
2
Canine Impaction
by
Dr. Zaid Al-Dewachi

Introduction
Canine play an important role in esthetics, being
corner tooth of mouth and function deserves
special attention for its impaction to be properlydiagnosed and managed.
5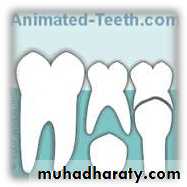

Assesment of
tooth eruptionTooth
development
Dental age
3/4th root
completion teeth
appears in arch
Nolla and
Moores havegiven charts
Normal tooth eruption
6



Impaction
IMPACTUS (latin origin) = pushed against
Archer (1975) defines impacted tooth as one
which is completely or partially unerupted and ispositioned against another tooth or bone or soft
tissue so that its further eruption is unlikely.
Impaction
According to Shafer, Hine and Levy, Impacted teeth are those which are
prevented from erupting by somephysical barrier in the eruption
path.
Or
When the crown remains at some
distance from the alveolar crestafter its scheduled eruption time
because of insufficient room or an
ectopic eruption pattern.
8
Impacted canine
Impaction of maxillary andmandibular canines is a
frequently encountered
clinical problem.
Third molars are the most
commonly impacted teeth
and canines stood
second.
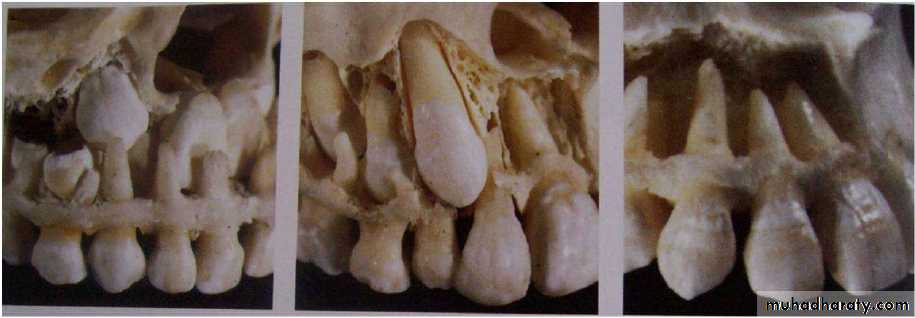
ERUPTION OF CANINE
Eruption of canine :
According to Broadbent, AO 1941-
Development of canine :
• It develops at 4 – 5 months of age between theroots of deciduous 1st molar.
Calcification of canine :
• It begins to calcify around 12 months of age.• Calcification is taking place far above the roots of
deciduous molar, allowing development of thefirst premolar between the deciduous molar roots.
11

At this stage the permanent
canine is located
immediately above both the
erupting first premolar and
the erupted first deciduous
molar.
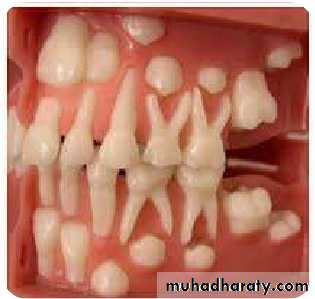
As the deciduous teeth
erupts towards the occlusal
plane, the permanent
incisor and canine crypts
migrate forward in the jaws.
The positional changes
between 8 and 10 years ofage need careful
observation for detection of
12
During this stage of development the
canine normally migrates buccally from aposition lingual to the root apex of the
deciduous precursor; however, some
canines do not make the transition from
the palatal to the buccal side of the dental
arch and remain palatally unerupted.
With sufficient increase in the size of the
subnasal area, the maxillary caninenormally moves downward, forward and
laterally away from the root of the lateral
incisor.
Between 8 and 12 years of age, the 'ugly
duckling' stage, there is insufficient spaceat the apical base to permit the axis of the
13
In the final phase of eruption, canines drive
their way between the lateral incisors andfirst premolars, forcing these teeth to
become more upright.
14
Factors governing eruption of
canine
Four factors govern the
eruption of permanent caninesinto normal position
1.
2.
3.
4.
Position of tooth bud in bony
crypt
Path of eruption
Shape and position of lateralincisors
Amount of space available
for canines in the arch15


