Psychiatry
Lecture 22: DISSOCIATIVE DISORDERS/PERSONALITY DISORDERS
DISSOCIATIVE DISORDERS
Characteristics
1. The dissociative disorders are characterized by abrupt but temporary loss of memory
(amnesia) or identity, or by feelings of detachment owing to psychological factors.
2. Dissociative disorders are commonly related to disturbing emotional experiences in the
patient's recent or remote past.
3. Besides dissociative disorders, causes of amnesia include physiological factors, such as head
injury, substance abuse, sequela of general anesthesia, and dementia.
Classification and treatment
The
DSM-IV-TR categories of dissociative disorders are listed in the table below.
Treatment of the dissociative disorders includes hypnosis and drug-assisted interviews as well
as long-term psychoanalytically oriented psychotherapy to recover "lost" (repressed)
memories of disturbing emotional experiences.
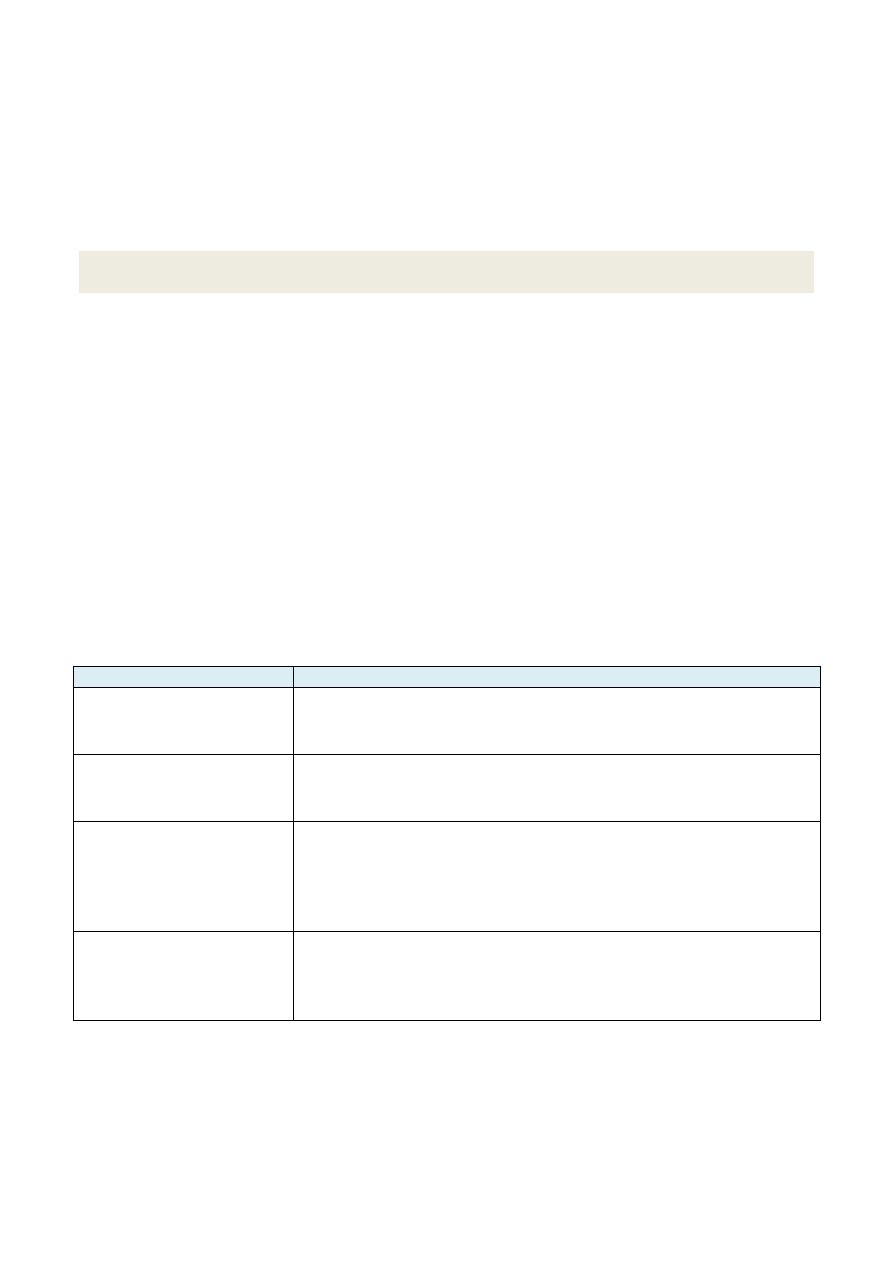
DSM-IV-TR Classification and Characteristics of Dissociative Disorders
Classification
Characteristics
Dissociative amnesia
Failure to remember important information about oneself after a
stressful life event
Amnesia usually resolves in minutes or days but may last years
Dissociative fugue
Amnesia combined with sudden wandering from home after a
stressful life event
Adoption of a different identity
Dissociative identity
disorder
(formerly multiple
