HIV Infection and AIDS
د. رزان
• To define HIV& AIDS.
• Enumerates the modes of transmition.Demonstrate the clinical presentation.• Outline the management.
• Contribute to AIDS prevention.
Objectives :

HIV Infection and AIDSDefinitions:
HIV infection: infection with the human immunodeficiency virus HIV-1or HIV-2 retroviruses.
AIDS: Acquired immunodeficiency syndrome—AIDS is the final stage of HIV infection. AIDS is diagnosed when a person with HIV has a CD4 count of less than 200 cells/mm3 and/or one or more AIDS-defining illnesses.
EFFECTS ON LIFE
• AIDS is a life long problem.• Mortality is high.
• Diagnosis is usually late.
• Its a syndrome that contain many diseases like infections and tumours.
• Multiple routs of transmission.
• It is sexually transmitted.
• Transmittable to the off springs.
CONT.
• It affects patient’s work performance and productivity.• It is a social stigma, and related to sin.
• It affects the patient psych .
• Treatment is difficult because it is very expensive if available! and not that effective.
• Over burden the community.
• Nationally alarming!.

THE CAUSATIVE AGENTS OF AIDS:
HIV-1 and HIV-2 (the latter mainly found in West Africa) are retroviruses.
From the lentivirus group.
They are single-stranded RNA viruses.
Employing reverse transcriptase
which allows incorporation of the virus into cell's DNA.
Extremely high spontaneous mutation rate associated with reverse transcriptase
copying .
Causative Agents:
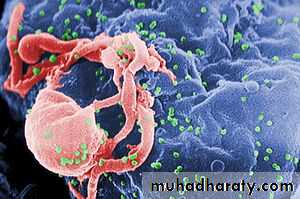
Affinity for CD4 cells .The virus infects and depletes helper/inducer CD 4 T-lymphocytes,
leading to loss of cell mediated immunity and opportunistic infection.
فيروس HIV-1 (باللون الأخضر) في خلية ليمفاوية
Methods of transmission:
HIV is spread by infected body fluids e.g. blood or semen. Methods of transmission are multiple and difficult to control :1-Sexual contact: Most common; male homosexuals still a risk group.
2- Perinatal: During birth or by nursing; About 20-50% of infants born to HIV-infected women have HIV disease.
3-Transfusions: Risk of receiving HIV-infected blood when no proper screening procedures used.
4-Organ transplantation.
5-Blood inoculation: Shared needles among drug abusers;
improper sterilization of instruments; injuries to health care workers and laboratory personnel (usually needle stick).
The high risk groups
The major risk groups are for HIV-are:• Male homosexuals (initial major risk group).
• Intravenous drug abusers.
• Sexual contacts of HIV individuals.
• Recipients of HIV contaminated blood or organs (now very low risk; but in early days of epidemic, devastating affect on hemophiliacs).
• Infants born to HIV infected women.
• Those who have multiple sexual parteners (weather homo,hetro or bisexual)especially with unprotected sexual practice.
• Frequent travelers.
The seronegative window
The first 3-6 months of infection during which the patient is negative by antibody dependant screening investigations.The acute infection may be symptomless
in 50% of cases.HIV infection may be asymptomatic for several years.
mean latent period between infection
and the development of AIDS is 10Years.
after Five years of HIV infection, 15% will have progressed to AIDS.
but two-thirds of the remainder will be asymptomatic.
Group
Skin signs1 (Primary
phase).II (Early phase:
asymptomatic).
III (Persistent generalized
.lymphadenopathy]IV(Symptomatic
AIDS)Transient maculopapular eruption.
Hypersensitivity reactions, viral warts and fungal infections.Herpes zoster, candidiasis, eczemas,
.Kaposi's sarcomaOpportunistic infections, Kaposi's sarcoma, lymphoma.

presentation:
In the early stages of symptomatic infection: ,Fatigue
Weight loss
Fever
Diarrhoea
Skin changes
Generalized lymphadenopathy.
are present without the opportunistic
infections which define AIDS.
1-NON INFECTIOUS CUTANEOUS FINDINGS.Seborrhoic dermatitis.

Opportunistic infections
Are nusual and difficult to control.Opportunistic organisms include:
Mycobacterium avium complex.
Pneumocystis carinii.
Cryptococcus neoformans.
Toxoplasmosis.
Cytomegalovirus.
And others...