Incidence
Dachi and Howell (1961) reported that theincidence of maxillary canine impaction is
0.92%, and mandibular canine impaction is
0.35%
Asians present more of buccal canine
impactions.
Impactions are twice as common in
females (1.17%) as in males (0.51%).
Of all patients with maxillary impacted
canines, it is estimated that 8% have
bilateral impactions.
Maxillary canine
Mandibular canineBuccal
Palatal
Lingual
Buccal
Classification of impacted canine
Impacted canine
19Classification of palatally impacted
canine Based on two variables:
(1). Transverse relationship of the crown of the
tooth to the line of dental arch which may be(a) Close
(b) Distant (nearer the midline)(2). Height of the crown of the teeth in relation
to the occlusal plane which may be(a) High
(b) Low20

Group 1
Proximity to the line of arch – close.Position in the maxilla – low.
Group 2Proximity to the line of arch – close.
Position in the maxilla – forward , lowmesial to the lateral
&
incisor root.
21

Group 3
Proximity to the line of arch –close.
Position in the maxilla – high.Group 4
Proximity to the line of arch –
distant.

Group 5
Canine root apex mesial to that of lateralincisor or distal to that of first premolar.
Group 6Erupting in the line of arch in place and
resorbing the roots of incisors.23
Classification by ACKERMAN and FIELDS in 1935.
IMPACTED CANINEHorizontally
Vertically
Palatal
Above
Labial
Below
Mid- alveolar
(With respect to the arch)
(With respect to the apex)(JCO 1979 DEC)
24
Etiology
Maxillary canines erupt bilaterally whereanterior and posterior regions of maxillary
arch intersect, these osseous structures
have different embryologic origins
Ant. Maxilla is derived from Ant. Nasal bud
and Post. Maxilla is formed by fusion ofMaxillary buds
The follicles of maxillary canine are located
at the mesial of the pre maxillary sutureduring periods of active growth.
Any deviation in or disturbance of that
osseous growth can provoke a change inorientation of canine tooth buds.
26
Etiology of impacted canine
• LOCALIZED• SYSTEMIC
• GENETIC27




LOCALIZED
Tooth size- arch lengthdiscrepancies
Failure of the primary canine
root to resorbProlonged retention or early
loss of primary canineAnkylosis of permanent canine
Cyst or neoplasm28


LOCALIZED
Dilaceration of the rootAbsence of maxillary lateral
incisorVariation in timing of lateral
incisor root formation
Iatrogenic factors
Idiopathic factors


SYSTEMIC
Endocrine deficienciesFebrile diseases
Irradiation
30



GENETIC
HeredityMalposed tooth germ
Presence of alveolar cleft
32
( Moyers concept summarized by Bishara)
• Moyers say that maxillary cuspid follows a
more difficult and tortous path of eruptionthan any other tooth.
• At age of 3 it is high in maxilla and its crown
directed mesially and lingually.• It moves toward occlusal plane gradually
uprighting itself until it seems to strike thedistal aspect of the root of the lateral incisor.
SAMIR BISHARA. AJO-DO Feb. 1992 & Semin Orthod June 1998
Theories put forth for impacted
canine Mc Bridge concept
Canine is formed high in the anterior wall at antrum,below the floor of orbit, long tortous path of eruption.
Tooth have much to travel from floor of orbit to oralcavity thereby had greater chances of “losing its way”
3
Becker 1984
He noted that there appear to be two processes for
palatal displacement of maxillary cuspid1.
2.
Developmental: due to absence of guidance of
lateral incisor
It relates to more advanced period when tooth
moving down into a narrower part of alveolarprocess
35

