The Lacrimal System
Anatomy1.The puncta
2.The canaliculi
3.lacrinal sac
4.Nasolacrimal duct
Causes of watering Eye
1.hypersecretion secondary to ocular inflammation and surface disease.2.defective drainage
a.Malposition of the lacrimal puncta e.g. secondary to ectropion
b.obstructionany where along the lacrimal drainage system.
3. lacrimal pump failureObstruction
1.primary punctual stenosis . seen in :a.infections e.g. herpes simplex and trachoma
b.post irradiation for malignant lid tumors.
c.cicatrizing conjunctivitis.
2.secondary to medial ectropion .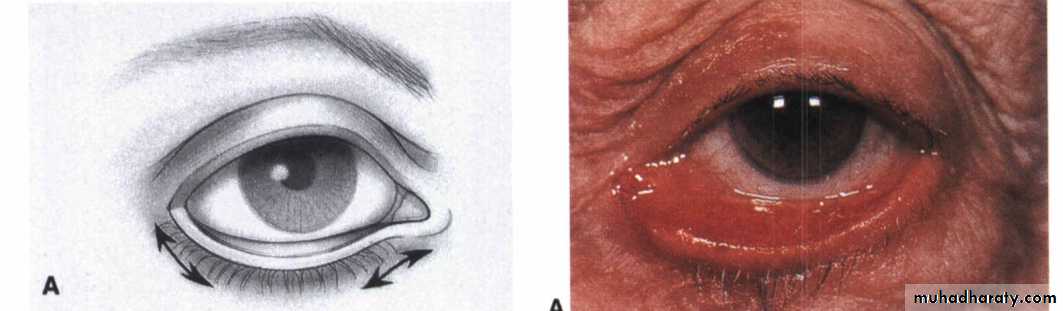
Treatment:
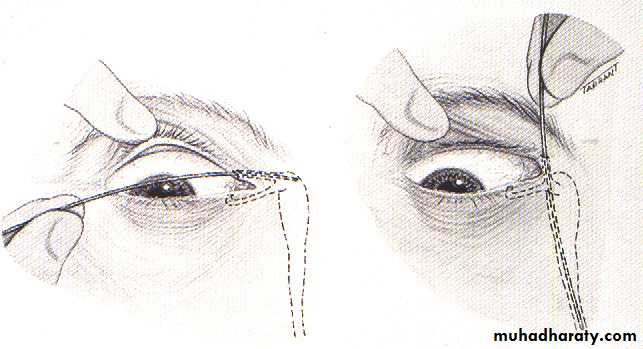
1. For primary punctual stenosis dilatation with nettleship dilator or punctoplasty.2. For the secondary punctual stenosis:
a.Zeigler cautery burns to the medial palpebral conjunctiva 5mm below the punctum.
b.medialconjunctivoplastyCanalicular obstruction
Causes are similar to those of primary punctual stenosis.Treatment:
a.partial obstruction treated by intubation.
b.total obstruction may be treated with canaliculodacryocystorhinostomy (CDCR).
nasolactimal duct obstruction
causes :
1.idiopathic is by far the most common.
2.secondary
a.nasoorbital trauma.
b.wegenergranulomatosis
c. infiltration by nasopharyngeal tumours.
Treatment:
Dacryocystorhinostomy.
Congenital nasolacrimal duct obstruction(delayed canalization)
It result from delayed canalization of the nasolacrimal duct at the valve of Hasner.Present with Epiphora and matting of the lashes ,starting soon after birth.
Treatment:
1.massage of the lacrimal sacand duct.2.probing :this should be delayed until the age of 12 months because spontaneous canalizationoccurs in about 95% of cases.
Dacryocystitis
acute or chronicmost commonly staphylococcal or streptococcal.
Acute dacryocystitis
Usually secondary to nasolacrimal duct obstruction
Treatment
Systemic antibiotics and warm compresses
DCR after acute infection is controlled
Chronic dacryocystitis
Epiphora and chronic or recurrent unilateral conjunctivitisTreatment - DCR
Dry Eye
The Tear filmIt has three layers:
1.Outer Lipid layer secreted by the meibomian gland
2.Middle Aqueous Layer secreted by the main and accessory lacrimal glands.
3.Inner Mucin secreted by the conjunctival goblet cells
classification
(a)hyposecretive (Sjogren or non-Sjogren)1.Sjogren
a. Primary is associated with a dry mouth (xerostomia) and auto-antibodies.
b.Secondary is associated with a systemic autoimmune connective tissue disorder :
1.Rheumatoid Arthritis
2. SLE
3.Psoriatic arthritis
4.Dermatomyositis and polymyositis
2.non-Sjogren e.g.age related
(b) evaporative
a. Oil deficiency secondary to meibomian glands dysfunction e.g. posterior blepharitis
b.Defective resurfacing as a result of abnormal lid-globe congruity or defective blinking.
DiagnosisSymptoms include irritation, foreign body sensation, burning, presence of stringy mucous discharge and transient blurring of vision.
Signs include abnormal tear minscus and inferior punctate corneal epithelial erosion.
Treatment
1. patient education regarding the avoidance of environmental factors and toxic drugs that may exacerbate the symptoms .2. tear substitutes in the form of tear drops,gelor ointments
3. topical cyclosporine (0.05%,0.1%) reduces cell mediated inflammation of lacrimal tissue.
Done by Omar Abid ALsamrrae
^_^ as simple as life