Management of Bleeding Disorders in the Dental Practice: Managing Patients on
AnticoagulantsThe normal haemostasis process involves three stages:
1. Vascular spasm2. Platelet plug formation: platelets adhere to the exposed blood vessel surface. The adenosine disphosphate (ADP) helps platelets become sticky and aggregate to form a plug which helps to reduce the amount of blood loss.
3. Clotting: which involves two pathways, intrinsic and extrinsic, and results in the formation of thrombin which converts
fibrinogen to fibrin and forms a clot that stops blood loss.
For normal homeostasis to be achieved,
four biological factors should be intact:1. Adequate platelet numbers;
2. Normal platelet functions;
3. Normal blood vessels; and
4. Adequate clotting factors.
Accordingly, bleeding disorders:
Coagulation disorders;
Vascular defects;
Platelet number defects; and
Platelet FUNCTION defects.
This, of course, is in addition to other complementary factors such as
fibrinolytic defects and other acquired factors
In general, anticoagulant medications are prescribed for prophylaxis (eg prevention of deep vein thrombosis
(DVT), pulmonary embolism (PE) in high risk
patients or prevention of strokes in chronic
AF or prosthetic heart valves), or therapeutic
treatment of venous thrombo-embolic
disorders like DVT or PE
Common anticoagulants used innthe UK include (in order of the most common):
aspirin, warfarin, clopidogrel, dipyridamole andheparin.
• Patients on warfarin
Warfarin is commonly prescribed for prophylaxis or therapeutic treatment of thrombo-embolic disease and arrhythmiasIt acts as a vitamin K antagonist so it affects
the synthesis of active factors II, VII, IX, X and protein C.
This process takes 3 to 4 days and it
prolongs both the prothrombin time (PT) and
To less extinct activated partial thromboplastin time (APTT).
Warfarin effects are delayed for 12 to 36 hours and last for 72 hours and
Antibiotics are of particular importance as dentists may prescribe them post-operatively. Broad spectrum antibiotics can change the intestinal flora that may decrease absorption of vitamin K and thus the international normalized ratio
(INR) will be prolonged.
The PT measures the effectiveness of the extrinsic and common pathways. The normal value is approximately 10 to 15 seconds.
Because of the variability in PT reported by different laboratories, the World Health Organization recommends the use of the INR for reporting PT values. The INR
is calculated by: patient PT/control PT. The
normal INR is approximately 1.
The usual therapeutic range for INR is from 2 to z
Disorder Therapeutic Range
Pulmonary embolism 2−3Atrial fibrillation 2−3 Post myocardial infarction 2.5−3.5
Mechanical prosthetic heart valves 3−4
An INR above this range may