Vonder Heydt concept
Total arch length of permanent teeth is initiallyestablished very early in life at the time of eruption of
first permanent molars.
Canine is larger and later erupting and considering
like a musical chair situation it may get impacted.36
Peck and peck concept:
1) Palatally impacted canine is an inherited trait occurs in
combination with tooth agenesis,tooth size reduction,
supernumery tooth and other ectopically positioned
tooth.
2) Bilaterally occuring phenomenon (17%)
3) Females affected more than males (1:3.2)4) Familial occurrence
So they concluded palatally impacted canine as dentalanomaly having GENETIC ORIGIN.
37
Guidance theory of Miller:
Normal eruption: canine usually have a more mesial
development path, which is guided downwardsapparently along the distal aspect of the lateral incisor
roots.
Miller (1963) and Bass (1967) reported that there
appeared to be an unusually high prevalence ofcongenitally missing lateral incisors associated with
palatally impacted canine teeth.
38
Vincent Kokich 2004
He said that labial impact of the maxillary canine is
due to either ectopic migration of the canine crown
over the root of lateral incisor or shifting of maxillary
dental midline causing insufficient space for the
canine to erupt.
41
Labial or lingual
malpositioningof impacted
tooth
Dentigerous
cyst formation
Migration of
neighbouring teeth
and loss of arch
length
Infection
particularly withpartial eruption
Internal resorption or
external root
resorption of impacted
or neighbouring tooth
Referred pain
Shafer et al.SEQUELAE OF IMPACTED
CANINE
42
Diagnosis
InspectionPalpation
Radiograp
hs
44
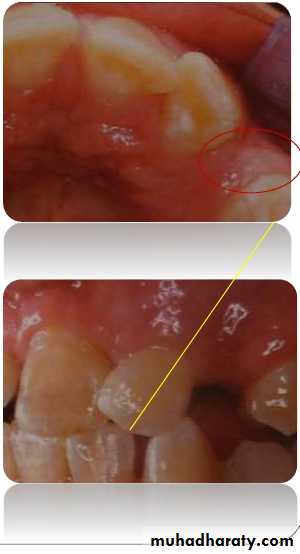
Inspection
Non-appearance of
permanent canine clinicallyby its eruption age.
Presence of antimere.
Presence of anterior spacing
for a long period.Persistent median diastema.
Abnormal morphology of
lateral incisor or presence of
peg laterals.
Improper angulations of
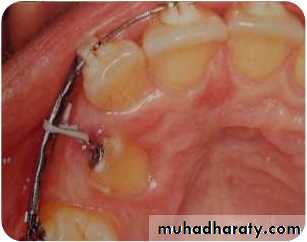
45Palpation
Bulge of permanent Canine could be palpatedbuccally above the deciduous canine 2-3 yrs
before its eruption.
It should be palpated deep above attached
gingiva in the sulcus where mucosa reflects. Deciduous canine should be checked for
mobility. Palpation should be done in abnormal
locations after getting clue from inspection.
46
Clinical Assessment of impacted
canine Determine patients dental age.
Assess the primary tooth its absence, colour,mobility, extent of root resorption.
Examine the morphology and thickness of
bony contour showing presence of labial orpalatal bulge.
Examine the cast to determine the arch shape
transverse and sagittal symmetry, intercaninedistance and lack of harmony between tooth
size and arch size.
47
Periapical
Mandibular archOPG
Lateral ceph
Extraoral
RADIOGRAPHS
I. Qualitative radiographs
Maxillary archOcclusal
PAview
Max. ant. occlusal
Parallax method
C T scanning48
True vertex/occlusal
II. 3-D localisation
Radiographic views at right angle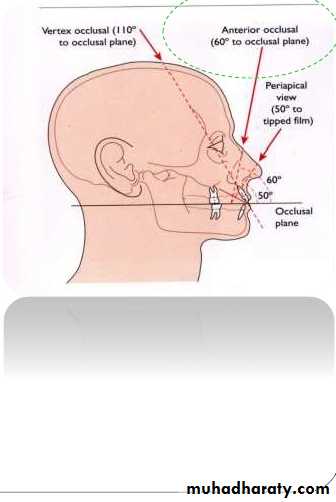
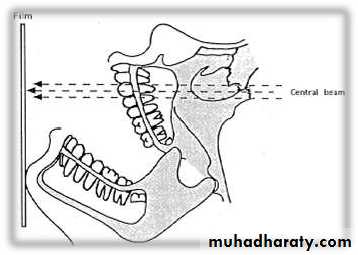
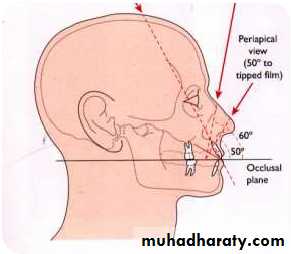
Occlusal radiograph
Provides a third i.e. horizontaldimension.
57x76 mm films are used.
Distoocclusal upper median film.
Central ray of x-ray is placed onthe median sagittal plane and
adjusted at an angle of 60-70 to
long axis of perm. max. canine.
It provides a topographic depiction
of palatal vault aiding inlocalization of palatally impacted
tooth.
Does not show exact cross
49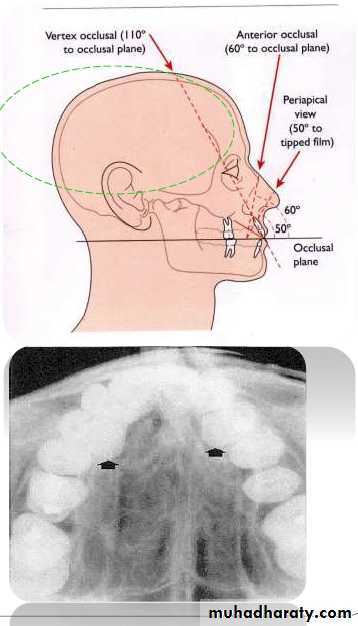
Occlusal radiograph
Maxillary true (vertex)occlusal
• X-ray beam runs parallel to
long axis of incisors.
• Possible to get cross section
of anteriors.
• Allows for bucco-lingual
position of impacted
canines or supernumerary
teeth irt to roots of incisors
50