Candidiasis
Viral warts


Molluscum contageosum
TUMERS:Kaposi's sarcoma
( a multicentric tumour of
vascularendothelium)
Lymphoma.
Encephalopathy may develop.

Underestimation:
The magnitude of AIDS problem including incidence, prevalence, complications and sequelae is not well understood and is underestimated especially in the developing countries.Population knowledge about AIDS is limited.
Efforts to reduce and control the AIDS problem are limited.
Patients may hesitate to seek medical help because AIDS is associated with behaviors which are socially, culturally and legally unacceptable.
AIDS have not received the priority it deserves, and not given due attention.
.Case detection:
H.I.V requiers along list of investigations to acheive the diagnosis and asses the condition (that’s if available it would be very costly)
ELISA test for screening;
Western blot: confirmation.
(Two different blood specimens must be positive)
Negative test: possibility of an HIV infection acquired in last3–6months is not excluded.
More sensitive tests searching for HIV RNA
Viral load (copies/mL.):• RNA–PCR.
• branched DNA signal amplification assay (b-DNA-SA).
• nucleic acid sequence based amplification (NASBA).
HIV resistance analysis (genotypic):
CD4, CD8 lymphocyte account and ratio.
liver function tests (LFTs), electrolytes, renal function test
full blood examination (FBE)
serologic tests for syphilis
Hepatitis A serology
Hepatitis B serology
Hepatitis C serology
HSV type 2, EBV, CMV, toxoplasmosis serology
G6PD in case future use of sulphonamides is required.
Pap smear every 6-12 monthly.
Subsequent routine 3-6 monthly follow up.
*
FBE, CD4/CD8 lymphocyte surface markers, HIV viral load, LFTs,
electrolytes, renal function tests.*
amylase, CK, lipase,to check for medication side effects if on HAART
*when the CD4 count falls below 100, regular screening for MAC
should be performed (/Mycolytic F/)*
Pap smear should be performed 6-12 monthly, more frequently as CD4
count declines*
STD check should be included if relevant symptoms exist or if
exposure has occurred.

The treatment
there is at least 10% primary resistance among new infections in Europe.Patient are to be managed in departments with special experience in HIV disease.
The drug treatment are not always avilable.
drugs are expensive. Treatment is still unavailable to the vast majority of people living with HIV (PLWH). Only 1% of the 4.1 million sub-Saharan Africans with HIV receive anti-HIV drugs.
Not always effective.
Combination therapy is required.
A lot of side effects.
Need for close follow up.
Therapeutic agents:
Three classes of therapeutic agents are available• Fusion inhibitors block the entry of HIV into cells.
• Reverse transcriptase inhibitors (RTI) block the translation of viral RNA into DNA.Three types ----nucleoside analogs (NRTI)
• -nucleotide analog (NtRTI
• -nonnucleoside inhibitors (NNRTI).
• 3. Protease inhibitors (PI) block the maturation and discharge of new viral particles
Reverse transcriptase inhibitors
Nucleoside analogues (NRTI): Zidovudine, stavudine, didanosine, lamivudine, abacavir.
Nucleotide analog (NtRTI) TenofovirNonnucleotide reverse transcriptase
inhibitors (NNRTI):Nevirapine, delavirdine
Protease inhibitors Saquinavir, indinavir, ritonavir, nelfinavir, amprenavir, fosamprenavir.

Medical intervention is by highly active antiretroviral therapy (HAART)
(COMPINATIONS OF reverse transcriptase and protease inhibitors ),the prophylaxis of opportunistic infection
and general support including early treatment of Infections and tumers
The mortality:
Ten years after infection:50% will have developed AIDS,
of whom 80% will have died.
After AIDS has developed, mortality is high, with 50% dying in1 year,
and 85% in 5 years.
No vaccination.
NO effective pre-exposure prophylaxis:
PREVENTIONS:• Improve population knowledge about AIDS.
• Encourage voluntary counseling.
• Widening the screening program to include:
• every person enter from out side the country.
• And any person with STD, health workers at risk.
• HIGH INDEX OF SUSPECSION is required to detect HIV.
• Provide privacy during counseling.
• Develop departments with special experience in HIV disease.

Thank you

Thank you