Neuromylitis optica(Devic disease)
NMO is an immune-mediated demyelinating disorder consisting of a severe myelopathy that is typically longitudinally extensive, meaning that the lesion spans three or more vertebral segments.It is demylinating disorder affecting female more than male
It is autoimune disease affecting B-cell mediated immunity (MS affecting T-cell)It is 2 types monophasic or relapsing
Aggressive inflammatory disorder consisting most typically:
attacks of acute ON and myelitis. Attacks ofON can be bilateral (rare in MS) or unilateral; myelitis
can be severe and transverse (rare in MS) and is typically:
longitudinally extensive, involving three or more
contiguous vertebral segments. Attacks of ON may be
precede or follow an attack of myelitis by days, months,
or years, or vice versa.
Clinical criteria of NMO:
4 of the followings:1-optic neuritis bilateral or unilateral
2-transverse myelitis
3- MRI spinal cord hyperintense lesion in more than3 vertebral segment and it is contageous
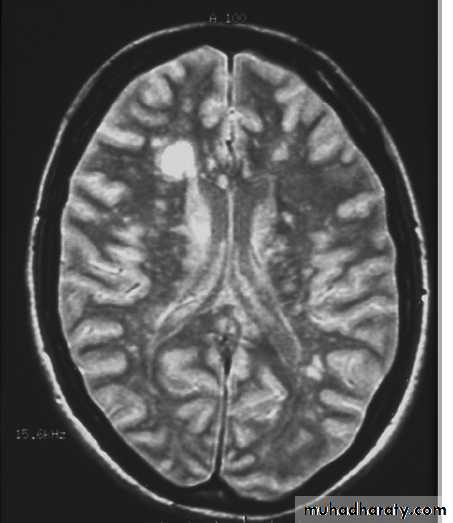
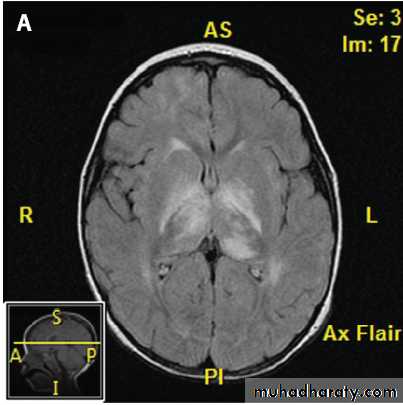
4- MRI brain normal or lesions not that area of ms like in area postrema of medulla ,hypothalamus …
5- +ve serum and or csf aquaporine 4 antibody
Up to 40% of patients have a systemic autoimmune disorder, often systemic lupus erythematosus, Sjِgren’s syndrome, p-ANCA (perinuclear antineutrophil cytoplasmic antibody)–associated vasculitis, myasthenia gravis, Hashimoto’s thyroiditis
This disease is idiopathic or may be triggered by
- Varicella virus-herpers simplex virus
-upper respiratory tract infection
-HIV
-paraneoplastic (very rarly)
-sero+ve patient more laible for relapses

Clincal features
Transverse myelitis --bilat. Lower and/or upper limbs weakness (spastic form) ,bilat babanski signs with sensory level at the site of lesions and incontenance .Optic neuritis unilat. Or bilat.
Other features like : vomiting,hiccup,hypothermia,encephalopathy ,syringobulbia
Investigations
MRI spinal cord and brain
CSF - protien high, sugar normal ,cells mildly elevated contain neutrophile and lymphocyte
Serum and csf aquaporin 4 AB +VE
ANA may be +veTreatment
Iv infusion methyl pridnisolone 500- 1000 mg per day for 3-5 days- Plasma exchange 20 cc/kg per session for 5 sessions on each other day
-iv immunoglobuline 400mg/kg per day for 5days
If pt. not responding to steroid we can use PE immediately (PE rescue)
-after treat the acute attack by above treatment ,we prevent the relaps by Rituximub (anti CD20)
-physiotherapy and symptomatic treatment
Prognosis
Female favourable prognosisRelapsing form favourable prognosis
+ve aquaporine 4 AB good prognosis
Male bad prognosis
Monophasic bad prognosisSero-ve bad prognosis
Acute disseminated encephalomylitis(ADEM-It is autoimmune demylinatind disorder
-triggered by viral infection like :meseales,varicella zoster,influenza virus or due to vaccine like meseales vaccine-the diseae affect male and female equaly , affecting all age group
-it is monophasic but sometimes it is relapsing or recurrent after months or years in 30 % of cases specially in pediatric age groupClinical features
-optic neuritis (unilateral or bilateral)-Transvers mylitis which is complet while in MS it is partial
-Rt. Or Lt. hemiparesis
-Meningism
-Encephalopathy may be present
-Fever may be present
-Seizure
-Heperreflexia or areflexia with babanski sign
-incontence of urine
-Cerebellar sigs may be present specially if due to varicella zoster
-The course of illness varies may lasting weeks to months .
-Sometimes the disease is devastating and may lead to high
mortality in type called acute hemorragic leukoencephalitis-In general it has benign course and the curable rate was 80%
- It is monophasic but sometimes it is relapsing or recurrent speciaily in childrenDiagnosis
--Clinically some manifestation mimic MS but associted with encephalopathy (confusion ,drowsiness)--MRI brain show demylinating plaques differ from that of MS plaques by it is larger, confluent, affect white and gray mater(basal ganglia and thalamus) and sotimes it is symetrical with contrast enhacement
--CSF analysis may show increase protein, lymphocytic pleocytosis and normal sugar and sometimes +ve oligoclonal bands , sometimes csf normal.
Treatment
--IV methyl prednisolone 1 gram per day for 5 days if child the dose is 20-30 mg/kg day for 5 days the steroid given in infusion--Plasma exchange specially if not responding to steroid
--IV Immunoglobuline (IV.IG)
--physiotherapy and cardiorespiratory support
Transverse myelitis
It is disorder of spinal cord affecting cervical, thoracic, or upper lumber segment (L1) spinal cord ends at LI in adult and L2-3 in childrenCauses :
1- compresive (tumor, disc , hematoma , abcess)
2-demylinating (MS , ADEM, NMO)
3- inflamatory like ( SLE , antiphospholipid)
4-toxines
5-nutrisional like B12 diffeceny
6- infectious and post infectious like post respiratory tract infection
7- idiopathic
Clinical features
--Paraparesis or plagia or quadriparesis
--Sensory level at the site of lesion and (loss of sensation below the level of lesion like patient loss all sensory modality till the level of umbilicus--D10)
--Incontence of urine and or faeces
--hyperreflexia and bilat. Babanski sign
--if cervical cord affected respiratory compramisation may occur
-
Diagnosis
--Cinically--MRI CORD to exclude compresive lesion and to look for any hyperintese lesion increase signal intensity in T2 image
--Sometimes MRI normal specially in post infectious cause , normal MRI does not exclude the diagnosis
--CSF may be needed specially in infectious cause CSF PCR for infectious cause otherwise csf is normal ,sometimes only increase protein mildly with mild increase in lymphocyte
--Vasculitic screen (ANA, C- ANCA , P- ANCA, ANTIds DNA AB…..)
Treatment
1-If there is compressive lesion treat it surgically , if no surgical lesion (for other causes) you can give --2-Steriod (MP --- 1 gm per day ) for 5 days
3- plasma exchange if not responding to steroid
4-IVIG
5-Treat the underlying cause
6-Physiotherapy , elastic stocking and prophaylactic heparin to prevent DVT.