Occlusal radiograph
Maxillary true (vertex)occlusal Ong’s projection
• Extra-oral technique for
vertex occlusal view• To increase clarity and
reduce exposure due to useof intensifying screen
Alternative technique to vertex/true occlusal view
Ong: AJO-DO, Volume 1994 Dec (621 - 626)
51
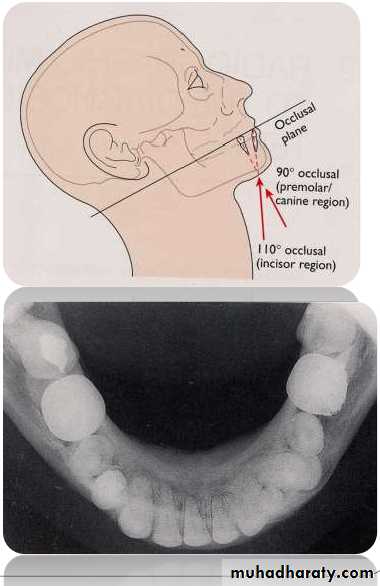
Occlusal radiograph
Mandibular occlusal900to OP – cross-section of
PM, molar region1100 to OP – cross-section of
incisor region
5
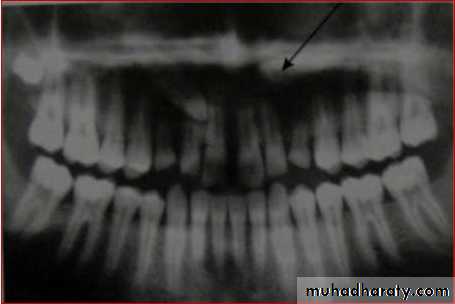
OPG
Panoramic radiographs are basic radiograph
for assessment of impacted teeth•
•
•
•
•
Tooth position whether deep or shallow
General orientation horizontal or inclined
mesially/distallyRelationship with neighbouring teeth
Risk of their transpositionPresence or absence of apical resorption of
roots of adjacent teeth
53
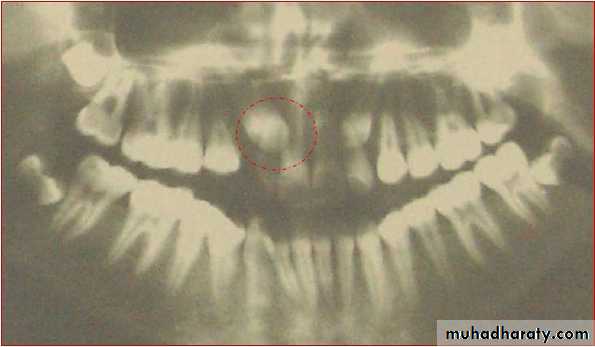
When mesio distal width of canine crown was
1.5 times larger (i.e. 15% larger) than theadjacent central incisor, then the canine is
palatally placed
This is only true in cases where canine should
not be at a higher level55
56
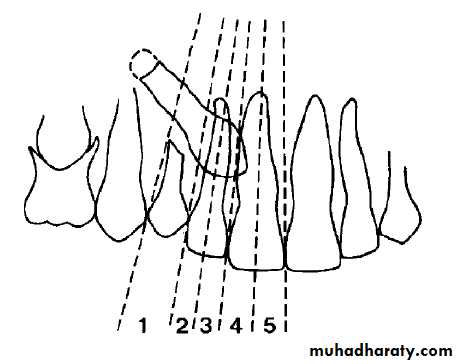
Ericson and Kurol in EJO 1988 defined number of
sectors to denote different types of impaction.
i.
ii.
Sector 1: if the cusp tip of the canine is