increase the patient’s risk of a spontaneousor surgically induced bleeding episode, while
an INR below the desired therapeutic level
increases the risk of a thrombo-embolism or
ischaemic cerebrovascular event
Pre-operative assessment
Dentists need to do extensive assessment before any dental treatment is undertaken and that should include a detailed medical history, finding out why the patientis on anticoagulants and whether the medical
condition is stable. Dentists also need to check whether the INR history is stable or erratic and discover how long the patient has been stable on warfarin. Any other medical problems
should also be assessed (eg liver disease, diabetes) as all such conditions will affect the decision on how to manage the patient. The difficulty of the oral surgical procedure should
also be assessed
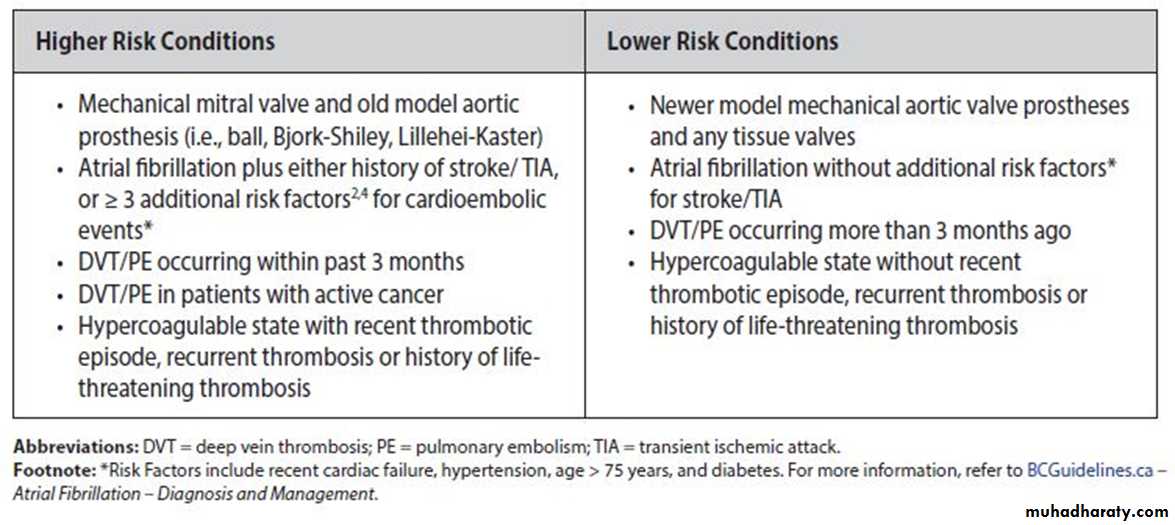
Low risk
Atrial fibrillation without stroke,
cardiomyopathy without atrial fibrillation,
venous thrombosis more than six months
earlier,
were considered to be low risk conditions
High risk
Mechanical mitral valve, ball-cage valve replacement,venous thrombosis less than three months earlier,
Hypercoagulable state,
atrial fibrillation with history of stroke,
acute myocardial infarction less than three
months earlier and
recent (within one month) stroke or transient ischaemic attack were
considered to be high risk conditions.
The risk of a thrombo-embolic event resulting from any of these conditions
if warfarin was stopped should be weighedagainst the risk of post-operative bleeding if
warfarin was continued. Stopping warfarin
for two days increases the risk of a thromboembolic
event by 1%.
Bleeding complications do not carry the same risks as a thromboembolic complication (permanent disability or death)..
The INR should be checked within
24 hours of the planned surgical procedure
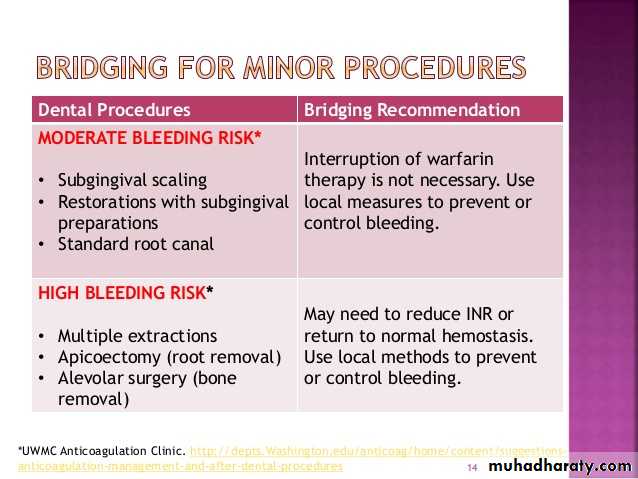
and, if INR values <4 and the oral surgery
procedure is simple (Table 4), the procedure
can be performed without adjusting the
warfarin and any excessive bleeding can
usually be managed by local measures.7
If the patient needs more than
a simple extraction, or if there are other risk
factors involved (eg complicated medical
history, history of erratic INR), the patient
should be referred for treatment in a hospital
setting.
However, if the patient has an INR
value >4, he/she should be referred to thephysician for evaluation. An INR greater than
4.0 is usually considered non-therapeutic,
and the patient is at risk of a serious bleeding
complications
Intra-operative
Infiltrative local anaesthetic
techniques should be used, while regional
local anaesthetic injections (ie inferior dental
block) should be avoided, if possible may cause bleeding that may extend down
the neck.