personality
disorder)
At least two distinct personalities ("alters") in an individual
More common in women (particularly those sexually abused in
childhood)
In a forensic (e.g., jail) setting, malingering and alcohol abuse must be
considered and excluded
Depersonalization disorder Recurrent, persistent feelings of detachment from one's own body,
the social situation, or the environment (derealization) when stressed
Understanding that these perceptions are only feelings, i.e., normal
reality testing
PERSONALITY DISORDERS
Characteristics
1. Individuals with personality disorders (PDs) show chronic, lifelong, rigid, unsuitable
patterns of relating to others that cause social and occupational problems (e.g., few friends, job
loss).
2. Persons with PDs generally are not aware that they are the cause of their own problems (do
not have "insight"), do not have frank psychotic symptoms, and do not seek psychiatric help.
Classification
1. Personality disorders are categorized by the Diagnostic and Statistical Manual of Mental
Disorders, Fourth Edition, Text Revision (DSM-IVTR) into clusters:
A (paranoid, schizoid, schizotypal);
B (histrionic, narcissistic, borderline, and antisocial);
C (avoidant, obsessivecompulsive,
and dependent);
and not otherwise specified (NOS) (passive-aggressive).
A person with a passive-aggressive PD procrastinates and is inefficient, and, while outwardly
agreeable and compliant, is inwardly angry and defiant.
2. Each cluster has its own hallmark characteristics and genetic or familial associations (e.g.,
relatives of people with PDs have a higher likelihood of having certain disorders)
3. For the DSM-IV-TR diagnosis, a PD must be present by early adulthood. Antisocial PD cannot
be diagnosed until age 18; prior to this age, the diagnosis is conduct disorder.
Treatment
1. For those who seek help, individual and group psychotherapy may be useful.
2. Pharmacotherapy also can be used to treat symptoms, such as depression and anxiety, which
may be associated with the PDs.
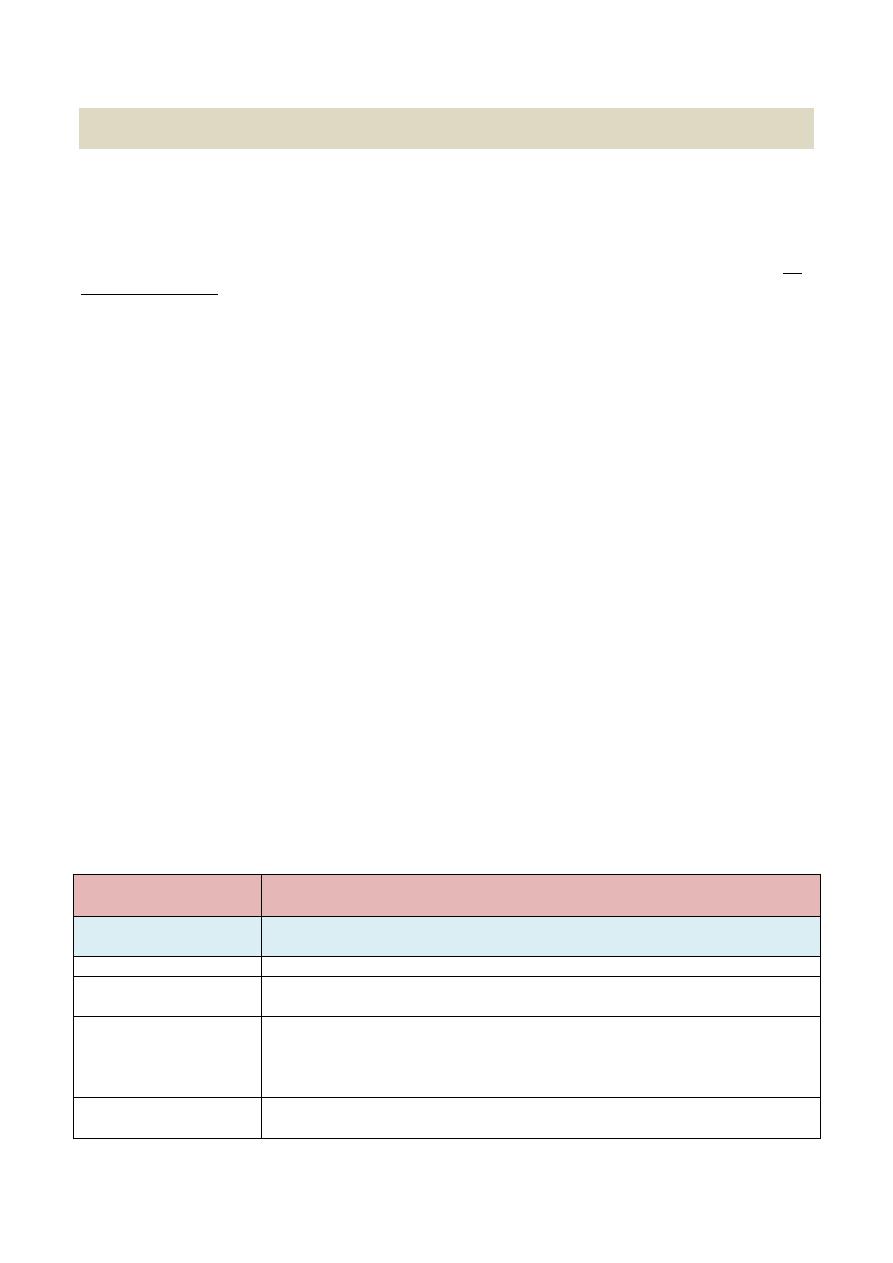
DSM-IV-TR Classification and Characteristics of the Personality Disorders
Personality
Disorder
Characteristics
Cluster A
Hallmark:
Avoids social relationships, is "peculiar" but not psychotic
Genetic or familial
association:
Psychotic illnesses
Paranoid
Distrustful, suspicious, litigious
Attributes responsibility for own problems to others
Interprets motives of others as malevolent
Collects guns
Schizoid
Long-standing pattern of voluntary social withdrawal
Detached; restricted emotions; lacks empathy, has no thought disorder
Schizotypal
Peculiar appearance
Magical thinking (i.e., believing that one's thoughts can affect the course of
events)
Odd thought patterns and behavior without frank psychosis
Cluster B