between the interincisor median line and the
long axis of the central incisor;
Sector 2: if the peak of the cuspid of the canine
is between the major axes of the lateral andcentral;
iii. Sector 3: if the peak of the cuspid of the canine
is between the major axis of the lateral and thefirst premolar.
The factors were:
1.2.
3.
4.
5.
6.
7.
Canine angulation to the midline;
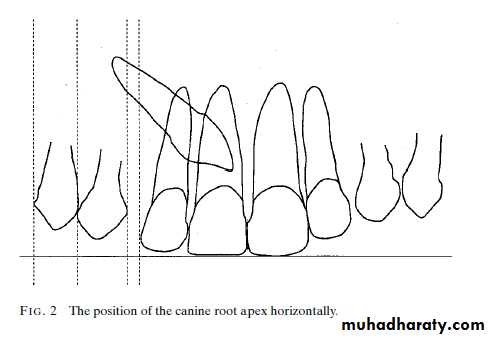
Vertical height of the canine crown;
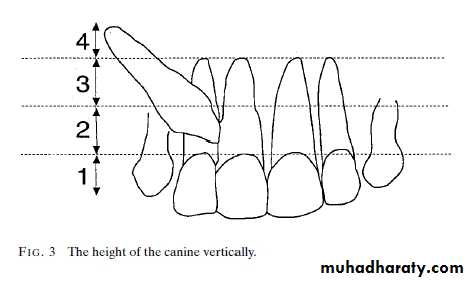
Antero-posterior position of the canine root
apex;
Canine crown overlap of the adjacent incisor;
Root resorption of adjacent incisor;Labio-palatal position of the canine crown;
Labio-palatal position of the canine apex.60
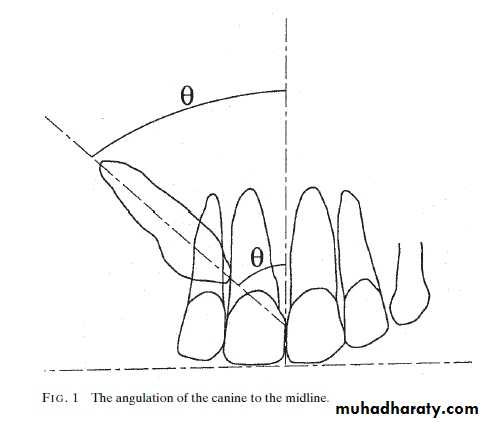
1.Canine angulation to the midline
Grade 1: 0–15°Grade 2: 16–30°
Grade 3 31°
61
2. Vertical Canine Crown Height
Grade 1: Below the level of the cemento-enameljunction (CEJ).
Grade 2: Above the CEJ, but less than half way up
the root.Grade 3: More than half way up the root, but less
than the full root length.Grade 4: Above the full length
of the root.
3. Position of Canine Root Apex Antero-posteriorly
Grade 1: Above the region of the canineposition.
Grade 2: Above the upper first premolar
region.Grade 3: Above the upper second premolar
region.63

