overall
procedure with a single explanation;
consequently, they have to be
led through the
procedure slowly.

4
. Give all explanations at a
child’s level
of
understanding.
5.
Use euphemisms appropriately
. Dentists
should demonstrate various instruments
step by step before their application by
telling, showing, and doing
. When the
dentist works intraorally, a pediatric
patient should be shown as much of the
procedure as possible, here
tell-show-do
method
can be used.

6.
Reinforce appropriate behavior
. Be as
specific as possible, because specific
reinforcement is more effective than a
generalized approach.
7. followed by
reductions in children’s fear-
related behaviors
. e.g; are you ok? Or do you
feel fine?
8.
Disregard minor inappropriate behavior
.
Ignored minor misbehavior tends to
extinguish itself when it is not reinforced.