Hallmark:
Dramatic, emotional, inconsistent
Genetic or familial
association:
Mood disorders, substance abuse, and somatoform disorders
Histirionic
Theatrical, extroverted, emotional, sexually provocative, "life of the party"
Shallow, vain
In men, "Don Juan" dress and behavior
Cannot maintain intimate relationships
Narcissistic
Pompous, with a sense of special entitlement
Lacks empathy for others
Antisocial
Refuses to conform to social norms and shows no concern for others
Associated with conduct disorder in childhood and criminal behavior
in adulthood ("psychopaths" or "sociopaths")
Borderline
Erratic, impulsive, unstable behavior and mood
Feeling bored, alone, and "empty"
Suicide attempts for relatively trivial reasons
Self-mutilation (cutting or burning oneself)
Often comorbid with mood and eating disorders
Mini-psychotic episodes (i.e., brief periods of loss of contact with reality)
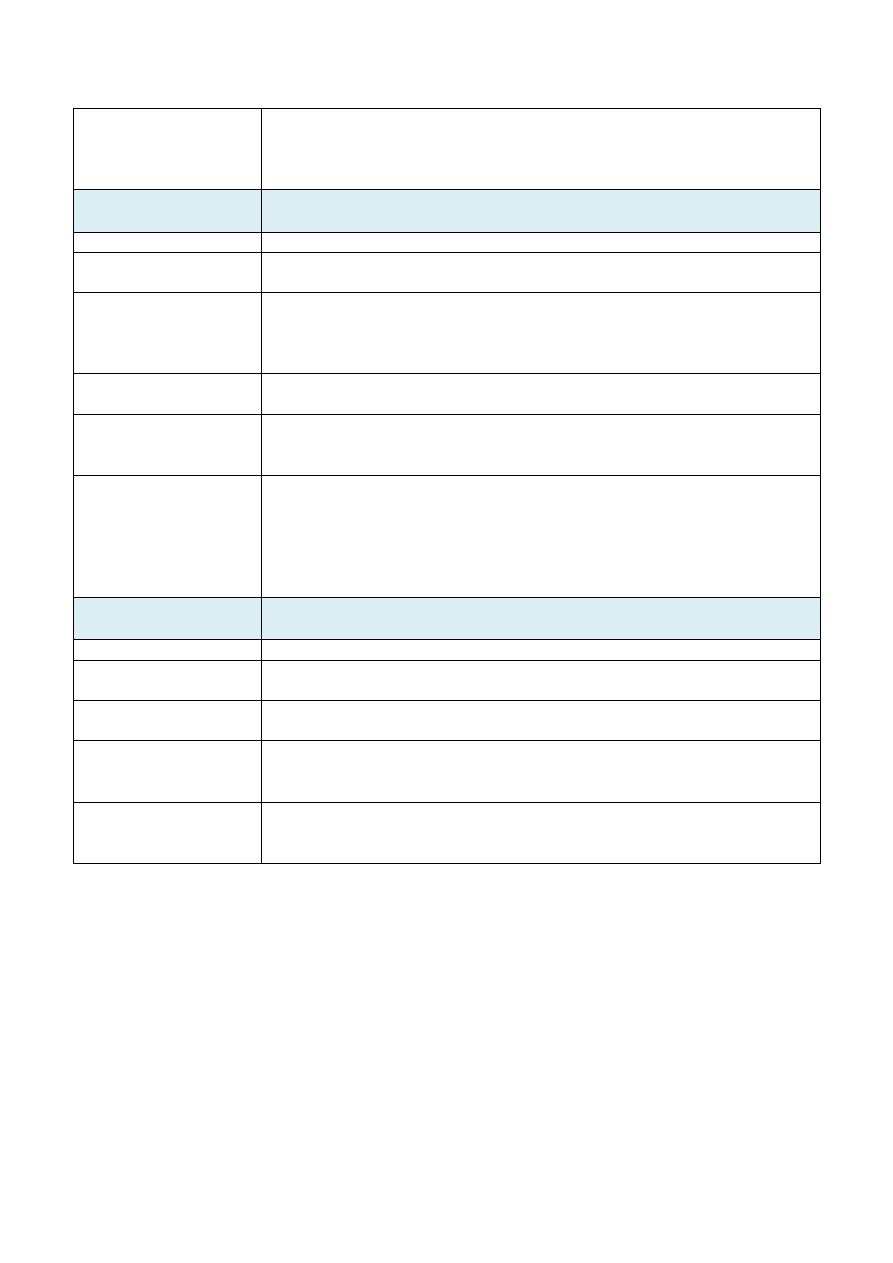
Cluster C
Hallmark:
Fearful, anxious
Genetic or familial
association:
Anxiety disorders
Avoidant
Sensitive to rejection, socially withdrawn
Feelings of inferiority
Obsessive-compulsive Perfectionistic, orderly, inflexible
Stubborn and indecisive
Ultimately inefficient
Avoidant
Allows other people to make decisions and assume responsibility for them
Poor self-confidence, fear of being deserted and alone
May tolerate abuse by domestic partner
The End