4. Canine Overlap of the Adjacent Incisor Root
Grade 1: No horizontal overlap.Grade 2: Less than half the root width.
Grade 3: More than half, but lessthan the whole root width.
Grade 4: Complete overlap of rootwidth or more.
645. Presence of Root Resorption of the Adjacent
IncisorThe presence or absence of root resorption of the
adjacent upper incisor was recorded as judgedfrom examination of the OPG, although, a further
50 per cent of patients may have bucco-lingual root
resorption that is not diagnosed by routine
radiography (Ericson and Kurol, 1987).
65
Conclusion:
The orthodontists’ decision to expose or remove animpacted upper permanent canine, based on
radiographic information, seems to be primarily
guided by its labiopalatal position and it angulation
to the midline.
66

Lateral Cephalogram

Perapical view
First and the most simplest viewAdvantages
1) Root development, pattern and
integrity
2) Crown resorption
3) Root resorption of adjacent tooth
4) Minimum of surrounding tissue is
exposed which increase
accuracy and resolution.
5) Minimal radiation exposure
Disadvantage
1) 2D picture of 3D object
2) cannot determine bucco-lingual
position of tooth & vertical
position of impacted tooth.
69

70
the canine.
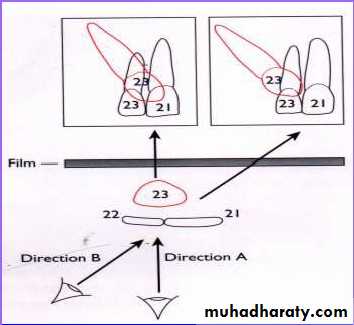
Tube shift technique or Clarke
technique (parallax method)
Principle:
• 2 periapical views of the same object are taken from slightlydifferent angles which can provide depth to the flat 2-D
picture depicted by each of the films individually.• Useful in distinguishing the buccal or lingual displacement of
Mesialangulation
Normal
angulation
Distal
angulation
Procedure:
1.In the periapical film, the X-rayis taken in the area of interest
with the X-ray beam passing
perpendicular to a tangent to
the line of arch at this point & at
an appropriate angle to
horizontal plane.
2.In the second film, the X-ray
tube is shifted mesially ordistally round the arch but held
at the same angle to the
horizontal plane. The X-ray
tube should describe between
30-450 of an arc of circle whose
72
Result:
• It is based on the SLOB principle.
• If the object has moved on the same side as thatof the X-ray tube it is lingually placed & if it has
moved on the opposite side it is on the buccalside.
Disadvantage:In cases when canine is highly placed, and
Periapical film shows no superimposition of canine
with the roots of erupted tooth or when

Vertical tube shift method
Left canine is highly placed in OPG. In IOPA left canine moves towards apical 1/3 of lateral
incisor.73
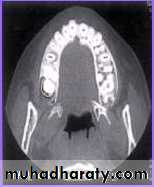