Surgical procedures should be carried out with
minimal trauma to the bone and soft tissue as
this reduces the risk of bleeding during or after
the operation.
Minimal bone
should be removed and the teeth should besectioned for removal where possible.
Intra-operative bleeding can
usually be managed by local measures such aswound compression with wet gauzes, packing
of resorbable gelatin sponge/resorbable
oxidized cellulose and tight multiple sutures.
The resorbable gelatin sponge and resorbable
oxidized cellulose inserted into the extraction
socket prior to suturing acts as a mechanical
matrix to facilitate clotting and helps to reduce
the incidence of post-operative bleeding.2
Tranexamic acid solution is a
topical antifibrinolytic that is commonly used
to prevent excessive haemorrhage during
surgery
. Some authors recommend the
routine use of tranexamic acid irrigation or
mouthrinses after surgery, alone or with aids
such as fibrin glue and oxidized cellulose mesh,
especially when INR values are 3.5 to 4, to help
blood clot formation before suturing.9 Other
new studies found that such measures are not
necessary to prevent bleeding complications
For post-operative pain
management, paracetamol with or withoutcodeine is recommended in patients on
oral anticoagulant therapy. NSAIDs should
be avoided as they may increase the risk
of post-operative bleeding in patients on
anticoagulants
Other anticoagulants
Medications such as low dose aspirin, clopidogril and dipyridamole areprescribed to prevent stroke and heart
attack. Aspirin and clopidogril irreversibly bind to the platelets and decrease their aggregation.
Patients are at risk of emboli and myocardial infarction if the antiplatelet
medication is stopped (stopping aspirin may increase the risk of thrombo-embolic events by 0.005%).
Studies have shown that patients undergoing simple minor oral surgery experienced minimal bleeding
complications when they continued on these medications (those bleeding
conditions were controlled with simple local measures).
These results indicated that low dose aspirin, clopidogril and dipyridamole
may be continued if a patient requires minor oral surgery.
For complicated oral surgery procedures, the antiplatelet medication can be stopped one week before the
surgery after consultation with the patient’s
physician.
NSAIDs also reversibly bind to the platelet for a limited period of time (approximately six hours). Hence,
there should be no major complications
if a patient is taking a NSAID drug.
Complications can arise if the patient is taking anticoagulant medication and NSAID.
Heparin
Heparin is administered subcutaneously or intravenously and isoften used for acute thrombo-embolic episodes or for hospitalization protocols
that include significant surgical procedures.
The effect of heparin is best assessed by the APTT. Heparin combines with antithrombin
III and the resulting complex inactivates several clotting factors in the coagulation cascade, but the most important steps are inhibition of the conversion of factor X to Xa and the antithrombin effect.
Heparin is rapidly removed from the blood and has an approximately 90 minute half-life.
Protamine sulphate reverses the effect of heparin and can be used in emergencies.
PT, APTT and thrombin times are therefore prolonged by the use of
heparin
. Most patients are monitored with the APTT and are maintained at 1.5 to 2.5
times the control value.Platelet counts should also be monitored if heparin is used
for more than 5 days because heparin can cause a thrombocytopenia.
Heparin is available as unfractionated heparin or low molecular
weight (LMW) heparin.
The anticoagulant effect of standard or unfractionated heparin has an immediate effect on blood clotting, which is usually lost within less
than six hours of stopping heparin.
Low dose heparin therapy may have little effect
either on the APTT or on post-operative bleeding.
LMW heparins have a longer duration of action but less effect on platelets, require less monitoring and
may have little effect either on the APTT
or on post-operative bleeding.
They are used primarily for prophylaxis of
post-operative deep vein thrombosis,
and there is no need to monitor APTT.
levels. When following recently published
recommendations, only about 1% of patientsexperienced a significant post-operative
bleeding episode.
All of these episodes were controllable with local measures.
For simple oral surgery procedures of 1–3 teeth, there is usually
no need to interfere with anticoagulant
treatment involving heparin or LMW
heparins or antiplatelet drugs. In more
complicated oral surgery cases, treatment is
best to be carried out in hospital.