CT Scan
By Ericson & Kurol Used to diagnose the exact
position of an impacted tooth.
Clear serial radiographs may be
taken at graduated depth in any
part of human body in this
method.
This technique allows the
elimination of superimposition
of other structures.
It is however rarely used in the
diagnosis of impacted teeth
because of
(1) Large radiation dosage.
74
75
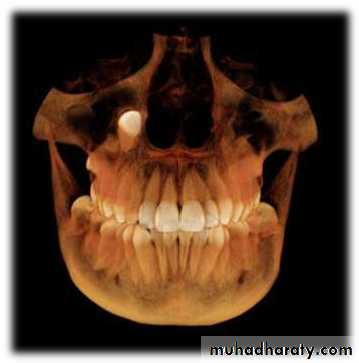
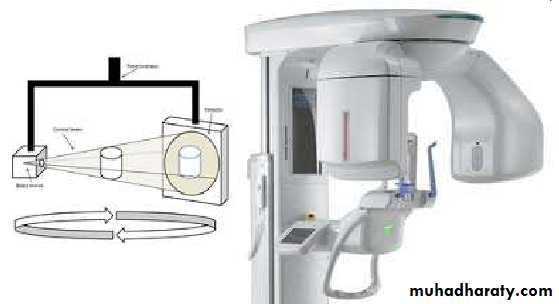
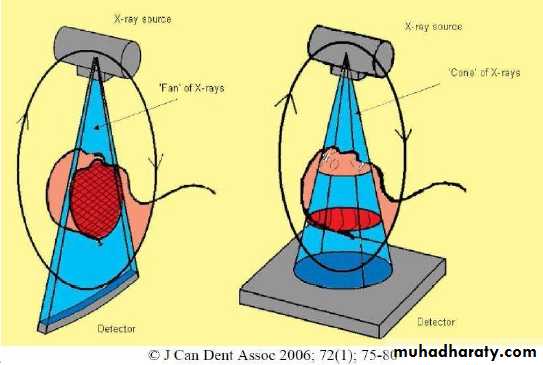
CBCT
Cone beam
computedtomography
(or CBCT, also
referred to as C-arm
CT, cone beam
volume CT, or flat
panel CT) is a
medical imaging
technique consisting
of X-ray computed
tomography where
the X-rays are

conventional radiography does
information.76
not provide sufficient
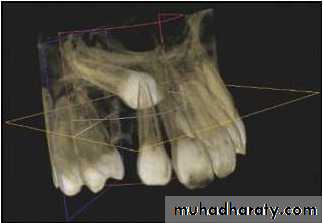
CBCT
CBCT is more accurate than
conventional techniques inlocalising impacted maxillary
canines.
CBCT is more reliable than
conventional techniques There is no robust evidence
that supports using CBCT as
the first line imaging technique.
We should only use it when
Cone-beam computed tomography vs conventional radiography in visualization
of maxillary impacted-canine localization: A systematic review of comparativestudies. Ehsan Eslami et al. Am J Orthod Dentofacial Orthop 2017;151:248-58
78
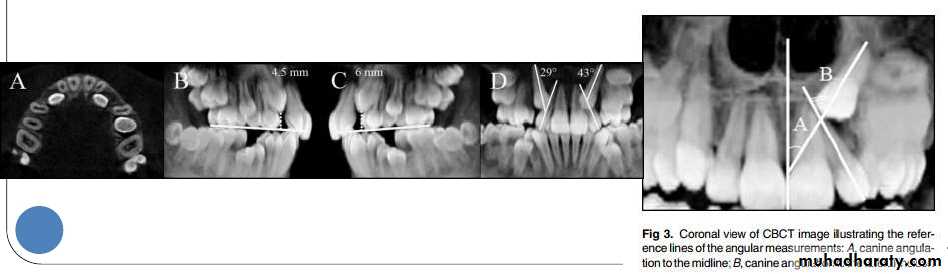
A study was done by Ali Alqerban et al AJODO March
2015, to compare 3D CBCT images of unilaterally
impacted canines with the normal contralateral sides,
and to detect possible radiographic factors involved in
maxillary canine impaction.
Prediction of the probability of canine impaction based
on CBCT was excellent. The canine angulation to the
lateral incisor on the coronal view, the canine cusp tip to
the occlusal plane on the sagittal view, and the canine
crown position were the strongest predictors based on
the CBCT radiographs and may help orthodontists to
identify the probability of impaction for optimally timing
the intervention.


Cone-beam computed tomographyand the orthosurgical management of impacted
teethCBCT imaging can be used to interpret buccolingual
information in detail, to distinguish and define the extent and
depth of root resorption, and to delineate long-axis orientation
of unerupted teeth, including root apex location. It is able to
synthesize traditional panoramic and cephalometric
radiographs. permits oral surgeons to visualize the position
and surgical anatomy of the tooth as it will be seen in the
operating theater and allows orthodontists to plan directional
traction.
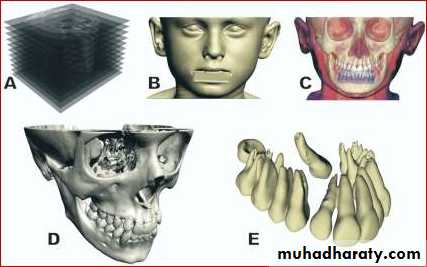
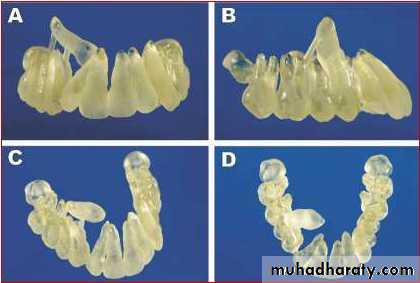
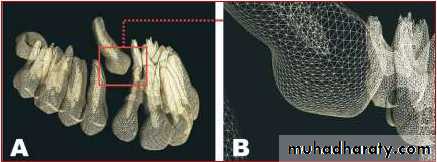
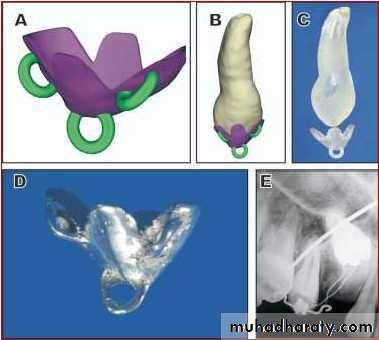
Rapid Prototyping
A new method for diagnosis and treatmentplanning of maxillary canine impaction.
Rapid prototyping' is a group of techniques
used to quickly fabricate a scale model of aphysical part or assembly using three-
dimensional computer aided design (CAD)
data.
Rapid prototyping as a tool for diagnosis and treatment planning for maxillary canine
Jorge Faber, Patrícia Medeiros Berto, and Marcelo Quaresma, AJODO 2006;129:583
80
81
PROGNOSIS
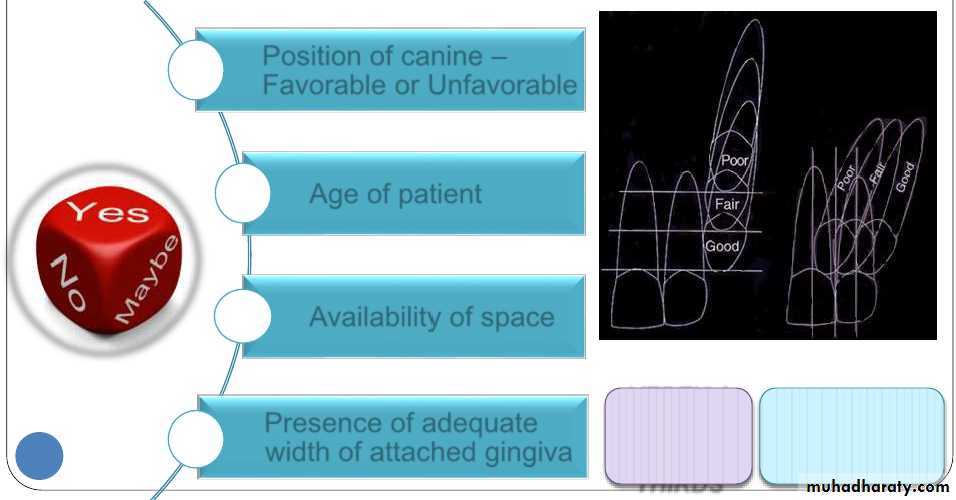
Determining the Prognosis
Factors influencing the treatmentdecision of an impacted canine
Position of canine –
Favorable or UnfavorableAge of patient
Availability of space
Presence of adequate
width of attached gingiva
VERTICA
L RULE
OF
THIRDS
HORIZONTAL
RULE OF
THIRDS
Treatment alternatives
1. No treatment, if the patient does not desire it.Since the long term prognosis of deciduous canine
is poor as its root may eventually resorb , it shouldbe periodically evaluated.
2. Auto transplantation of the canine.3. Extraction of impacted canine and moving
premolar in its position.4. Extraction of the canine & posterior segmental
osteotomy to move the buccal segment mesially to
close the residual space.
84